上颌前牵引联合FRⅢ矫治器在骨性Ⅲ类错牙合畸形患儿中的应用分析
2024-08-18张美玲杨琳
[摘要]目的:探讨上颌前牵引联合FRⅢ型矫治器矫治替牙期骨性Ⅲ类错牙合畸形患儿中的应用效果。方法:选取2019年12月-2021年6月笔者医院收治的92例骨性Ⅲ类错牙合畸形患儿作为研究对象,按照矫治方式将单一行上颌前牵引的患儿作为牵引组(n=43),将行上颌前牵引联合FRⅢ型矫治器治疗的患儿作为联合组(n=49),观察两组患儿治疗前及治疗1年后颌面部硬组织指标、软组织指标、牙性指标及舌骨位置变化情况。结果:治疗后,两组患儿的上牙槽座角(SNA)、下牙槽座角(SNB)、上下牙槽座角(ANB)、上颌骨位置(A-OLP)、下颌骨位置(Pg-OLP)、下颌平面与前颅底平面(SN)延长线所成角(MP-SN)、与眶耳平面(FH)所成角(MP-FH)及Y轴与FH平面相交内角(Y轴角)均较治疗前有所改善,且联合组改善情况优于牵引组(P<0.05)。治疗后,两组患儿下唇突点到审美平面距离(LL-EP)、鼻下点、鼻小柱点连线和鼻下点与上唇突点连线夹角(NLA)及面凸角(G-Sn-Pg)均较治疗前有所改善,且联合组改善情况优于牵引组(均P<0.05)。治疗后,两组患儿上中切牙长轴、鼻根点及上齿槽座点夹角(U1-NA)、上下中切牙垂直距离(覆牙合)及上下中切牙切缘投影距(覆盖)情况均较治疗前有所改善,且联合组改善情况优于牵引组(均P<0.05)。治疗后,两组患儿舌骨最前上点H到Y轴的距离(H-Y),H到X轴的距离(H-X)均较治疗前增大,且联合组高于牵引组(均P<0.05),两组患儿H到下颌平面距离(H-MP)及H到FH距离(H-FH)对比,差异无统计学意义(P>0.05)。结论:将上颌前牵引与FRⅢ型矫治器联合用于骨性Ⅲ类错牙合畸形患儿中,可有效改善患儿牙咬牙合关系及凹陷型侧貌,并促使其舌骨位置恢复正常。
[关键词]上颌前牵引;FRⅢ型矫治器;替牙期;骨性Ⅲ类错牙合畸形;软硬组织
[中图分类号]R783.5 [文献标志码]A [文章编号]1008-6455(2024)08-0063-04
Application of Maxillary Protraction Combined with FRⅢ Appliance in Children with Skeletal Class Ⅲ Malocclusion in Mixed Dentition
ZHANG Meiling, YANG Lin
( Department of Stomatology, the Third People’s Hospital of Chengdu, Chengdu 610000, Sichuan, China )
Abstract: Objective To investigate the application effects of maxillary protraction combined with FRⅢ appliance on children with skeletal Class Ⅲ malocclusion in mixed dentition. Methods 92 children with skeletal Class Ⅲ malocclusion who were treated in the author's hospital from December 2019 to June 2021 were selected as the research subjects. According to the correction methods, the children only with maxillary protraction were selected as traction group (n=43), and the children treated with maxillary protraction combined with FRⅢ appliance were included in combined group (n=49). The maxillofacial hard tissue indexes, soft tissue indexes, dental indexes and hyoid bone position of the two groups of children were observed before treatment and after 1 year of treatment. Results After treatment, the sella-nasion-point A(SNA) angle, sella-nasion-point B (SNB) angle, point A-nasion-point B (ANB) angle, maxillary position (A-OLP), mandibular position (Pg-OLP), angle formed with the mandibular plane and the extension line of sella-nasion line (SN) (MP-SN), angle formed with frankfort horizontal plane (FH) (MP-FH), and intersection angle of Y axis and FH plane (Y-axis angle) in both groups were improved compared with those before treatment, and the improvements in combined group were better than those in traction group (P<0.05). After treatment, the distance from the prominence of the lower lip to the esthetic plane (LL-EP), angle between the lower nasal point, the columellar point and the lower nasal point and the upper lip protrusion point (NLA) and facial convex angle (G-Sn-Pg) were improved in the two groups compared to before treatment, and the improvement status group were better in combined group (all P<0.05). After treatment, the angle between the long axis of the upper central incisor, the nasal root point and the upper alveolar point (U1-NA), the vertical distance (overlap) of the upper and lower central incisors, and the projection distance (overlap) of the upper and lower central incisors in the two groups were also improved compared with those before treatment, and the improvement status were better in combined group than traction group (all P<0.05). After treatment, the distance from hyoid anterior superior point H to Y axis (H-Y) and the distance from H to X axis (H-X) in both groups were prolonged compared with those before treatment, and the distances of combined group were longer than those in traction group (all P<0.05). There were no statistical differences in the distance from H to mandibular plane (H-MP) and the distance from H to FH (H-FH) between the two groups (P>0.05). Conclusion The combination of maxillary protraction and FRⅢ appliance in children with skeletal Class Ⅲ malocclusion can effectively improve the occlusal relationship and concave profile of children, and promote the normal recovery of position of hyoid bone.
Key words: maxillary protraction; FRⅢ appliance; mixed dentition; skeletal Class Ⅲ malocclusion; soft and hard tissues
骨性Ⅲ类错牙合畸形主要由上下颌骨矢状发育不协调引起,临床表现为前牙反牙合覆盖大,不能后退至切对切,磨牙近中关系,在青少年中较为常见,发病率为4.76%~12.6%[1]。因此类错牙合畸形患儿上颌发育不足及凸度变小,可导致其上唇呈塌陷状态,再加上下颌骨的过度发育导致患儿出现面高比例失调,呈典型的面中凹陷型颜面,在影响面部美观度的同时,可能引起患儿鼻腔及上气道狭窄,影响患儿呼吸功能、咀嚼功能或发音功能等,临床矫治较为棘手[2]。乳牙期及替牙期为矫治此类畸形的最佳时期,前方牵引及功能器矫治为改善牙列关系的主要方式,其中,前方牵引主要通过牵拉促进上颌骨骨缝间的骨质改建,牵引上颌骨向前下移位,促进其生理学位置的恢复,但研究发现,单一行上颌前牵引效果欠佳[3]。FRⅢ型矫治器为矫治Ⅲ类错牙合畸形常用的功能性矫治器,其在引导上颌向前发育的同时,可限制过度发育的下颌使骨体及颈部软组织向后改建,进而提高牵引效果[4]。基于此,本研究将上颌前牵引与FRⅢ型矫治器联合用于骨性Ⅲ类错牙合畸形患儿的临床矫治中,取得了满意效果,报道如下。
1 资料和方法
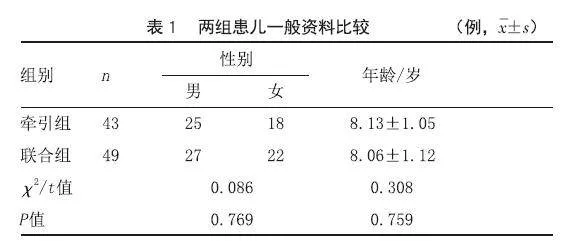
1.1 一般资料:选取2019年12月-2021年6月笔者医院收治的92例骨性Ⅲ类错牙合畸形患儿作为研究对象。纳入标准:①均符合骨性Ⅲ类错牙合畸形临床诊断[5];②低角或均角型Ⅲ类错牙合;③年龄6~12岁;④临床资料完整。排除标准:①有正畸治疗史;②颜面部手术史;③存在颌面部外伤或其他口腔疾病患儿。按照矫治方式将单一行上颌前牵引的患儿作为牵引组(n=43),将行上颌前牵引联合FRⅢ型矫治器SmK2ygyXKtG7Y/075AoXQuhtS6cZUWNI7+739cCerFs=治疗的患儿作为联合组(n=49),两组患儿一般资料比较差异无统计学意义(P>0.05),均衡可比,见表1。本研究获得医院伦理委员会批准通过。
1.2 治疗方法:牵引组给予上颌前牵引治疗。首先使用上颌螺旋扩弓器进行扩弓,将其置于患儿腭部中央位置,调整至合适水平及高度,第一前磨牙、磨牙配置带环,并于远中颊侧制作焊接牵引钩,将带环、牵引钩及扩弓器进行焊接固定,随后安装前方牵引面具进行前方牵引,调节牵引方向与平面呈20°~30°角,牵引力为450~600克/侧,两侧施力需均匀平行,每日牵引12 h以上,直至建立正常磨牙关系及牙合覆盖关系,牵引结束后佩戴活动保持器,平均疗程8个月。联合组在牵引组基础上联合FRⅢ型矫治器治疗,佩戴时间为结束牵引后,将口内牵引装置拆除,常规制作并戴用FRⅢ型矫治器,每日佩戴8~10 h,配合唇肌封闭训练,平均疗程8个月。
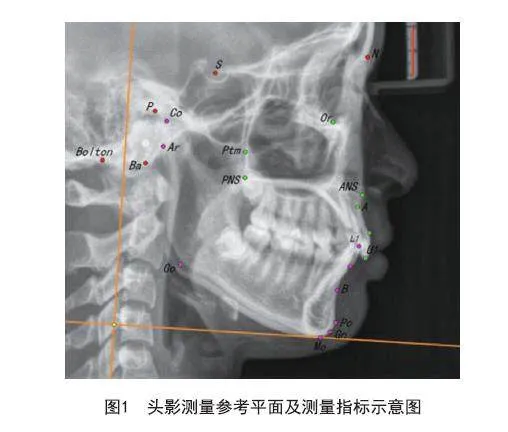
1.3 观察指标:取两组患儿治疗前、治疗1年后头颅侧位X线片进行相关指标测量。①硬组织指标:测量两组患儿蝶鞍点、鼻根点及上齿槽座点夹角,即上牙槽座角(SNA);蝶鞍点、鼻根点及下齿槽座点夹角,即下牙槽座角(SNB);上、下牙槽座及鼻根点连线夹角,即上下牙槽座角(ANB);上齿槽座点与OLP线的垂直距离,即上颌骨位置(A-OLP);下颌颏部最前点与OLP线的垂直距离,即下颌骨位置(Pg-OLP);下颌平面与前颅底平面(SN)延长线所成角(MP-SN),与眶耳平面(FH)所成角(MP-FH)及Y轴与FH平面相交内角(Y轴角)。②软组织指标:测量两组患儿下唇突点到审美平面距离(LL-EP);鼻下点、鼻小柱点连线和鼻下点与上唇突点连线夹角(NLA);软组织眉间点、鼻下点、颏前点形成的夹角,即面凸角(G-Sn-Pg)。③牙性指标:测量两组患儿上中切牙长轴、鼻根点及上齿槽座点夹角(U1-NA);上下中切牙垂直距离(覆牙合)及上下中切牙切缘投影距(覆盖)。④舌骨位置变化情况:测量舌骨最前上点H到Y轴的距离(H-Y),H到X轴的距离(H-X),H到下颌平面距离(H-MP),H到FH距离(H-FH)。头影测量参考平面及测量指标示意图见图1。
1.4 统计学分析:选用SPSS 21.0统计软件处理数据,计数资料表示为n(%),选用χ2检验,计量资料(x¯±s)表示,应用t检验,疗效对比使用秩和检验,P<0.05为差异具统计学意义。
2 结果
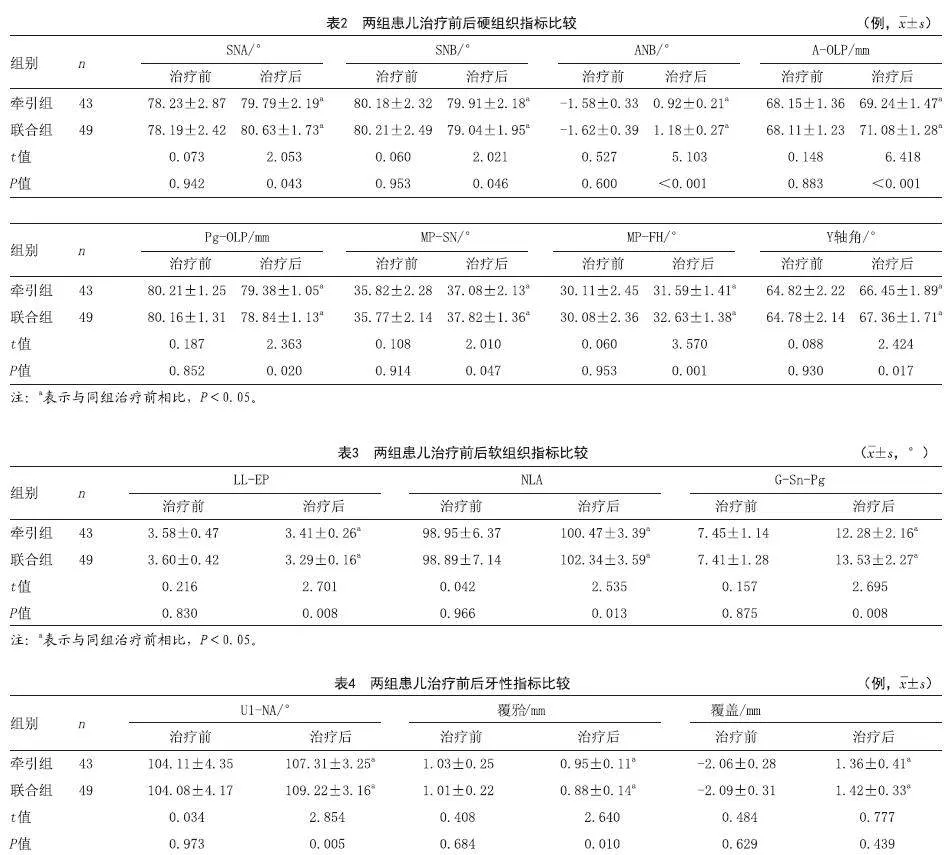
2.1 两组患儿治疗前后硬组织指标比较:治疗后,两组患儿的SNA、SNB、ANB、A-OLP、Pg-OLP、MP-SN、MP-FH及Y轴角均较治疗前有所改善,且联合组改善情况优于牵引组(P<0.05),见表2。
2.2 两组患儿治疗前后软组织指标:治疗后,两组患儿LL-EP、NLA及G-Sn-Pg均较治疗前有所改善,且联合组改善情况优于牵引组(均P<0.05),见表3。
2.3 两组患儿治疗前后牙性指标对比:治疗后,两组患儿U1-NA、覆牙合及覆盖情况均较治疗前有所改善,且联合组改善情况优于牵引组(均P<0.05),见表4。
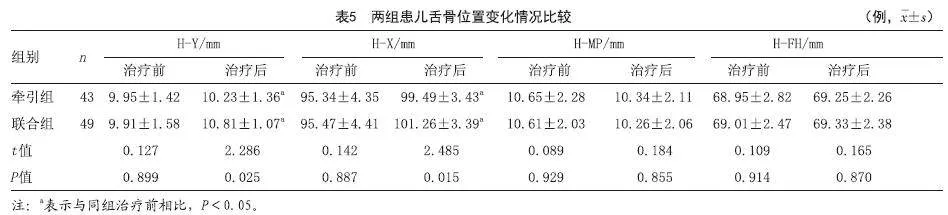
2.4 两组患儿舌骨位置变化情况比较:治疗后,两组患儿H-Y及H-X距均较治疗前增大,且联合组高于牵引组(均P<0.05),两组患儿H-MP及H-FH对比,差异无统计学意义(P>0.05),见表5。
3 讨论
骨性Ⅲ类错牙合畸形多因上颌发育不足或下颌发育过度所致,具有发病率高、畸形严重及矫治困难等特点,在我国发病率高达15%左右[6]。因存在面高比例失调、下牙弓及下颌后移,存在此类畸形患者常呈“地包天”面型,严重影响其面部外观及口腔功能[7]。研究显示[8],25%~57%的骨性Ⅲ类错牙合畸形患儿可能存在鼻腔和上气道狭窄,由此引发的鼾症及阻塞性呼吸睡眠暂停综合征严重影响患儿日常生活。乳牙期及替牙期患儿处于颌骨发育期,为矫治此类畸形的重要时期,因该阶段骨组织可塑性较强,在外界矫正力量的作用下易发生改建,能够及时纠正不良骨骼关系,有效引导患儿颌面结构向正常型生长发育。
上颌前牵引及功能矫治器均可用于上颌后缩或伴有上颌后缩病例的临床矫治,为治疗骨性Ⅲ类错牙合畸形的常见手段。其中,上颌前牵引通过牵拉作用能够使上颌骨随牵引方向向前移动,以改善上颌后缩,而在此之前常配合上颌扩弓以有效扩展上颌骨缝,为后续纠正上下颌骨矢状方向不协调奠定基础[9]。功能矫治器的矫治效果主要为促进患儿牙性指标的改善,其主要通过改善上切牙唇倾度及下切牙舌倾度来改善牙齿咬合,进而改善患儿侧貌[10]。本研究中,经治疗两组患儿软硬组织及相关牙性指标均得到一定改善,但联合组改善情况优于牵引组,提示与单一行上颌前牵引治疗相比,其与FRⅢ型矫治器的联合使用对骨性Ⅲ类错牙合畸形患儿的临床疗效更佳,能够有效改善患儿咬牙合关系及侧貌。上颌前牵引主要利于颌骨生长潜力进行改良治疗,其主要通过对骨缝施加重力牵引以促进骨缝区骨改建,并配合适当扩弓使骨缝连接扩展,促进新骨生成,刺激上颌骨前部骨膜牵张,以促进上颌骨向前生长。王鹏等[11]也通过研究证实上颌骨前牵引可有效改善骨性Ⅲ类错牙合畸形患者侧貌外形,并指出其能够解除下颌对上颌的锁结关系,使正常咬合关系建立,在刺激上颌生长的同时也抑制了下颌的过度生长,矫治效果显著。但冉碧红等[12]通过研究发现,单一的上颌前牵引矫治效果不佳,如上颌前牵引能够引导上颌复合体向前生长,但因所施加的作用力较为单一,无法完全促使上颌骨与下颌骨完全恢复至协调状态,口周异常肌力亦不能完全解除,错牙合畸形生长改良改建难以全部完成。FRⅢ型矫治器的使用在一定程度上弥补了此类不足,其能够在上颌前牵引的基础上给予下颌向后下方旋转的作用力,故若上颌前移量不足,其可通过增加下颌后移量来使颜面外貌更为协调。此外,FRⅢ型矫治器具备上颌唇挡和颊盾,在利用骨膜牵张力促使牙弓、颌骨生长发育的同时,一定程度上可避免口周唇、颊的肌肉功能及舌的运动功能对颌骨发育产生的影响,能够促使上下颌骨最大限度恢复至正常协调状态,有利于错牙合畸形的生长改良改建[13]。
临床研究发现,Ⅲ类错牙合畸形患者舌骨位置较高,有向上移位趋势,且舌骨位置更靠前,这种位移是造成错牙合的原因之一[14]。而本研究结果显示,治疗后,两组患儿H-Y及H-X距均较治疗前增大,且联合组高于牵引组,提示上颌前牵引与FRⅢ型矫治器的联合使用一定程度上可促进舌骨位置恢复正常。一方面,上颌骨前牵引能够牵拉唇肌,使其保持向前移位,而下颌因外物在口内的作用改变了牵拉过程中口面肌对牙齿和骨骼的施力大小及方向,有利于牙合发育及颅面生长,因而舌骨肌群功能发生改建。与此同时,佩戴FRⅢ型矫治器患儿在吞咽时需依靠舌来固定并保持矫治器位置,在此过程中提下颌肌的反复收缩,有利于正常牙齿接触吞咽的建立,舌也得到反复训练,有利于舌骨恢复正常位置。Liu Y等[15]研究指出,FRⅢ型矫治器使Ⅲ类错牙合畸形患者下颌骨发生顺时针旋转,其舌骨位置向后下方向产生位移,一定程度上可减轻舌骨位置对颌面发育的影响。
综上所述,将上颌前牵引与FRⅢ型矫治器联合用于骨性Ⅲ类错牙合畸形患儿中,可有效改善患儿牙咬牙合关系及凹陷型侧貌,并促使其舌骨位置恢复正常,有一定的临床推广价值。
[参考文献]
[1]Lin M, Xie C, Yang H, et al. Prevalence of malocclusion in Chinese schoolchildren from 1991 to 2018: A systematic review and meta-analysis[J]. Int J Paediatr Dent,2020,30(2):144-155.
[2]Galeotti A, Martina S, Viarani V, et al. Cephalometric effects of Pushing Splints 3 compared with rapid maxillary expansion and facemask therapy in Class Ⅲ malocclusion children: a randomized controlled trial[J]. Eur J Orthod, 2021,43(3):274-282.
[3]de Souza R A, Rino Neto J, de Paiva J B. Maxillary protraction with rapid maxillary expansion and facemask versus skeletal anchorage with mini-implants in class Ⅲ patients: a non-randomized clinical trial[J]. Prog Orthod, 2019,20(1):35.
[4]Lyu L, Lin H, Huang H. The effect of combined maxillary pad movable appliance and FR-III functional appliance in the treatment of skeletal Class III malocclusion of deciduous teeth[J]. BMC Oral Health, 2022,22(1):485..
[5]赵志婷,范存晖,杨茜,等.替牙期骨性Ⅲ类错牙合儿童上气道形态及舌骨位置的X线头影测量[J].青岛大学医学院学报,2013,49(3):252-255.
[6]张东强,杜星颜,王敏,等.微型种植钉支抗治疗Ⅲ类错牙合畸形的临床研究[J].中国美容医学,2021,30(1):109-112..
[7]Liu Y, Hou R, Jin H, et al. Relative effectiveness of facemask therapy with alternate maxillary expansion and constriction in the early treatment of Class III malocclusion[J]. Am J Orthod Dentofacial Orthop, 2021,159(3):321-332.
[8]陈虹羽,赖文莉.McNamara分析法对正畸正颌联合治疗骨性Ⅲ类错牙合畸形的疗效评价[J].温州医科大学学报,2022,52(1):61-64.
[9]韩雪,张凡柯,李小兵.2种扩弓方式对骨性Ⅲ类患者上颌前牵引疗效影响的meta分析[J].北京口腔医学,2022,30(3):206-211.
[10]于晓艳,江淑敏,张晓红.上颌前方牵引联合快速扩弓对替牙晚期骨性Ⅲ类错牙合患者颊旁间隙的影响[J].中国美容医学,2021,30(3):79-82.
[11]王鹏,苏哲君,张兴乐,等.改良前方牵引矫治器治疗上颌后缩畸形患者的疗效观察[J].河北医学,2018,24(12):2029-2032.
[12]冉碧红,赵军,龙晓玲.上颌前牵引联合FRⅢ型矫治器保持对儿童生长发育期骨性Ⅲ类错牙合畸形的疗效[J].实用临床医药杂志,2020,24(18):18-21.
[13]Yeon B M, Lee N K, Park J H, et al. Comparison of treatment effects after total mandibular arch distalization with miniscrews vs ramal plates in patients with Class III malocclusion[J]. Am J Orthod Dentofacial Orthop, 2022,161(4):529-536.
[14]邹茵,付巧梅,徐贤寅.儿童安氏Ⅰ、Ⅱ、Ⅲ类错牙合畸形患者舌体积、舌骨位置、气道容积及颌面部形态的关系[J].上海口腔医学,2020,29(6):632-637.
[15]Liu Y, Yang K. Three-dimensional changes in the upper airway and craniomaxillofacial morphology of patients with Angle Class III malocclusion treated with a Frankel III appliance[J]. BMC Oral Health, 2021,21(1):634.
[收稿日期]2022-11-21
本文引用格式:张美玲,杨琳.上颌前牵引联合FRⅢ矫治器在骨性Ⅲ类错牙合畸形患儿中的应用分析[J].中国美容医学,2024,33(8):63-67.
