Effect of Combining Acupuncture and Functional Training on Post-stroke Functional Impairment of Hand
2013-07-18NiHuanhuanCuiXiaoHuYongshanWuYiHuangDequanQuPeiyuWangJunWuJiShiJunchao
Ni Huan-huan, Cui Xiao, Hu Yong-shan, Wu Yi, Huang De-quan, Qu Pei-yu, Wang Jun, Wu Ji, Shi Jun-chao
1 Department of Rehabilitation Medicine, Tianshan Hospital of Traditional Chinese Medicine of Changning District, Shanghai, Shanghai 200051, China
2 Department of Rehabilitation Medicine, Huashan Hospital Affiliated to Fudan University, Shanghai 200030, China
Effect of Combining Acupuncture and Functional Training on Post-stroke Functional Impairment of Hand
Ni Huan-huan1, Cui Xiao1, Hu Yong-shan2, Wu Yi2, Huang De-quan1, Qu Pei-yu1, Wang Jun1, Wu Ji1, Shi Jun-chao1
1 Department of Rehabilitation Medicine, Tianshan Hospital of Traditional Chinese Medicine of Changning District, Shanghai, Shanghai 200051, China
2 Department of Rehabilitation Medicine, Huashan Hospital Affiliated to Fudan University, Shanghai 200030, China
Objective: To observe the clinical effect of combining acupuncture and functional training on post-stroke functional impairment of hand.
Methods: A total of 165 cases who met the inclusion criteria were randomized into a treatment group (85 cases) and a control group (80 cases). Cases in the treatment group were treated with routine acupuncture points plus Shixuan (EX-UE 11) and Xiaohai (SI 8), whereas cases in the control group were treated with routine acupuncture points alone. After acupuncture, cases in both groups conducted functional training in upper limbs. The finger grip strength and hand function were assessed before and after 3-course treatment.
Results: Cases in the treatment group obtained better finger grip strength and hand function than those in the control group (bothP<0.05).
Conclusion: In addition to functional training, adding Shixuan (EX-UE 11) and Xiaohai (SI 8) to traditional acupuncture formulae works better for post-stroke functional impairment of hand.
Acupuncture Therapy; Electroacupuncture; Stroke; Complications
Stroke is a common medical emergency that can cause a high disability rate. Stroke survivors often experience functional impairment of limbs, especially the hands. Due to fine movements and a larger projection area in the cerebral cortex, it is extremely difficult to restore the hands function after stroke. Statistical results have shown that 96.4% of stroke patients lost their hand function 3 months following stroke[1]. Since functional impairment of hand can severely affect the patient’s performance in activities of daily living (ADL), functional recovery of hand can be a decisive factor in patient’s quality of life. We addressed this problem by adding Shixuan (EX-UE 11) and Xiaohai (SI 8) to routine acupuncture points. The results of combining acupuncture and functional training are now reported as follows.
1 Clinical Materials
1.1 Diagnostic criteria
1.1.1 Diagnostic criteria in Western medicine
This is based on theKey Points in Diagnosing Cerebrovascular Diseasesstipulated in the 4th National Academic Conference on Cerebrovascular Diseases in 1995[2], coupled with cerebral infarction or hemorrhage confirmed by cranial CT or MRI scan. The latest attack is considered as the target in the recurrent cases.
1.1.2 Diagnostic criteria in Chinese medicine
This is based on theShanghai Diagnostic and Therapeutic Guidelines of Traditional Chinese Medicine[3]and all patients were diagnosed with stroke of meridians.
1.2 Inclusion criteria
Those who met the diagnostic criteria; duration of cerebral infarction or hemorrhage ≤1 month; having signed informed consent; having stable vital signs; Glasgow coma scale (GCS) score >8; aged between 40 and 79; inability to move hand following stroke.
1.3 Exclusion criteria
Traumatic conditions of the affected hand/peripheral nerve injury; active liver disease, the liver or kidney insufficiency, congestive heart failure, malignant tumor; malignant progressive hypertension, respiratory failure; having a history of dementia or mental disorders; >1 month of hemorrhagic or ischemic stroke; dropped out during the observation.
1.4 General data
A total of 165 stroke inpatients from Department of Rehabilitation Medicine, Tianshan Hospital of Traditional Chinese Medicine of Changning District, Shanghai were randomly allocated into a treatment group of 85 cases and a control group of 80 cases. There were no statistical differences in gender, age, duration, stroke category and affected parts (P>0.05), indicating that the two groups were comparable (table 1).

Table 1. Between-group comparison of general data
2 Treatment Methods
2.1 Treatment group
Major acupoints: Shixuan (EX-UE 11), Xiaohai (SI 8), Quchi (LI 11), Shousanli (LI 10), Waiguan (TE 5), Zhongzhu (TE 3) and Hegu (LI 4).
Adjunct acupoints: Combine with Baxie (EX-LE 3) for back of hand swelling.
Method: After routine disinfection, punctured above points using disposable filiform needles. Punctured Shixuan (EX-UE 11) perpendicularly using filiform needles of 0.32 mm in diameter and 25 mm in length, and retained the needles for 20 min; punctured Xiaohai (SI 8) obliquely (45°-60°) to produce an electric shock/numb sensation that radiated towards the fingers; punctured the other acupoints perpendicularly using filiform needles of 0.32 mm in diameter and 40 mm in length, 1-1.5 cun for Quchi (LI 11) and Shousanli (LI 10), 0.5-1 cun for Waiguan (TE 5) and Zhongzhu (TE 3), and 0.5-1 cun from Hegu (LI 4) towards Houxi (SI 3); and then manipulated needles by twisting, lifting and thrusting, 1 min for each acupoint and connected Xiaohai (SI 8) and Waiguan (TE 5) with G6805-II electric stimulator, using discontinuous wave, a frequency of 2 Hz and an intensity within the patient’s tolerance, which could induce finger abduction.
2.2 Control group
Major acupoints: Quchi (LI 11), Shousanli (LI 10), Waiguan (TE 5), Zhongzhu (TE 3) and Hegu (LI 4).
Adjunct acupoints: The adjunct acupoints are same as the treatment group.
Method: After routine disinfection, punctured above points using disposable filiform needles of 0.32 mm in diameter and 40 mm in length; and then connected Quchi (LI 11) and Waiguan (TE 5) with G6805-II electric stimulator, using discontinuous wave, a frequency of 2 Hz and an intensity within the patient’s tolerance.
Functional training was done 6 times each week. Acupuncture was conducted once every other day and 5 times constituted a course of treatment. The therapeutic efficacies were observed after 3 courses of treatment.
3 Therapeutic Efficacy Observation
3.1 Observation indexes
3.1.1 Scoring of finger grip strength
This is based on the finger grip strength scoring system[4]for neurological deficit in the 1995 China stroke scale.
0: Grade V, normal.
1: Grade IV, inability to clench a fist.
2: Grade III, a hollow fist with finger extension.
3: Grade III, finger flexion but no extension.
4: Grade II, limited finger flexion (can’t touch the palm).
5: Grade I, slight moving of the fingers.
6: Grade 0, inability to move fingers at all.
3.1.2 Scoring of hand function
The hand and wrist functions were assessed using Fugl-Meyer assessment (FMA) scale[5], which contains 3 major domains and 15 sub-items. The maximum score for each sub-item is 2 and the sum of the score is 30.
The above assessments were made during recruitment (V1) and after 3 courses of treatment (V2) by experienced rehabilitation therapists who were not involved in the grouping and treatment.
3.2 Criteria of therapeutic efficacy
Recovery: Grade IV-V of finger grip strength.
Marked effect: Grade III of finger grip strength.
Improvement: Grade I-II of finger grip strength.
Failure: Grade 0 of finger grip strength.
3.3 Statistical method
The SPSS 10.0 version software was used for statistical analysis,t-test for measurement data and Chi-square and Mann-Whitney U test for ranked data.
3.4 Results
3.4.1 Observation of finger grip strength
As shown in table 2, there was a statistical difference in the finger grip strength between two groups (P<0.05), indicating that patients in the treatment group had better finger grip strength than those in the control group.
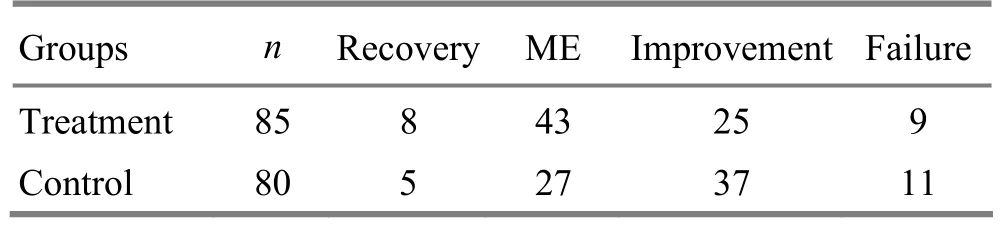
Table 2. Between-group therapeutic efficacy comparison in finger grip strength (case)
3.4.2 Observation of hand function
As shown in table 3, there was no statistical difference in hand motor function between two groups (P>0.05). After treatment, there were before-after statistical differences in the hand function in both groups (P<0.01) and a between-group statistical difference in the hand function scoring (P<0.05).
Table 3. Comparison of hand function scores before and after treatment in the two groups (, point)
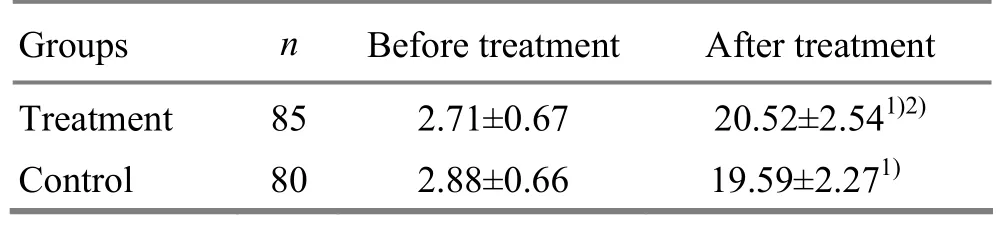
Table 3. Comparison of hand function scores before and after treatment in the two groups (, point)
Note: Intra-group comparison, 1)P<0.01; inter-group comparison, 2)P<0.05
GroupsnBefore treatment After treatment Treatment 85 2.71±0.67 20.52±2.541)2)Control 80 2.88±0.66 19.59±2.271)
4 Discussion
To date, acupuncture has been extensively used for rehabilitation of post-stroke limb paralysis. Numerous studies have proven that acupuncture can benefit recovery of the paralytic limbs, alleviation of sequela and performance in ADL[6-10]. Acupoints of the Three Yang Meridians of Hand, especially the Yangming (Large Intestine) Meridian is commonly used for functional recovery of upper extremities, since Yangming Meridians are full of qi and blood and therefore indicated for Wei-Flaccidity syndrome in Chinese medicine, including loss of hand function following stroke. Quchi (LI 11), Shousanli (LI 10) and Hegu (LI 4) can lubricate joints, circulate blood and unblock collaterals. As one of the Confluent Points of the Eight Extraordinary Meridians, Waiguan (TE 5) connecting with the Yang Link Vessel, can regulate qi of the six yang meridians and improve weakness or paralysis of the upper limbs[11-13].
Functional impairment of fingers is a most common symptom in stroke patients. Since the fine movements of fingers can be a key factor in determining a stroke patient’s quality of life, this study selected Shixuan (EX-UE 11) to improve the treatment effect. One of the Shixuan points, Zhongchong (PC 9), is also a Jing-Well acupoint. Other Shixuan (EX-UE 11) are also located close to Jing-Well acupoints. Literally meaning the origin of water/meridian-qi, these Jing-Well acupoints have been believed by physicians in different generations to unblock meridians and resolve Bi-Impediment syndrome[14]. As a result, they are often used for disturbed or blockage of qi circulation such as stroke or collapse. Anatomically, Shixuan (EX-UE 11) locate around the arterial and venous network, nerves and pain receptors. Needling Shixuan (EX-UE 11) can directly stimulate the peripheral nerve, enhance the vasomotor function and increase the arterial/venous blood flow, thus improving the finger functions. Xiaohai (SI 8) is the He-Sea acupoint of the Small Intestine Meridian and full of meridian qi. In addition, it is located in the ulnar groove innervated by the medial antebrachial cutaneous nerve and ulnar nerve stem. Needling this point can produce a strong sensation that radiates from the elbow to fingers and rapidly activate meridian qi, thus benefiting the forearm, wrist and fingers.
This study has suggested that combining acupuncture and functional training can enhance the recovery of hand function following stroke; adding Shixuan (EX-UE 11) and Xiaohai (SI 8) to traditional acupuncture formulae can improve the treatment effect and obtain a better result in hand function recovery than traditional acupuncture therapy.
[1] Wang MB. Modern Assessment and Treatment for Hemiplegia. Beijing: Huaxia Press, 1990: 142-143.
[2] Chinese Neuroscience Society, Chinese Neurosurgical Society. Key diagnostic points for cerebrovascular diseases. Zhonghua Shenjingke Zazhi, 1996, 29(6): 379-380.
[3] Shanghai Municipal Health Bureau. Shanghai Diagnostic and Therapeutic Guidelines of Traditional Chinese Medicine. 2nd Edition. Shanghai: Publishing House of Shanghai University of Traditional Chinese Medicine, 2003: 75-76.
[4] Chinese Society of Psychiatry. Clinical neurologic deficient severity scoring standard in stroke patients. Zhonghua Shenjingke Zazhi, 1996, 29(6): 381.
[5] Zhou WJ, Sun QL. Assessment Manual for Paralysis Rehabilitation. Beijing: People’s Medical Publishing House, 2006: 47-50.
[6] Sun YZ, Wang YJ, Wang W. Effect of acupuncture plus rehabilitation training on shoulder-hand syndrome due to ischemic stroke. J Acupunct Tuina Sci, 2012, 10(2): 109-113.
[7] Fan GQ, Zhang DB, Luo W. Acupuncture for Stroke. Shanghai: The Second Military Medical University Press, 2001: 209-263.
[8] Wu YC, Chai L. Effect of combined acupuncture and Chinese herbal formula on the motor function and activities of daily living in post-stroke patients. J Acupunct Tuina Sci, 2011, 9(5): 315-318.
[9] Li ZR. Experience in acupuncture treatment for post-stroke upper extremity disability. Shanghai Zhenjiu Zazhi, 2000, 19(1): 3-4.
[10] Li Y, Pang Y, Zhou ZC. Clinical study on kidney-nourishing and Governor Vessel-regulating acupuncture therapy for apoplexy sequela. J Acupunct Tuina Sci, 2007, 5(3): 156-159.
[11] Qian YJ, Chen T. Rehabilitation effect of combined acupuncture and mid-frequency computer for hand function impairment following brain injury. Shanghai Zhenjiu Zazhi, 2010, 29(10): 660-661.
[12] Li L, Zheng P, Chen X, Bai Y, Mao M. Clinical study on acupuncture and ischemic stroke. J Acupunct Tuina Sci, 2009, 7(3): 137-139.
[13] Li L, Yao L, Han LB. Observation on the clinical efficacy of balancing acupuncture plus kinesiotherapy for post-stroke shoulder-hand syndrome. Shanghai Zhenjiu Zazhi, 2011, 30(9): 607-608.
[14] Wang JY. Clinical experience in using Five-Shu points. Zhongguo Zhenjiu, 1983, 3(2): 23.
Translator: Han Chou-ping
Received Date: May 20, 2013
R246.6
A
in the two groups
the same medical treatment measures and rehabilitation care, including functional training of the upper extremities every day.
Author: Ni Huan-huan, attending physician
Cui Xiao, chief physician.
E-mail: cuixiao@163.com
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Clinical Study on Electroacupuncture for Cervical Intervertebral Disc Herniation
- Observation on Clinical Effects of Electroacupuncture Therapy for Apoplexy with Obstructive Sleep Apnea Syndrome
- Clinical Observation on Acupuncture Therapy for Depression at Perimenopause
- Therapeutic Efficacy Observation on Combining Herbal Cake-partitioned Moxibustion with Plumblossom Needle Therapy for Cervical Radiculopathy
- Therapeutic Observation on Swift Needling with Fire Needle plus Medication for Herpes Zoster
- Shu-Stream Points for Two Cases with Time-related Disease