Cholangiocarcinoma: principles and current trends
2011-07-07GeorgeZografosAthanasiosFarfarasFloraZagouriDimosthenisChrysikosandKostasKaraliotas
George N Zografos, Athanasios Farfaras, Flora Zagouri, Dimosthenis Chrysikos and Kostas Karaliotas
Athens, Greece
Review Article
Cholangiocarcinoma: principles and current trends
George N Zografos, Athanasios Farfaras, Flora Zagouri, Dimosthenis Chrysikos and Kostas Karaliotas
Athens, Greece
BACKGROUND:Cholangiocarcinoma (CCA) is a lethal cancer of the biliary epithelium, originating from the liver (intrahepatic), at the confluence of the right and left hepatic ducts (hilar) or in the extrahepatic bile ducts. It is a rare malignancy associated with poor prognosis.
DATA SOURCES:We searched the PubMed/MEDLINE database for relevant articles published from 1989 to 2008. The search terms used were related to "cholangiocarcinoma" and its "treatment". Although no language restrictions were imposed initially, for the full-text review and final analysis, our resources only permitted the review of articles published in English. This review deals with the treatment of cholangiocarcinoma, the principles and the current trends.
RESULTS:The risks and prognostic factors, symptoms and differential diagnosis are thoroughly discussed. In addition, the tools of preoperative diagnosis such as endoscopic retrograde cholangiopancreatography, digital image analysis, fluorescencein situhybridization and magnetic resonance cholangiopancreatography are reviewed. Moreover, the treatment of CCA is discussed.
CONCLUSIONS:The only curative treatment available is surgical management. Unfortunately, many patients present with unresectable tumors, the majority of whom die within a year of diagnosis. Surgical treatment involves major resections of the liver, pancreas and bile duct, with considerable mortality and morbidity. However, in selected cases and where indicated, appropriate management with aggressive surgery may achieve a good outcome with a prolonged survival expectancy.
(Hepatobiliary Pancreat Dis Int 2011; 10: 10-20)
cholangiocarcinoma; treatment; prognostic factors; risk factors; surgery
Introduction
Up to the late 1970s, cases of cholangiocarcinoma (CCA) affecting the confluence of the hepatic ducts were considered rare, difficult to diagnose and unresectable.[1]CCA is relatively uncommon with an annual incidence of 1-2 cases per 100 000 in the Western countries. However, rates have been rising worldwide over the past decades, partly due to advances in diagnostic techniques.[2,3]In addition, breakthroughs in operative techniques over the last decade have led to a dramatic change in approach; resection is now generally regarded as the best possible treatment.
CCA is a lethal cancer of the biliary epithelium and can develop anywhere along the biliary tree. Anatomically, CCAs are classified as intrahepatic when they develop in the liver, as hilar when they arise at the confluence of the right and left hepatic ducts, and as distal extrahepatic bile duct cancers. Based on their appearance, these tumors can be defined as mass-like, periductal, intraductal or mixed bile duct tumors which involve the hepatic duct bifurcation when they are known as Klatskin tumors (by the name of the author who first described this kind of hilar CCA in 1965). Bismuth-Corlette classified perihilar tumors into 4 subtypes (Table 1).
The histological types are listed in Table 2. Greater than 90% of bile duct cancers are well-differentiated and mucin-producing adenocarcinomas. Other types include squamous cell carcinoma, small cell carcinoma, and sarcoma. Macroscopically, adenocarcinomas of the bile duct are classified as sclerosing, nodular, or papillary (analogous to the classification scheme for gallbladder adenocarcinomas). Sclerosing (scirrhous)tumors comprising over 80% CCAs are associated with an intense desmoplastic reaction and a low resectability, and tend to be highly invasive. Nodular tumors show the appearance of constricting annular lesions and are also associated with a low resectability. Papillary tumors are rare and present as bulky masses that project into the bile duct lumen.
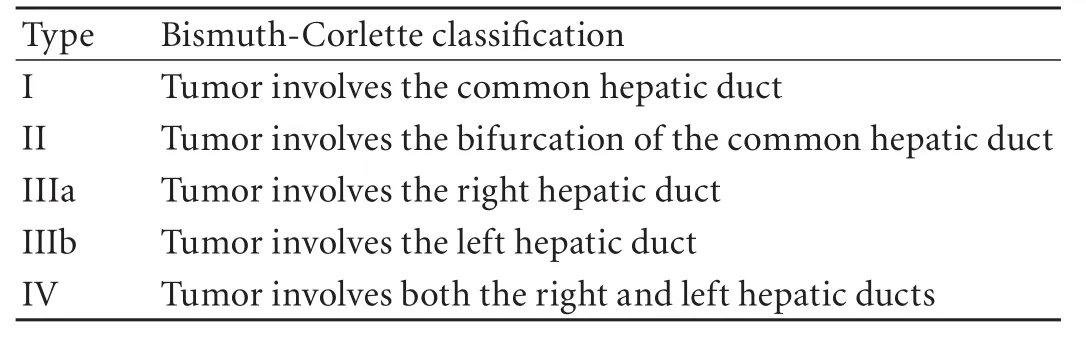
Table 1. The Bismuth-Corlette classification of perihilar tumors
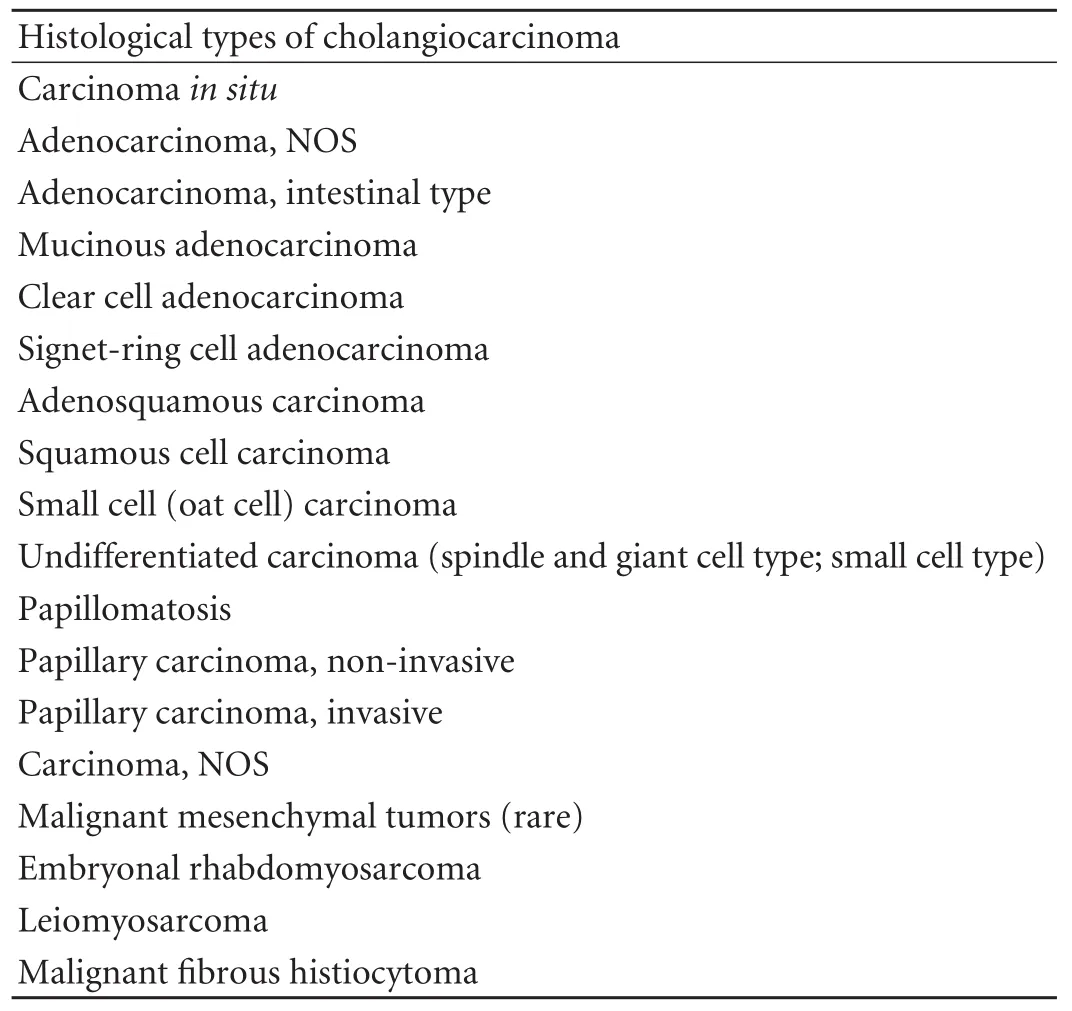
Table 2. Histological types of cholangiocarcinoma (extrahepatic)
There is no system that stratifies patients into subgroups for potential resectability and simultaneously correlates with survival. For extrahepatic (hilar and distal) CCA there are two systems for staging, the American Joint Committee on Cancer (AJCC) TNM (tumor, node, metastases) Staging System (Table 3) and the modified Bismuth-Corlette classification (Table 1). Intrahepatic CCAs are classified as hepatocarcinomas (Table 4).
The peak age for CCA is the seventh decade, with a slightly higher incidence in men. Despite its significant increase, the incidence of the disease remains low, with marked global variations. The highest rates are reported in northeast Asia where the disease affects 96 per 100 000 men. At about 100 times greater than that in the West, this rate presumably reflects differences in localrisk factors and genetics. Despite its low incidence, CCA is responsible for about 13% of primary liver cancers and accounts for 1.3% to 2.6% of annual cancer-related deaths worldwide.[4]
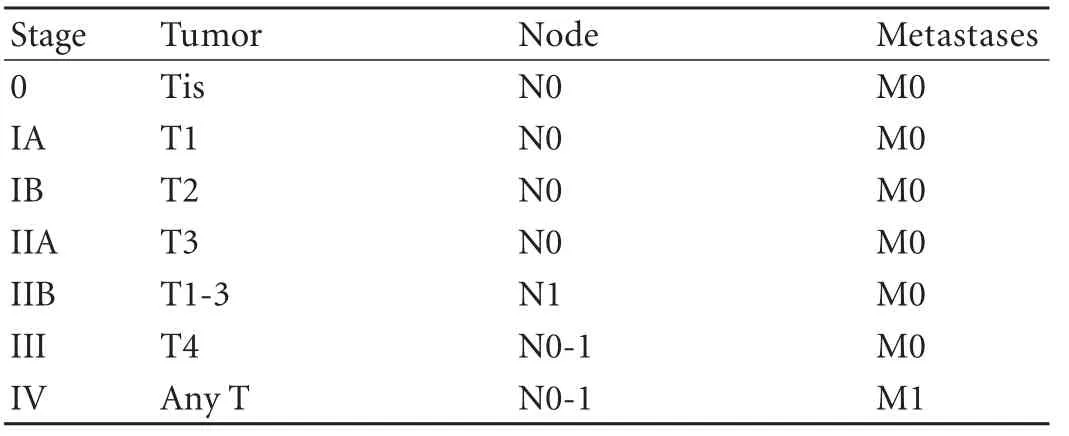
Table 3. TNM staging for extrahepatic cholangiocarcinomas
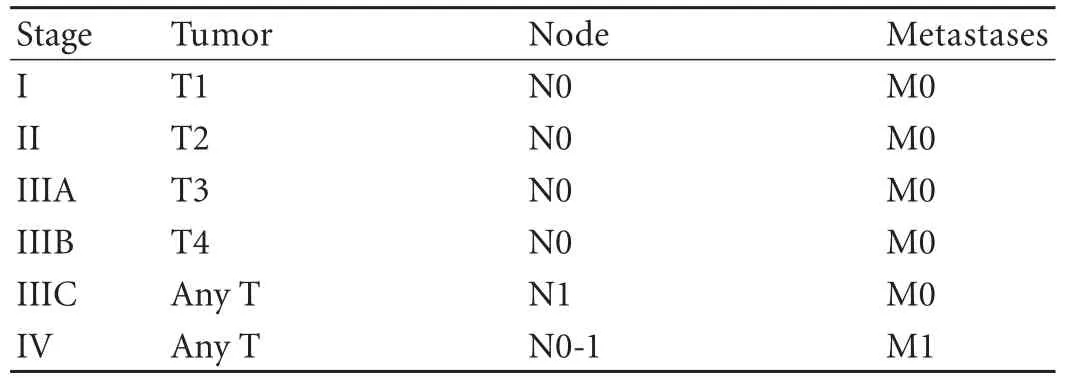
Table 4. TNM staging for intrahepatic cholangiocarcinomas
Surgical resection has been the mainstay of curative treatment for CCA. However, the operative mortality is high and the 5-year survival rate remains disappointing.[5]Most patients who undergo resection die of local tumor recurrence.[6]This is related to the fact that complete surgical resection with tumor-free histological margins is difficult to perform. It is seen only between 10% and 50% of resected specimens.[7]Surgery, frequently incorporating a major hepatic resection, is thus considered as palliative rather than curative.
Although surgical principles remain unchanged, significantly increased survival rates over the last decade, improvement in palliative and adjuvant management, and molecular insight into pathophysiology of thedisease have been conducive to a new approach to CCA. It is important to establish that surgery can be performed with relative safety and to define its optimal place in the overall management strategy.
Risk factors
Because of its sporadic nature, the etiology of CCA remains enigmatic and evaluation of risk factors poses a difficult puzzle. The most common predisposing factor for CCA is primary sclerosing cholangitis (PSC), which has been reported in up to 40% of patients suffering from a specific malignancy. Although it has been shown that the risk of development of CCA is higher within the first 2.5 years following diagnosis of PSC, no association has yet been established between the duration of PSC and the incidence of CCA.[4-8]In addition, patients with intrahepatic biliary stones have a 10% risk of developing CCA, while up to 70% of patients with histologically confirmed CCA have hepatolithiasis.[9-12]Moreover, biliary malformations such as Caroli's disease and congenital fibropolycystic disease carry a 10% to 15% risk of malignancy.[13]Liver fluke infection is another important risk factor for the development of CCA. Infection by Opisthorchis viverrini has been demonstrated as a definite cause of human CCA, whereas infection byClonorchis sinensishas been linked to a higher incidence of CCA.[14,15]Chronic pancreatitis, non-specific liver cirrhosis, history of biliary-enteric drainage for benign disease, exposure to environmental toxins, primarily including dioxins, increased body mass index and consumption of alcohol have also been associated with a higher prevalence of CCA.[16,17]Moreover, many hormones, neuropeptides, and neurotransmitters have been found to regulate malignant and non-malignant cholangiocyte pathways in patients with chronic biliary diseases.[18]
Hepatitis B (HBV) and hepatitis C (HCV) are established risk factors for hepatocellular carcinoma and their roles have been proposed in the development of CCA. Various studies have demonstrated a statistically significant increase of antibodies against HBV among CCA patients, while up to 30% of them have antibodies against HCV.[19,20]
Genetic and epigenetic changes play an integral role in the transfer of cholangiocytes to their malignant counterparts. Epigenetic gene silencing refers to non-mutational gene inactivation, mainly based on hypermethylation of promoter sequences. Hypermethylation has been shown to play a central role in the progression of tumor growth in almost all types of cancer, including CCA.[21]The hypermethylation and inactivation of a number of cell cycle inhibitors as well as the repression of many tumor suppressor genes have been shown to occur in up to 83% of patients with CCA.[22,23]In addition, inactivation of the tumor suppressor gene Semaphorin3B has been described as methylated in 100% of the studied cases.[24]Furthermore, inherited mutations that affect DNA repair genes have been strongly associated with a high CCA risk.[23]Inactivation of these genes allows cells to avoid apoptosis and to undergo unrestricted proliferation and may be vigorously involved in the pathogenesis of CCA.
A role is emerging for non-coding RNAs in the neoplastic transformation of cells. These microRNAs are gene-specific regulators that act as key regulators in numerous processes including cell proliferation, cell death and apoptosis and are associated with the development of malignancy in various tissues.[25,26]Increased activation of microRNAs, such as miR-141, miR-200b and miR-21 involved in circadian rhythm and tumor suppression, has been demonstrated in CCA patients, while a down-regulation of microRNAs processing antiapoptotic functions has also been noted. Alterations in microRNA expression may contribute to tumor growth by modulating the functional expression of critical genes involved in the development of CCA.[27,28]
The development of novel cell culture models of CCA could provide important research tools with which we investigate relevant cellular alterations and new possible risk factors that may be pertinent to human diseases. In addition, such models can serve as the basis for the preclinical testing of new therapeutic strategies. It is also remarkable that few human CCA cell lines now exist, and their availability has been limited.
Symptoms: differential diagnosis
Symptoms may include jaundice, clay-colored stools, bilirubinuria, pruritus, weight loss, and abdominal pain. Jaundice is the most common manifestation of bile duct cancer. The obstruction and subsequent cholestasis tends to occur early if the tumor is located in the common bile duct or common hepatic duct. Jaundice often occurs later in perihilar or intrahepatic tumors and is a marker of advanced disease. Abdominal pain is relatively common in advanced disease and is often described as a dull ache in the right upper quadrant.
The differential diagnosis of biliary strictures may be difficult to prove the wide spectrum of alternative diagnoses, including PSC, gallbladder carcinoma, pancreatic carcinoma, intraductal papillary mucinous tumor, or benign biliary strictures from causes such as pancreatitis.
Preoperative evaluation
Imaging techniques including ultrasound, CT, and MRI are of limited sensitivity for the detection of CCA. However, technological breakthroughs have made multiple endoscopic modalities available for the evaluation of patients with masses of indeterminate origin and diagnosis of CCA. Endoscopic retrograde cholangiopancreatography (ERCP) is a powerful tool in the diagnosis of CCAs. It has the ability to define the anatomy of the biliary system and to determine the extent of bile duct involvement. Moreover, tissue specimens may be obtained for cytological confirmation. While cytology provides an almost 100% specificity, it carries the disadvantage of low sensitivity. Newer approaches, such as digital image analysis (DIA) and fluorescence in situ hybridization (FISH) promise better results by overcoming the restrictions of specimens with limited cellularity and offering increased sensitivity without compromising its high specificity.[29,30]In addition, ERCP may be used for stent placement in order to provide palliation and relieve jaundice.[31]
Magnetic resonance cholangiopancreatography (MRCP) is a noninvasive technique with the ability to evaluate intrahepatic lesions with a sensitivity of 86% and a specificity of 98%.[32]Unfortunately, this advantage is also its greatest disadvantage, as tissue sampling is not possible. Another available option is CT or percutaneous ultrasound-guided fine needle aspiration. This is a more difficult technique with a long learning curve; tumors are often small and isoechoic to the liver, making them difficult to access.[33,34]Consequently, despite its good results compared with ERCP, it is less frequently used.
Surgery
Surgery is the treatment of choice as it is the only potentially curative therapy for patients suffering from CCA. Tumors arising from cholangiocytes grow slowly and metastasize late during disease progression.[35]Given that in most cases CCAs are well advanced at the time of diagnosis, however, treatment options become limited and surgery ceases to be a feasible proposition.
The resectability of CCA depends on the exclusion of peritoneal and distant lymph node metastases and the absence of major vascular invasion.[36]Exclusion criteria for resection include encasement of the contralateral portal vein or hepatic artery, contralateral involvement of secondary biliary radicles and lymph node metastases beyond the hepatoduodenal ligament. Peritoneal metastases that are overlooked on abdominal CT should be excluded laparoscopically.[37]
Segmentectomy or lobectomy is the preferred operation for solitary intrahepatic CCAs.[38]Removal of the caudate lobe during hepatic resection for CCA has been proposed and is widely accepted as offering improved tumor cell-free margins at minimal morbidity cost. Moreover, this procedure eliminates the most frequent site of hepatic recurrence, which is the caudate lobe.[39]Less extensive procedures have proved beneficial for less advanced disease if the resection margins are free of tumor and are the operations of choice in such instances.
Major hepatectomy with systematic nodal dissection is associated with prolonged survival in patients with carcinoma involving the hepatic hilus, including those with advanced disease. Extended hemihepatectomy, with or without pancreatoduodenectomy, plus extrahepatic bile duct resection and regional lymphadenectomy, has recently been recognized as the standard curative treatment for hilar bile duct cancer. During left hepatectomy, Spiegel's lobe removal is necessary for Bismuth-Corlette type IIIb tumors, while its efficiency in type I-IIIa hilar CCA remains to be evaluated.[40]Pancreatoduodenectomy is the treatment of choice for middle and distal bile duct cancer. Major hepatectomy with pancreatoduodenectomy has been performed in selected patients with widespread disease with controversial results. In addition, en bloc resection has been linked with a better outcome but may not be technically feasible in the majority of cases, especially when there is involvement of the left hepatic duct.[41]However, in spite of optimum surgery establishing tumor cell-free margins, the absence of lymph node dissemination and despite the improvement achieved over the last decade, the 5-year survival rates still range from 13% to 44%.[5,42-44]
On the other hand, tumors associated with a bilateral lobal extension involving the secondary biliary radicles should be classified as unresectable. Unfortunately, the percentage of patients referred with advanced disease is very high, partly because of the latency and low sensitivity of the symptoms. Other contraindications for curative surgical management include unilobar disease with encasement of the contralateral portal vein or hepatic artery branch, bilateral portal vein or hepatic artery branch encasement, the presence of distant metastases, and significant comorbidities.[3,45]
Perioperative morbidity following resection of CCA has been high, ranging from 31% to 85%. Most of the reported complications are related to the biliary tree, including abscesses, bile and pancreatic leak and cholangitis, whereas others include hemorrhage and miscellaneous infections.[46]The short-term surgicalprocedure outcome has improved over the last decade and postoperative mortality ranges from 5% to 10%.[44-49]
In order to increase resectability, portal vein embolization (PVE) has been proposed as adding multiple potential benefits. PVE before hepatectomy is designed to induce atrophy of the embolized lobe scheduled to be resected, while inducing compensatory hypertrophy of the preserved lobe. PVE enables safe and potentially curative extended hepatectomy in a subset of patients who would otherwise be marginal candidates for resection based on a small liver remnant size.[50-52]
Aggressive management
Aggressive surgery is indicated in patients with locally advanced CCA, because they are associated with considerable postoperative morbidity and mortality. Recent advances in microvascular techniques in digestive organ surgery are responsible for placing new options on the table. Combined liver and portal vein resection and concomitant reconstruction has been applied, with significantly increased survival rates compared to nonresected patients.[53,54]Despite the overall improvement, there is a 2-year postoperative survival after portal vein resection of 17% compared with 5% in patients without resection.[55]Several techniques can be used for portal vein reconstruction. End-to-end anastomosis, graft interposition using the iliac vein, hepatic venous segment, saphenous vein or a left renal venous patch are some of the techniques described for portal vein reconstruction without any one of them having been demonstrated as being significantly beneficial over the rest.[56-58]Combined liver and retrohepatic inferior vena cava resection and reconstruction using an artificial graft (ePTFE) has also been used for advanced CCAs. However, the benefits emerging from this technically difficult process are far from proven.[59,60]In addition, hepatopancreatoduodenectomy has been proposed as a possible alternative technique.[61,62]
An aggressive approach, including portal vein resection combined with major liver resection, should be limited to young patients with locally advanced CCAs that are considered unresectable by standard liver resection. As this surgery has been carried out at experienced centers, the reported postoperative morbidity and mortality rates are within an acceptable range. Moreover, negative margins may be achieved in 80% of cases and this is directly associated with improved survival.[53]Fiveyear actuarial survival with the aggressive approach has been described as high as 32%.[63]
Local resection
Local resection is widely considered to be safer than liver resection and can be considered in patients with Bismuth typeihilar CCA.[64]Its mortality is significantly lower; in some studies no mortality has been described after local excision compared with extended procedures. Moreover, the morbidity rates are reduced about 50% after local resection, compared with rates in patients who undergo extended procedures.[5,65]One of the greatest disadvantages of this procedure lies in the fact that radicality may significantly drop as low as 28%, while the absence of negative margins increases the incidence of recurrence.[66]
In earlier reports, the 5-year survival rates were significantly lower after local resection than after extended surgery (7% vs. 17%). In these studies, it is likely that patients undergoing local resection had tumors with or without minimal involvement of the bile duct confluence, which could explain the unsatisfactory results.[5,45]On the other hand, numerous large studies have shown no evidence of any statistical difference in survival between local resection and extended surgery.[67-69]Furthermore, it has been proposed that local surgery may be beneficial compared to radical resection in strictly selected cases of patients with small, early stage tumors. One such study demonstrated a 5-year survival rate after local resection of up to 27%, a marked improvement on the 5-year survival rate after associated liver resection of just 6%.[70]
However, local resection is an inadequate treatment for hilar CCA involving the bile duct confluence; in this instance, liver resection should be recommended. Notwithstanding, it represents an attractive option for selected patients with early stage CCA, who could be benefitted by a notably better short-term outcome and without cost in long-term survival.
Is there a role for liver transplantation?
Liver transplantation for CCA remains a controversial subject. However, the prospect of achieving negative margins within the liver and accomplishing a radical resection has rendered transplantation an attractive option. In fact, this technique may only be used for hilar CCAs, as transplantation for intrahepatic or extrahepatic tumors is fraught with high recurrence rates and rapid metastases of the tumor (peritoneal spread, or distant metastases). For this reason, it has been abandoned.[71]Extrahepatic nodal disease or metastases are also contraindications to liver transplantation. In addition, recent multicenter series have reported unsatisfactory results with 3-year survival rates of less than 30% and a 26-month median time to recurrence.[72-74]However, selected patients with early stage CCA canbe treated with liver transplantation within a research protocol. Preliminary results have shown that liver transplantation combined with external-beam radiation, systemic 5-FU and brachytherapy can be a treatment of choice for highly selected early stage patients. Another therapeutic approach, which combines liver transplantation and preoperative aggressive neoadjuvant therapy, has produced more promising results with 5-year survival rates reaching 71%. This remarkable improvement in survival could possibly be accredited to a better control of locoregional cancer by neoadjuvant therapy, as CCA resection failures are usually thought to be the result of locoregional recurrence rather than distant metastases.[42,75,76]As prioritization for deceased donor liver allocation is a highly controversial matter and the prolonged waiting time has been recognized as an adverse prognostic factor, this protocol may only be applied to highly selected patients (younger than 45 years, who develop CCA as a result of PSC with early stage hilar CCA.[76,77]
In summary, the aim to expand the indications for liver transplantation for CCA reflects the efforts of transplant surgeons to provide an effective form of therapy for a previously untreatable disease. In this regard, liver transplantation for CCA should continue in the context of an allocation system that includes the severe organ availability, patient disease factors, and waiting times.
Palliative treatment
Palliative surgery in patients with CCA offers an alternative to an aggressive surgical approach, with significantly better short-term outcomes. Patients with intrahepatic CCA have shown no survival benefits from palliative resection over curative resection. Consequently, with the exception of highly selected patients, those with such a malignancy should be excluded from palliative management.[78,79]Palliative resections have a relevant beneficial impact on the outcome of patients with distal and hilar CCA. Long-term survival has been reported as relatively high and efficiency is noteworthy.[80,81]
Surgical drainage procedures have not been demonstrated to be superior to non-operative palliation with respect to procedure-related mortality and survival. Non-surgical stenting should be regarded as the first choice of palliative biliary drainage for patients with hilar CCA and for those with distal CCA and short life expectancy. For patients with distal CCA and longer projected survival, a surgical bypass should be considered.[82-84]
Photodynamic therapy (PDT) has been used in palliative management with encouraging results. It is a minimally invasive procedure and is based on photosensitizers that are chemical compounds stimulated by light of a specific wavelength. A photosensitizer is administered to the patient and the tissue to be treated is exposed to light suitable for stimulating the photosensitizer. The close proximity of the photosensitizer and an oxygen molecule creates a stimulated singlet state oxygen molecule, which induces tumor cell death through apoptosis or necrosis, occlusion and thrombosis of small vessels supporting the malignant tumor.[85-87]PDT may be used for cholestasis treatment and is reported to improve quality of life with longer survival.[88-93]Side-effects are rare and may include phototoxicity.
Despite the use of PDT providing such promising data, its evaluation as an adjuvant treatment remains uncontrolled and therefore should only be regarded as palliative management.[88]
Neo-adjuvant therapy
Currently, there are no adjuvant and neoadjuvant treatments available as curative treatment for patients suffering from CCA. In addition, although we know that many neo-adjuvant therapies are effective in eradicating tumors, the frequent lack of residual disease diminishes our capacity to measure the tumor response. The only objective endpoints that can be validated are diseasefree and overall survival.
Neo-adjuvant chemoradiotherapy can be an option for selected patients. McMaster et al[94]reported 9 patients with extrahepatic bile duct cancer who underwent preoperative chemoradiation. A pathological complete response was obtained in 3 patients, and negative margins were obtained in all patients (100%). In patients with stageior II cholangiocarcinoma, Rea et al[95]reported the 1-, 3-, and 5-year survival rates were 82%, 48%, and 21% after neoadjuvant radiotherapy, chemosensitization and resection respectively and the recurrence rate was 25%. This treatment requires further confirmation. As a consequence, the role of neo-adjuvant therapy remains investigational.
The role of adjuvant chemotherapy in CCA is yet to be determined, with conflicting data regarding its effect on survival. Some studies[93-96]have proposed that chemotherapy prolongs survival in CCA, especially in patients with unresectable tumors. However, the result has been questioned as in many cases they were statistically underpowered and restricted to short-term follow-up. Most of the studies[96,97]failed to show any survival benefit gained by chemotherapy.
Radiation therapy has also been proposed as an alternative procedure, but the effectiveness of thismodality remains very low. The CCA cell response to radiation is so poor that radiation therapy has been abandoned in most centers. Moreover, this procedure has been associated with a marked deterioration in patients' quality of life and significant morbidity, including gastrointestinal bleeding, biliary strictures, intestinal obstruction, and hepatic decompensation.[98-100]The combination of chemotherapy and radiation has been demonstrated to provide better results than the individual procedures, however further studies are required to support these findings.[101]
In summary, chemotherapy, radiation and PDT cannot be unconditionally recommended for adjuvant therapy of CCA.
Prognostic factors
Because of the increasing incidence of CCA worldwide, it is vital to identify the factors associated with a better outcome. Among numerous prognostic factors that have been described, the most important for long-term survival are negative surgical margins, lymph node status, and differentiation grade of the tumor. The most consistent independent determinant for long-term survival after potentially curative resection of a biliary tumor is the surgical margin status of the resected bile duct. Non-free margins are associated with a major decrease in survival rates and an increase in recurrence rates.[102-107]
Lymphatic dissemination is also an important prognostic factor. Lymphatic node (LN) involvement is present in up to 55% of patients undergoing operation for CCA. An increased number of infiltrated LNs as well as the presence of para-aortic LNs is associated with a worse outcome. A 5-year survival rate of 14% for patients with regional LN metastases and of 12% for those with positive para-aortic nodes has been reported. LN micrometastasis has no impact on survival in patients with otherwise negative LNs.[107-110]
Poorly differentiated adenocarcinomas are linked with lower 5-year survival rates and are commonly associated with LN dissemination. Moreover, microinvasion of small blood vessels is related to high recurrence rates.[45,111]Portal vein invasion is a strong prognostic factor of CCA and the actual number of 5-year survivors is limited, reaching only 9.9% compared with patients without portal vein resection (36.8%).[54]
Furthermore, perineural invasion of malignant cells along the nerve branches present within the biliary tract tissue has been shown to reduce survival rates.[112]Whether the TNM-based staging system is an important predictor remains controversial. Astonishingly, only a few studies confirm higher classification according to the TNM system with lower survival rates. Controversially, several studies have failed to demonstrate any predictive value for the staging system in use.[105,113]Low preoperative bilirubin levels are associated with better short-term as well as long-term outcome.[84,114]
Furthermore, patients who undergo combined portal vein resection have been associated with a significantly shorter time of survival compared with those who did not need portal vein resection.[107]
To stent or not to stent?
Resectability rates of 20%-55% have been reported when all cases referred to a specialist surgical unit are considered,[115,116]and for those pending surgery the respectability rates range from 30% to over 90%.[117]For those patients requiring surgery, the practice of placing a stent prior to surgery to achieve biliary decompression remains controversial. It is believed that routine preliminary decompression of the biliary tree is unnecessary. Indeed, controlled trials using preoperative percutaneous transhepatic biliary drainage have shown that as a routine procedure it provides no benefit. Stent associated biliary sepsis poses a considerable problem. In addition, a marked pericholangitic phenomenon has been observed in patients with biliary stents, in the form of surrounding edema and possible periductal fibrosis. It is postulated that this reaction is related to local sepsis and/or the presence of a foreign body. This phenomenon coupled with the presence of the biliary stent that may make it more difficult to assess the proximal extent of the tumor intraoperatively and may increase the risk of infections postoperatively. However, biliary drainage can prove extremely useful in certain circumstances, such as in cases of cholangitis. It certainly reduces liver size and turgidity and renders liver mobilization and subsequent resection technically easier. Incomplete biliary drainage accounts for the high incidence of early cholangitis ranging from 20% to 40% after placement of stents.[118]Moreover, elevated bilirubin levels and liver dysfunction are factors that adversely affect postoperative morbidity, thus advocating stent placement. Unilateral stents are typically adequate and associated with a higher success rate for stent insertion, drainage and lower early complication rate compared to bilateral stenting of both hepatic lobes.[31]
Moreover, the introduction of expandable metal stents has resulted in both an improvement of successful palliation rates and a decrease in the frequency of complications. If drainage is indicated, it is important to operate within two weeks, especially if a bypassprocedure is contemplated, to ensure an adequate duct diameter for anastomotic reconstruction.[119-123]
Conclusion
In conclusion, CCA is a rare malignancy associated with poor prognosis. The only curative treatment available is surgical management. Unfortunately, many patients present with unresectable tumors, and the majority of whom die within a year of diagnosis. Surgical treatment involves major resections of the liver, pancreas and bile duct, with considerable mortality and morbidity. However, in selected cases and where indicated, appropriate management with aggressive surgery may achieve a good outcome with a prolonged survival expectancy.
Funding:None.
Ethical approval:Not needed.
Contributors:ZF wrote the main body of the article under the supervision of ZGN. FA and CD provided advice on medical aspects. KK is the guarantor.
Competing interest:No bene fits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Blumgart LH, Benjamin IS. Liver resection for bile duct cancer. Surg Clin North Am 1989;69:323-337.
2 Landis SH, Murray T, Bolden S, Wingo PA. Cancer statistics, 1998. CA Cancer J Clin 1998;48:6-29.
3 Patel T. Worldwide trends in mortality from biliary tract malignancies. BMC Cancer 2002;2:10.
4 Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis 2004;24:115-125.
5 Boerma EJ. Research into the results of resection of hilar bile duct cancer. Surgery 1990;108:572-580.
6 Bengmark S, Ekberg H, Evander A, Klofver-Stahl B, Tranberg KG. Major liver resection for hilar cholangiocarcinoma. Ann Surg 1988;207:120-125.
7 Bosma A. Surgical pathology of cholangiocarcinoma of the liver hilus (Klatskin tumor). Semin Liver Dis 1990;10:85-90.
8 Burak K, Angulo P, Pasha TM, Egan K, Petz J, Lindor KD. Incidence and risk factors for cholangiocarcinoma in primary sclerosing cholangitis. Am J Gastroenterol 2004;99:523-526.
9 Chen MF, Jan YY, Jeng LB, Hwang TL, Wang CS, Chen SC, et al. Intrahepatic cholangiocarcinoma in Taiwan. J Hepatobiliary Pancreat Surg 1999;6:136-141.
10 Kubo S, Kinoshita H, Hirohashi K, Hamba H. Hepatolithiasis associated with cholangiocarcinoma. World J Surg 1995;19: 637-641.
11 Okuda K, Nakanuma Y, Miyazaki M. Cholangiocarcinoma: recent progress. Part 1: epidemiology and etiology. J Gastroenterol Hepatol 2002;17:1049-1055.
12 Lesurtel M, Regimbeau JM, Farges O, Colombat M, Sauvanet A, Belghiti J. Intrahepatic cholangiocarcinoma and hepatolithiasis: an unusual association in Western countries. Eur J Gastroenterol Hepatol 2002;14:1025-1027.
13 Chapman RW. Risk factors for biliary tract carcinogenesis. Ann Oncol 1999;10:308-311.
14 Kurathong S, Lerdverasirikul P, Wongpaitoon V, Pramoolsinsap C, Kanjanapitak A, Varavithya W, et al. Opisthorchis viverrini infection and cholangiocarcinoma. A prospective, case-controlled study. Gastroenterology 1985;89:151-156.
15 Watanapa P, Watanapa WB. Liver fluke-associated cholangiocarcinoma. Br J Surg 2002;89:962-970.
16 Hardell L, Bengtsson NO, Jonsson U, Eriksson S, Larsson LG. Aetiological aspects on primary liver cancer with special regard to alcohol, organic solvents and acute intermittent porphyria--an epidemiological investigation. Br J Cancer 1984;50:389-397.
17 Welzel TM, Graubard BI, El-Serag HB, Shaib YH, Hsing AW, Davila JA, et al. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma in the United States: a population-based case-control study. Clin Gastroenterol Hepatol 2007;5:1221-1228.
18 Marzioni M, Fava G, Benedetti A. Nervous and Neuroendocrine regulation of the pathophysiology of cholestasis and of biliary carcinogenesis. World J Gastroenterol 2006;12:3471-3480.
19 Kobayashi M, Ikeda K, Saitoh S, Suzuki F, Tsubota A, Suzuki Y, et al. Incidence of primary cholangiocellular carcinoma of the liver in japanese patients with hepatitis C virus-related cirrhosis. Cancer 2000;88:2471-2477.
20 Shaib YH, El-Serag HB, Davila JA, Morgan R, McGlynn KA. Risk factors of intrahepatic cholangiocarcinoma in the United States: a case-control study. Gastroenterology 2005;128:620-626.
21 Esteller M. Cancer epigenomics: DNA methylomes and histone-modification maps. Nat Rev Genet 2007;8:286-298.
22 Kim BH, Cho NY, Choi M, Lee S, Jang JJ, Kang GH. Methylation profiles of multiple CpG island loci in extrahepatic cholangiocarcinoma versus those of intrahepatic cholangiocarcinomas. Arch Pathol Lab Med 2007;131:923-930.
23 Yang B, House MG, Guo M, Herman JG, Clark DP. Promoter methylation profiles of tumor suppressor genes in intrahepatic and extrahepatic cholangiocarcinoma. Mod Pathol 2005;18: 412-420.
24 Tischoff I, Markwarth A, Witzigmann H, Uhlmann D, Hauss J, Mirmohammadsadegh A, et al. Allele loss and epigenetic inactivation of 3p21.3 in malignant liver tumors. Int J Cancer 2005;115:684-689.
25 Brennecke J, Hipfner DR, Stark A, Russell RB, Cohen SM. bantam encodes a developmentally regulated microRNA that controls cell proliferation and regulates the proapoptotic gene hid in Drosophila. Cell 2003;113:25-36.
26 Calin GA, Sevignani C, Dumitru CD, Hyslop T, Noch E, Yendamuri S, et al. Human microRNA genes are frequently located at fragile sites and genomic regions involved in cancers. Proc Natl Acad Sci U S A 2004;101:2999-3004.
27 Meng F, Henson R, Lang M, Wehbe H, Maheshwari S, Mendell JT, et al. Involvement of human micro-RNA in growth and response to chemotherapy in human cholangiocarcinoma cell lines. Gastroenterology 2006;130:2113-2129.
28 Mott JL, Kobayashi S, Bronk SF, Gores GJ. mir-29 regulates Mcl-1 protein expression and apoptosis. Oncogene 2007;26: 6133-6140.
29 Baron TH, Harewood GC, Rumalla A, Pochron NL, Stadheim LM, Gores GJ, et al. A prospective comparison of digital image analysis and routine cytology for the identification of malignancy in biliary tract strictures. Clin GastroenterolHepatol 2004;2:214-219.
30 Fogel EL, deBellis M, McHenry L, Watkins JL, Chappo J, Cramer H, et al. Effectiveness of a new long cytology brush in the evaluation of malignant biliary obstruction: a prospective study. Gastrointest Endosc 2006;63:71-77.
31 De Palma GD, Galloro G, Siciliano S, Iovino P, Catanzano C. Unilateral versus bilateral endoscopic hepatic duct drainage in patients with malignant hilar biliary obstruction: results of a prospective, randomized, and controlled study. Gastrointest Endosc 2001;53:547-553.
32 Guibaud L, Bret PM, Reinhold C, Atri M, Barkun AN. Bile duct obstruction and choledocholithiasis: diagnosis with MR cholangiography. Radiology 1995;197:109-115.
33 Fritscher-Ravens A, Broering DC, Knoefel WT, Rogiers X, Swain P, Thonke F, et al. EUS-guided fine-needle aspiration of suspected hilar cholangiocarcinoma in potentially operable patients with negative brush cytology. Am J Gastroenterol 2004;99:45-51.
34 Eloubeidi MA, Chen VK, Jhala NC, Eltoum IE, Jhala D, Chhieng DC, et al. Endoscopic ultrasound-guided fine needle aspiration biopsy of suspected cholangiocarcinoma. Clin Gastroenterol Hepatol 2004;2:209-213.
35 Malhi H, Gores GJ. Cholangiocarcinoma: modern advances in understanding a deadly old disease. J Hepatol 2006;45:856-867. 36 Nagorney DM, Kendrick ML. Hepatic resection in the treatment of hilar cholangiocarcinoma. Adv Surg 2006;40:159-171.
37 Weber SM, DeMatteo RP, Fong Y, Blumgart LH, Jarnagin WR. Staging laparoscopy in patients with extrahepatic biliary carcinoma. Analysis of 100 patients. Ann Surg 2002;235:392-399.
38 Targarona EM, Zografos G, Habib NA. Liver resection for recurrent hilar cholangiocarcinoma. Br J Surg 1993;80:1433.
39 Nimura Y, Hayakawa N, Kamiya J, Kondo S, Shionoya S. Hepatic segmentectomy with caudate lobe resection for bile duct carcinoma of the hepatic hilus. World J Surg 1990;14:535-544.
40 Parikh AA, Abdalla EK, Vauthey JN. Operative considerations in resection of hilar cholangiocarcinoma. HPB (Oxford) 2005; 7:254-258.
41 Van der Heyde MN, Verbeek PC, Lygidakis NJ. Decisionmaking in the treatment of patients with malignant proximal bile duct obstruction. Semin Liver Dis 1990;10:145-148.
42 Madariaga JR, Iwatsuki S, Todo S, Lee RG, Irish W, Starzl TE. Liver resection for hilar and peripheral cholangiocarcinomas: a study of 62 cases. Ann Surg 1998;227:70-79.
43 Ohtsuka M, Ito H, Kimura F, Shimizu H, Togawa A, Yoshidome H, et al. Results of surgical treatment for intrahepatic cholangiocarcinoma and clinicopathological factors influencing survival. Br J Surg 2002;89:1525-1531.
44 Valverde A, Bonhomme N, Farges O, Sauvanet A, Flejou JF, Belghiti J. Resection of intrahepatic cholangiocarcinoma: a Western experience. J Hepatobiliary Pancreat Surg 1999;6:122-127.
45 Jarnagin WR, Ruo L, Little SA, Klimstra D, D'Angelica M, DeMatteo RP, et al. Patterns of initial disease recurrence after resection of gallbladder carcinoma and hilar cholangiocarcinoma: implications for adjuvant therapeutic strategies. Cancer 2003;98: 1689-1700.
46 Forsmo HM, Horn A, Viste A, Hoem D, Ovrebo K. Survival and an overview of decision-making in patients with cholangiocarcinoma. Hepatobiliary Pancreat Dis Int 2008;7:412-417.
47 Gazzaniga GM, Filauro M, Bagarolo C, Mori L. Surgery for hilar cholangiocarcinoma: an Italian experience. J Hepatobiliary Pancreat Surg 2000;7:122-127.
48 Jarnagin WR, Fong Y, DeMatteo RP, Gonen M, Burke EC, Bodniewicz BS J, et al. Staging, resectability, and outcome in 225 patients with hilar cholangiocarcinoma. Ann Surg 2001; 234:507-519.
49 Kawarada Y, Das BC, Naganuma T, Tabata M, Taoka H. Surgical treatment of hilar bile duct carcinoma: experience with 25 consecutive hepatectomies. J Gastrointest Surg 2002; 6:617-624.
50 Abdalla EK, Barnett CC, Doherty D, Curley SA, Vauthey JN. Extended hepatectomy in patients with hepatobiliary malignancies with and without preoperative portal vein embolization. Arch Surg 2002;137:675-681.
51 Makuuchi M, Thai BL, Takayasu K, Takayama T, Kosuge T, Gunvén P, et al. Preoperative portal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: a preliminary report. Surgery 1990;107:521-527.
52 Nagino M, Kamiya J, Nishio H, Ebata T, Arai T, Nimura Y. Two hundred forty consecutive portal vein embolizations before extended hepatectomy for biliary cancer: surgical outcome and long-term follow-up. Ann Surg 2006;243:364-372.
53 Hemming AW, Kim RD, Mekeel KL, Fujita S, Reed AI, Foley DP, et al. Portal vein resection for hilar cholangiocarcinoma. Am Surg 2006;72:599-605.
54 Ebata T, Nagino M, Kamiya J, Uesaka K, Nagasaka T, Nimura Y. Hepatectomy with portal vein resection for hilar cholangiocarcinoma: audit of 52 consecutive cases. Ann Surg 2003;238:720-727.
55 Neuhaus P, Jonas S, Bechstein WO, Lohmann R, Radke C, Kling N, et al. Extended resections for hilar cholangiocarcinoma. Ann Surg 1999;230:808-819.
56 Lorf T, Hanack U, Ringe B. Portal vein replacement by hepatic vein transposition. Am J Surg 1997;174:353-354.
57 Miyazaki M, Kato A, Ito H, Kimura F, Shimizu H, Ohtsuka M, et al. Combined vascular resection in operative resection for hilar cholangiocarcinoma: does it work or not? Surgery 2007; 141:581-588.
58 Sakaguchi S, Nakamura S. Surgery of the portal vein in resection of cancer of the hepatic hilus. Surgery of the portal vein in resection of cancer of the hepatic hilus. Surgery 1986; 99:344-349
59 Arii S, Teramoto K, Kawamura T, Takamatsu S, Sato E, Nakamura N, et al. Significance of hepatic resection combined with inferior vena cava resection and its reconstruction with expanded polytetrafluoroethylene for treatment of liver tumors. J Am Coll Surg 2003;196:243-249.
60 Azoulay D, Andreani P, Maggi U, Salloum C, Perdigao F, Sebagh M, et al. Combined liver resection and reconstruction of the supra-renal vena cava: the Paul Brousse experience. Ann Surg 2006;244:80-88.
61 Kaneoka Y, Yamaguchi A, Isogai M. Hepatopancreatoduode nectomy: its suitability for bile duct cancer versus gallbladder cancer. J Hepatobiliary Pancreat Surg 2007;14:142-148.
62 Urahashi T, Yamamoto M, Ohtsubo T, Katsuragawa H, Katagiri S, Takasaki K. Hepatopancreatoduodenectomy could be allowed for patients with advanced intrahepatic cholangiocarcinoma. Hepatogastroenterology 2007;54:346-349.
63 Hemming AW, Reed AI, Fujita S, Zendejas I, Howard RJ, Kim RD. Role for extending hepatic resection using an aggressiveapproach to liver surgery. J Am Coll Surg 2008;206:870-878.
64 Bismuth H, Castaing D, Traynor O. Resection or palliation: priority of surgery in the treatment of hilar cancer. World J Surg 1988;12:39-47.
65 Sano T, Shimada K, Sakamoto Y, Yamamoto J, Yamasaki S, Kosuge T. One hundred two consecutive hepatobiliary resections for perihilar cholangiocarcinoma with zero mortality. Ann Surg 2006;244:240-247.
66 Tsao JI, Nimura Y, Kamiya J, Hayakawa N, Kondo S, Nagino M, et al. Management of hilar cholangiocarcinoma: comparison of an American and a Japanese experience. Ann Surg 2000; 232:166-174.
67 Jang JY, Kim SW, Park DJ, Ahn YJ, Yoon YS, Choi MG, et al. Actual long-term outcome of extrahepatic bile duct cancer after surgical resection. Ann Surg 2005;241:77-84.
68 Launois B, Reding R, Lebeau G, Buard JL. Surgery for hilar cholangiocarcinoma: French experience in a collective survey of 552 extrahepatic bile duct cancers. J Hepatobiliary Pancreat Surg 2000;7:128-134.
69 Tabata M, Kawarada Y, Yokoi H, Higashiguchi T, Isaji S. Surgical treatment for hilar cholangiocarcinoma. J Hepatobiliary Pancreat Surg 2000;7:148-154.
70 Launois B, Terblanche J, Lakehal M, Catheline JM, Bardaxoglou E, Landen S, et al. Proximal bile duct cancer: high resectability rate and 5-year survival. Ann Surg 1999;230: 266-275.
71 Meyer CG, Penn I, James L. Liver transplantation for cholangiocarcinoma: results in 207 patients. Transplantation 2000;69:1633-1637.
72 Brandsaeter B, Isoniemi H, Broomé U, Olausson M, Backman L, Hansen B, et al. Liver transplantation for primary sclerosing cholangitis; predictors and consequences of hepatobiliary malignancy. J Hepatol 2004;40:815-822.
73 Ghali P, Marotta PJ, Yoshida EM, Bain VG, Marleau D, Peltekian K, et al. Liver transplantation for incidental cholangiocarcinoma: analysis of the Canadian experience. Liver Transpl 2005;11:1412-1416.
74 Robles R, Figueras J, Turrión VS, Margarit C, Moya A, Varo E, et al. Spanish experience in liver transplantation for hilar and peripheral cholangiocarcinoma. Ann Surg 2004;239:265-271.
75 Sudan D, DeRoover A, Chinnakotla S, Fox I, Shaw B Jr, McCashland T, et al. Radiochemotherapy and transplantation allow long-term survival for nonresectable hilar cholangiocarcinoma. Am J Transplant 2002;2:774-779.
76 Rosen CB, Heimbach JK, Gores GJ. Surgery for cholangiocarcinoma: the role of liver transplantation. HPB (Oxford) 2008;10:186-189.
77 Heimbach JK, Gores GJ, Haddock MG, Alberts SR, Pedersen R, Kremers W, et al. Predictors of disease recurrence following neoadjuvant chemoradiotherapy and liver transplantation for unresectable perihilar cholangiocarcinoma. Transplantation 2006;82:1703-1707.
78 Kawarada Y, Yamagiwa K, Das BC. Analysis of the relationships between clinicopathologic factors and survival time in intrahepatic cholangiocarcinoma. Am J Surg 2002;183: 679-685.
79 Lang H, Sotiropoulos GC, Frühauf NR, Domland M, Paul A, Kind EM, et al. Extended hepatectomy for intrahepatic cholangiocellular carcinoma (ICC): when is it worthwhile? Single center experience with 27 resections in 50 patients over a 5-year period. Ann Surg 2005;241:134-143.
80 Kosuge T, Yamamoto J, Shimada K, Yamasaki S, Makuuchi M. Improved surgical results for hilar cholangiocarcinoma with procedures including major hepatic resection. Ann Surg 1999;230:663-671.
81 Witzigmann H, Berr F, Ringel U, Caca K, Uhlmann D, Schoppmeyer K, et al. Surgical and palliative management and outcome in 184 patients with hilar cholangiocarcinoma: palliative photodynamic therapy plus stenting is comparable to r1/r2 resection. Ann Surg 2006;244:230-239.
82 Lai EC, Chu KM, Lo CY, Fan ST, Lo CM, Wong J. Choice of palliation for malignant hilar biliary obstruction. Am J Surg 1992;163:208-212.
83 Moss AC, Morris E, Leyden J, MacMathuna P. Malignant distal biliary obstruction: a systematic review and metaanalysis of endoscopic and surgical bypass results. Cancer Treat Rev 2007;33:213-221.
84 Zhang BH, Cheng QB, Luo XJ, Zhang YJ, Jiang XQ, Zhang BH, et al. Surgical therapy for hiliar cholangiocarcinoma: analysis of 198 cases. Hepatobiliary Pancreat Dis Int 2006;5:278-282.
85 Abels C. Targeting of the vascular system of solid tumours by photodynamic therapy (PDT). Photochem Photobiol Sci 2004;3:765-771.
86 Krammer B. Vascular effects of photodynamic therapy. Anticancer Res 2001;21:4271-4277.
87 Ortner MA, Dorta G. Technology insight: Photodynamic therapy for cholangiocarcinoma. Nat Clin Pract Gastroenterol Hepatol 2006;3:459-467.
88 Nanashima A, Yamaguchi H, Shibasaki S, Ide N, Sawai T, Tsuji T, et al. Adjuvant photodynamic therapy for bile duct carcinoma after surgery: a preliminary study. J Gastroenterol 2004;39:1095-1101.
89 Berr F, Wiedmann M, Tannapfel A, Halm U, Kohlhaw KR, Schmidt F, et al. Photodynamic therapy for advanced bile duct cancer: evidence for improved palliation and extended survival. Hepatology 2000;31:291-298.
90 Ortner ME, Caca K, Berr F, Liebetruth J, Mansmann U, Huster D, et al. Successful photodynamic therapy for nonresectable cholangiocarcinoma: a randomized prospective study. Gastroenterology 2003;125:1355-1363.
91 Shim CS, Cheon YK, Cha SW, Bhandari S, Moon JH, Cho YD, et al. Prospective study of the effectiveness of percutaneous transhepatic photodynamic therapy for advanced bile duct cancer and the role of intraductal ultrasonography in response assessment. Endoscopy 2005;37:425-433.
92 Zoepf T, Jakobs R, Arnold JC, Apel D, Riemann JF. Palliation of nonresectable bile duct cancer: improved survival after photodynamic therapy. Am J Gastroenterol 2005;100:2426-2430.
93 Kelley ST, Bloomston M, Serafini F, Carey LC, Karl RC, Zervos E, et al. Cholangiocarcinoma: advocate an aggressive operative approach with adjuvant chemotherapy. Am Surg 2004;70:743-749.
94 McMaster KM, Tuttle TM, Leach SD, Rich T, Cleary KR, Evans DB, et al. Neoadjuvant chemoradiation for extrahepatic cholangiocarcinoma. Am J Surg 1997;174:605-609.
95 Rea DJ, Heimbach JK, Rosen CB, Haddock MG, Alberts SR, Kremers WK, et al. Liver transplantation with neoadjuvant chemoradiation is more effective than resection for hilar cholangiocarcinoma. Ann Surg 2005;242:451-461.
96 Farhat MH, Shamseddine AI, Tawil AN, Berjawi G, Sidani C, Shamseddeen W, et al. Prognostic factors in patients with advanced cholangiocarcinoma: role of surgery, chemotherapy and body mass index. World J Gastroenterol 2008;14:3224-3230.
97 Yi B, Zhang BH, Zhang YJ, Jiang XQ, Zhang BH, Yu WL, et al. Surgical procedure and prognosis of hilar cholangiocarcinoma. Hepatobiliary Pancreat Dis Int 2004;3: 453-457.
98 Czito BG, Anscher MS, Willett CG. Radiation therapy in the treatment of cholangiocarcinoma. Oncology (Williston Park) 2006;20:873-895.
99 Foo ML, Gunderson LL, Bender CE, Buskirk SJ. External radiation therapy and transcatheter iridium in the treatment of extrahepatic bile duct carcinoma. Int J Radiat Oncol Biol Phys 1997;39:929-935.
100 Grove MK, Hermann RE, Vogt DP, Broughan TA. Role of radiation after operative palliation in cancer of the proximal bile ducts. Am J Surg 1991;161:454-458.
101 Nakeeb A, Pitt HA. Radiation therapy, chemotherapy and chemoradiation in hilar cholangiocarcinoma. HPB (Oxford) 2005;7:278-282.
102 Hasegawa S, Ikai I, Fujii H, Hatano E, Shimahara Y. Surgical resection of hilar cholangiocarcinoma: analysis of survival and postoperative complications. World J Surg 2007;31:1256-1263.
103 Jan YY, Yeh CN, Yeh TS, Hwang TL, Chen MF. Clinicopathological factors predicting long-term overall survival after hepatectomy for peripheral cholangiocarcinoma. World J Surg 2005;29:894-898.
104 Liu CL, Fan ST, Lo CM, Tso WK, Lam CM, Wong J. Improved operative and survival outcomes of surgical treatment for hilar cholangiocarcinoma. Br J Surg 2006;93: 1488-1494.
105 Silva MA, Tekin K, Aytekin F, Bramhall SR, Buckels JA, Mirza DF. Surgery for hilar cholangiocarcinoma; a 10 year experience of a tertiary referral centre in the UK. Eur J Surg Oncol 2005;31:533-539.
106 Cheng Q, Luo X, Zhang B, Jiang X, Yi B, Wu M. Predictive factors for prognosis of hilar cholangiocarcinoma: postresection radiotherapy improves survival. Eur J Surg Oncol 2007;33:202-207.
107 Nishio H, Nagino M, Nimura Y. Surgical management of hilar cholangiocarcinoma: the Nagoya experience. HPB (Oxford) 2005;7:259-262.
108 Kitagawa Y, Nagino M, Kamiya J, Uesaka K, Sano T, Yamamoto H, et al. Lymph node metastasis from hilar cholangiocarcinoma: audit of 110 patients who underwent regional and paraaortic node dissection. Ann Surg 2001;233: 385-392.
109 Hong SM, Cho H, Lee OJ, Ro JY. The number of metastatic lymph nodes in extrahepatic bile duct carcinoma as a prognostic factor. Am J Surg Pathol 2005;29:1177-1183.
110 Yoshida T, Matsumoto T, Sasaki A, Morii Y, Aramaki M, Kitano S. Prognostic factors after pancreatoduodenectomy with extended lymphadenectomy for distal bile duct cancer. Arch Surg 2002;137:69-73.
111 Takao S, Shinchi H, Uchikura K, Kubo M, Aikou T. Liver metastases after curative resection in patients with distal bile duct cancer. Br J Surg 1999;86:327-331.
112 Tajima Y, Kuroki T, Fukuda K, Tsuneoka N, Furui J, Kanematsu T. An intraductal papillary component is associated with prolonged survival after hepatic resection for intrahepatic cholangiocarcinoma. Br J Surg 2004;91:99-104.
113 Pichlmayr R, Weimann A, Klempnauer J, Oldhafer KJ, Maschek H, Tusch G, et al. Surgical treatment in proximal bile duct cancer. A single-center experience. Ann Surg 1996; 224:628-638.
114 Su CH, Tsay SH, Wu CC, Shyr YM, King KL, Lee CH, et al. Factors influencing postoperative morbidity, mortality, and survival after resection for hilar cholangiocarcinoma. Ann Surg 1996;223:384-394.
115 Jackson JE, Roddie ME, Yeung EY, Benjamin IS, Adam A. Biliary endoprosthesis dysfunction in patients with malignant hilar tumors: successful treatment by percutaneous replacement of the stent. AJR Am J Roentgenol 1990;155:391-395.
116 LaBerge JM, Doherty M, Gordon RL, Ring EJ. Hilar malignancy: treatment with an expandable metallic transhepatic biliary stent. Radiology 1990;177:793-797.
117 Mizumoto R, Kawarada Y, Suzuki H. Surgical treatment of hilar carcinoma of the bile duct. Surg Gynecol Obstet 1986; 162:153-158.
118 Laméris JS, Hesselink EJ, Van Leeuwen PA, Nijs HG, Meerwaldt JH, Terpstra OT. Ultrasound-guided percutaneous transhepatic cholangiography and drainage in patients with hilar cholangiocarcinoma. Semin Liver Dis 1990;10:121-125.
119 Nguyen K, Sing JT Jr. Review of endoscopic techniques in the diagnosis and management of cholangiocarcinoma. World J Gastroenterol 2008;14:2995-2999.
120 Soderlund C, Linder S. Covered metal versus plastic stents for malignant common bile duct stenosis: a prospective, randomized, controlled trial. Gastrointest Endosc 2006;63: 986-995.
121 Stern N, Sturgess R. Endoscopic therapy in the management of malignant biliary obstruction. Eur J Surg Oncol 2008;34: 313-317.
122 Freeman ML, Sielaff TD. A modern approach to malignant hilar biliary obstruction. Rev Gastroenterol Disord 2003;3: 187-201.
123 Strasberg SM. ERCP and surgical intervention in pancreatic and biliary malignancies. Gastrointest Endosc 2002;56:S213-217.
June 18, 2010
Accepted after revision September 25, 2010
Author Affiliations: Third Department of Surgery, Athens General Hospital, Athens, Greece (Zografos GN, Farfaras A and Chrysikos D); Department of Clinical Therapeutics, Alexandra Hospital, Athens, Greece (Zagouri F); and Department of Surgery, Red Cross Hospital, Athens, Greece (Karaliotas K)
Flora Zagouri, MD, PhD, Vas. Sofias Ave and Lourou str, Ampelokipi, Athens 11528, Greece (Tel: +306946462998; Fax: +302103381511; Email: florazagouri@yahoo.co.uk)
© 2011, Hepatobiliary Pancreat Dis Int. All rights reserved.
杂志排行

Hepatobiliary & Pancreatic Diseases International的其它文章
- Laparoscopic liver resection for benign and malignant liver tumors
- Assessment of tumor vascularization with functional computed tomography perfusion imaging in patients with cirrhotic liver disease
- Expression oflamino acid transport system 1 and analysis of iodine-123-methyltyrosine tumor uptake in a pancreatic xenotransplantation model using fused high-resolution-micro-SPECT-MRI
- Hepatobiliary & Pancreatic Diseases International (HBPD INT)
- Roles of sulfonylurea receptor 1 and multidrug resistance protein 1 in modulating insulin secretion in human insulinoma
- Atypical focal nodular hyperplasia of the liver