Revascularization for Iliac-femoral Artery Pseudoaneurysm with Greater Saphenous Vein
2010-11-22JidongWuYuehongZhengNimChoiandFurtadoRui
Ji-dong Wu ,Yue-hong Zheng *,Nim Choi ,and Furtado Rui
1Department of Vascular Surgery,Peking Union Medical College Hospital,Chinese Academy of Medical Sciences &Peking Union Medical College,Beijing 100730,China
2Department of General Surgery,Cir Gen/Vas,Central Hospital Centre S.Januario,Macau,China
ILIAC-femoral artery pseudoaneurysm caused by syringe injection belongs to the category of infectious pseudoaneurysm.It is a severe complication in drug abusers,with difficult and controversial management.The high risk and mortality of pseudoaneurysm in drug addicts are widely attributed to vessel rupture,dislodge of the embolus,compression,and infection.The controversy between artery ligation and revascularization is still unsettled.From March 2004 to October 2007 in Central Hospital Centre S.Januario,Macao,we conducted arterial reconstruction for 21 cases of artery pseudoaneurysm with ipsilateral autologous greater saphenous venous grafts through designed single curved inguinal incision,and investigated the surgical revascularization procedures,complications,and follow-up,in order to get a solution for the parenteral drug abusers who suffered from artery pseudoaneurysm.
PATIENTS AND METHODS
General information
Twenty-one drug abusers with iliac-femoral artery pseudoaneurysm were enrolled from March 2004 to October 2007,among which 15 cases were male and 6 were female,with an average age of 31.3 (range,19-56) years.All patients had a drug abusing history of more than 3 years.The puncture sites of drug injection were all confirmed by ultrasonography,digital substraction angiography (DSA),or computed tomography angiography(CTA) to be at femoral artery in all patients (Fig.1).The maximum diameter of pseudoaneurysm was within the range of 3.0-7.5 cm.Common femoral artery and distal external iliac artery were often involved.Aneurysm rupture and repeated bleeding were noted in 14 patients,complicated with infections in groin,manifesting symptoms such as pain,redness,local tissue necrosis,and pyorrhea.Six cases presented intermittent claudication.Three cases complained about pulsatile mass in thigh.Two patients developed phlegmon in their lower extremities.One patient had lower limb swelling.Emergency operations were performed on 14 patients with ruptured aneurysm.
Surgical treatment

Figure 1.Computed tomography (CT) scan of drug abuser with iliac-femoral artery pseudoaneurysm.
Single curved incision we designed for such disease was applied in operations performed on all the 21 cases.Under general anesthesia,a pathway of 15 cm in length was incised 5 cm above the ipsilateral inguinal ligament,curving toward inner part of the thigh.The inguinal ligament was cut off partially at upper incision,and external iliac artery was occluded at first (Fig.2).Heparin 100 U/kg was injected intravenously.Meanwhile,the superficial femoral artery was mobilized in case of bleeding.In most cases,a large amount of clots could be observed.After removal of these clots,the profunda femoral artery and collateral arteries were sutured.Abscesses existed in some cases at the bottom of aneurysm cavity,even deep into the pelvis or the anterior surface of femur.Necrotic tissue,pus,and mural thrombus were debrided by repeated rinsing.
Emergency procedures were performed on 14 patients immediately after the diagnosis of pseudoaneurysm rupture was confirmed.Extensive,even projecting,bleeding could be observed at the ruptured field.
All revascularization of lower limbs were accomplished with saphenous venous grafts.Through a curved incision,a 15-cm-long section of the trunk of greater saphenous vein was harvested following mobilization and ligation of tributaries.After dilating the harvested trunk with heparin saline,we created a bypass connecting external iliac artery and superficial femoral artery with this autologous graft in the mode of end-to-side anastomosis(Fig.3).
RESULTS

Figure 2.A single curved incision designed for excision of iliac-femoral pseudoaneurysm.
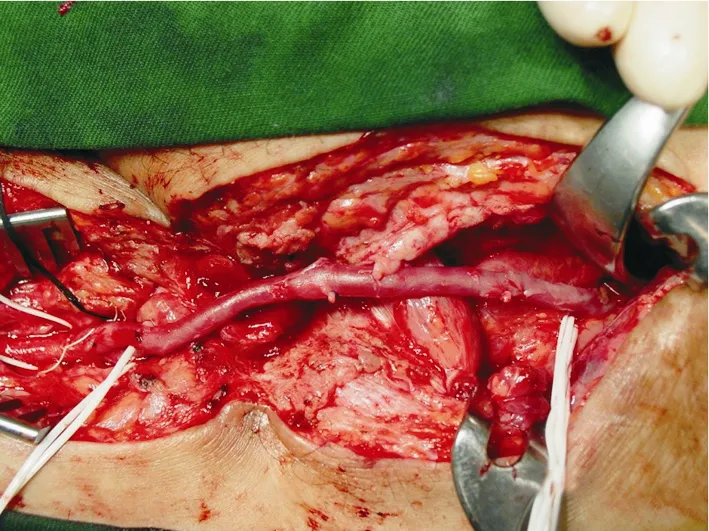
Figure 3.An iliac-femoral artery bypass with autologous greater saphenous venous graft.
Surgical procedures in all the 21 cases were finished without intraoperative mortality or perioperative complications.All the patients except one were free of claudication symptoms after revascularizations with autologous greater saphenous venous grafts.As for the case with preoperative popliteal artery stenosis,postoperative intermittent claudication was reported.One case later developed symptoms of infection and wound tissue fistula;one had inguinal incisional hematoma;and another complained about numbness or other abnormal feeling in thigh skin.The pulse of dorsal artery could be felt in 18 patients.
DISCUSSION
Pseudoaneurysm caused by syringe injection is a special type of infectious pseudoaneurysm.Drug abusers often use contaminated syringes,and lack techniques of injection.Pseudoaneurysm often leads to rupture and massive hemorrhage,and the patients accompanied with abscess manifest corresponding symptoms,which differ from iatrogenic pseudoaneurysm.For instance,the pseudoaneurysm developed in arteriovenous fistula for hemodialysis is rarely complicated by bacteremia or infection but mural thrombosis.1The main hazards of pseudoaneurysm caused by drug abuse are as follows:fatal hemorrhage as a result of rupture,thrombosis leading to distal embolization,as well as severe infection and organ dysfunction provoked by compression.These fatal complications are great challenges for vascular surgeons.2,3
Repeated drug injection may cause local infection and bleeding in patients with drug induced iliac-femoral artery pseudoaneurysm,thus the conventional artery repair method is infeasible.It is acknowledged that the optimal method is to reestablish blood circulation after excision of the pseudoaneurysm.Although end-to-end anastomosis of the femoral artery seems to be convenient in reconstruction,it is hard to apply to the drug addicts as the vessels involved in these patients are too long.So the most often used approach is revascularization with autogenous venous graft or artificial blood vessel transplant.
Arterial ligation for iliac-femoral pseudoaneurysm in drug addicts is prevalent in recent years,under the theory that drug abusers have profuse collateral branches at the puncture site.Salehian et al4analyzed 36 cases divided into two groups receiving arterial ligation and femoral arterial reconstruction respectively,and found that only 19%had developed intermittent claudication after ligation,proving arterial ligation to be a cost-effective therapy.Yegane et al5supported that femoral arterial reconstruction performed shortly after arterial ligation could be beneficial to improve intermittent claudication.We found that the incidence of intermittent claudication was higher in arterial ligation cases than that in femoral-popliteal arterial reconstruction.Therefore,if allowed in technique,reconstruction of blood vessels following the excision of iliac-femoral artery pseudoaneurysm would be beneficial to prognosis.6
Some drug abusers are suffering from deep venous thrombosis accompanied with phlebitis of saphenous vein.The femoral veins of some addicts with iliac-femoral artery pseudoaneurysm were occluded completely or even could not be detected.Therefore,their femoral veins were not appropriate for revascularization.However,appropriate greater saphenous veins were obtained in our study,indicating that autologous greater saphenous vein might be an access for venous drainage.Recanalization of autologous greater saphenous vein was found in 3 phlebitis patients.The vein,although thick in wall,could still be utilized as the material for bridging.
An optimal autologous greater saphenous venous graft is a prerequisite for arterial reconstruction in these patients.Klonaris et al7reported that internal iliac artery was used as grafting materials or patches in 12 cases because the autologous greater saphenous veins of the addicts were difficult to obtain.The single curved inguinal incision was adopted for all patients in our group,the distal end of which paralleled with Langer's lines.It was rather difficult to harvest vein trunks with little trauma and intact structure.Because of the high rate of complication of infection or rupture,transluminal interventional therapy should be carried out with caution.
Moreover,surgeons should be familiar with human immunodeficiency virus (HIV) diagnosis and treatment in order to prevent transmission of HIV and other infectious diseases during surgery.
1.Zheng YH,Liu CW,Guan H,et al.Surgical management of pseudoaneurysm from arteriovenous fistula for renal hemodialysis.Chin Med Sci J 2007;22:196-8.
2.Coughlin PA,Mavor AI.Arterial consequences of recreational drug use.Eur J Vasc Endovasc Surg 2006;32:389-96.
3.Guan H,Zheng YH,Li YJ,et al.Experience on surgical management of rupture of abdominal aortic aneurysm.Chin Med Sci J 2003;18:116-9.
4.Salehian MT,Shahid N,Mohseni M,et al.Treatment of infected pseudoaneurysm in drug abusers:ligation or reconstruction? Arch Iran Med 2006;9:49-52.
5.Yegane RA,Salehi NA,Ghaseminegad A,et al.Surgical approach to vascular complications of intravenous drug abuse.Eur J Vasc Endovasc Surg 2006;32:397-401.
6.Peirce C,Coffey JC,O'Grady H,et al.The management of mycotic femoral pseudoaneurysms in intravenous drug abusers.Ann Vasc Surg 2009;23:345-9.
7.Klonaris C,Katsargyris A,Papapetrou A,et al.Infected femoral artery pseudoaneurysm in drug addicts:the beneficial use of the internal iliac artery for arterial reconstruction.J Vasc Surg 2007;45:498-504.
杂志排行

Chinese Medical Sciences Journal的其它文章
- Sex Hormones and Androgen Receptor:Risk Factors of Coronary Heart Disease in Elderly Men△
- Comparison between Ophthalmologists and Community Health Workers in Screening of Shallow Anterior Chamber with Oblique Flashlight Test△
- Factors Influencing Pleural Effusion after Fontan Operation:an Analysis with 95 Patients
- Relationship between Carotid Atherosclerosis and Cerebral Infarction
- Expression of FLICE-inhibitory Protein in Synovial Tissue and Its Association with Synovial Inflammation in Juvenile Idiopathic Arthritis△
- A Case of Large“Silent”Extra-adrenal Retroperitoneal Paraganglioma Resected Laparoscopically