Application of three-dimensional speckle tracking technique in measuring left ventricular myocardial function in patients with diabetes
2024-04-22ZhengLiYingQianChunYunFanYongHuang
Zheng Li,Ying Qian,Chun-Yun Fan,Yong Huang
Abstract BACKGROUND Diabetic cardiomyopathy is considered as a chronic complication of diabetes mellitus (DM).Therefore,early detection of left ventricular systolic function (LVSF) damage in DM is essential.AIM To explore the use of the three-dimensional speckle tracking technique (3D-STI) for measuring LVSF in DM patients via meta-analysis.METHODS The electronic databases were retrieved from the initial accessible time to 29 April 2023.The current study involved 9 studies,including 970 subjects.We carried out this meta-analysis to estimate myocardial function in DM compared with controls according to myocardial strain attained by 3D-STI.RESULTS Night articles including 970 subjects were included.No significant difference was detected in the left ventricular ejection fraction between the control and the diabetic group (P > 0.05),while differences in global longitudinal strain,global circumferential strain,global radial strain,and global area strain were markedly different between the controls and DM patients (all P < 0.05).CONCLUSION The 3D-STI could be applied to accurately measure early LVSF damage in patients with DM.
Key Words: Diabetes mellitus;Left ventricular systolic dysfunction;Three-dimensional speckle tracking echocardiography;Meta analysis
INTRODUCTION
Diabetes mellitus (DM) is a common disease in China.Long-term poor blood glucose control can cause multisystem damage and a series of chronic complications[1].Diabetic cardiomyopathy (DCM) is a chronic complication and is a serious cause of poor prognosis in individuals with DM[2].Additionally,numerous reports have suggested that DM could elevate the occurrence of cardiac disorders,hypertension,and other illnesses and could worsen coronary artery illness[3].Therefore,early detection of left ventricular systolic function (LVSF) damage in DM patients is essential.
Currently,the routine clinical factor for assessing cardiac function is left ventricular ejection fraction (LVEF).However,LVEF is strongly affected by subjectivity,and several publications have exposed that LVEF could not indicate the severity of LVSF in patients with earlier DM.Moreover,it is impossible to effectively predict patients with segmental wall motion abnormalities and ejection fraction retention by LVEF.Therefore,evaluating left ventricular myocardial function is highly important for the diagnosis,treatment,and prognosis of heart disease.The 3D-STI is an innovative approach for evaluating cardiac motor function.It tracks myocardial motion from three-dimensional space through detecting myocardial echo speckle signals,which breaks through the limitation of the two-dimensional plane of 2D-STI and can evaluate cardiac function more accurately.
The 3D-STI is of great value in the assessment of primary or secondary LVSF.However,the ability of the 3D-STI to evaluate the outcome of left ventricular myocardial contractile function (LVMCF) in DM remains uncertain,and additional reports are needed.The purpose of the current analysis was to examine the ability of the 3D-STI to early predict LVSF damage in DMviameta-analysis.
MATERlALS AND METHODS
Screening of articles
The meta-analysis was registered (202390079) in INPLASY and followed the preferred reporting criteria of PRISMA 2020.A comprehensive exploration of studies on 3D-STI assessment in DM patients was conducted based on the PRISMA 2020 recommendations.Through the PubMed,Embase,Scopus,and Cochrane Library databases,studies on 3D-STI assessment in DM patients were retrieved from the initial obtainable time to 29 April 2023.The exploration strategy was employed based on the following terms: (1) “Three-dimensional speckle tracking”,“3D-speckle tracking”,“3D-STI”,or “STE”;(2) “Diabetes mellitus” or “DM”;and (3) “left ventricular” or “LV”.The current study conducted a meta-analysis.
Data extraction and quality evaluation
Full-text articles that included the main factors were eligible for inclusion in this study.The main factors were as follows: (1) Had a randomized controlled trial and cohort study;(2) had an article comparing LVMCF parameters between the DM group and control group;(3) had no history of cardiovascular syndromes;(4) had a diagnostic approach of 3D-STI;and (5) had at least one notable result,including global longitudinal strain (GLS),global circumferential strain (GCS),global radial strain (GRS),and global area strain (GAS).
Repeated documents and publications that did not supply original descriptions of interest,such as case reports,meeting essays,reviews,fundamental studies,and nonrelevant publications,were eliminated.Two researchers individually assessed the selected articles followed the selection criteria.Divergences between researchers were resolved by an agreement obtained from the assist of a third author.
The quality of the publications was considered with the New-Ottawa Scale and evaluated based on the following features: The comparison of the case and control groups,and the estimation of the consequences.The quality of the chosen studies was estimated individually by two investigators,and the incongruity was determined by discussion.
Risk of bias evaluation and sensitivity analysis
Publication bias was estimated through Egger’s test for the included articles.The random effects approach was used to minimize the variability among the included publications.The stability of the strains was measured through sensitivity analysis by eliminating one by one from the article.
Statistical analysis
The weighted mean difference and 95% confidence interval (95%CI) were employed to depict the statistical consequences of continuous variables.Heterogeneity was measured through RevMan 5.3 software and theI2test.AnI2< 25% indicated low heterogeneity,while a value > 50% implied high heterogeneity.The random-effects model was employed and checked with the fixed-effects model.Sensitivity analyses were carried out through the leave-one-out method.A difference was statistically significant atP< 0.05.
RESULTS
Study searching and selection
Two hundred and eighty-six articles were obtained from the above databases using a retrieval strategy.Sixty duplicated studies were excluded.Moreover,studies without suitable information,including meeting articles (123),reviews (27),fundamental studies (2),case reports (18),and nonrelational studies (28),were disqualified.After the full texts were read,19 studies were rejected due to lack of statistics.Ultimately,the remaining 9 articles were involved.The article collection process is exhibited in Figure 1 and Table 1.
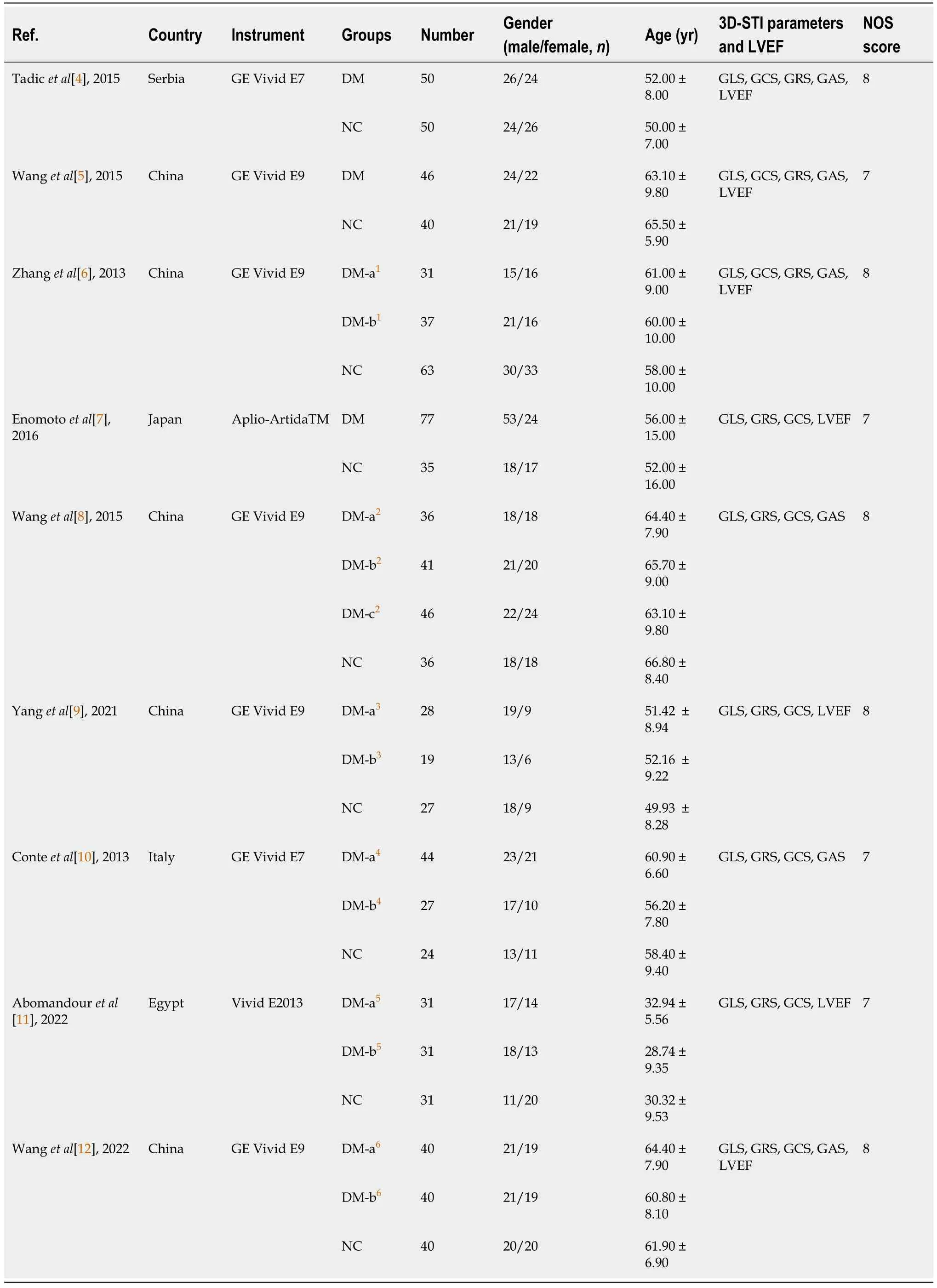
Table 1 General data and quality evaluation of the included studies
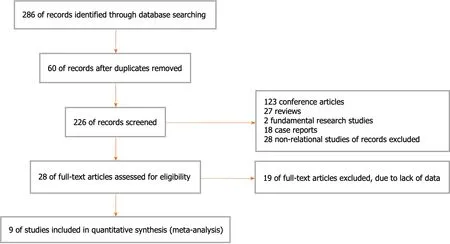
Figure 1 Study selection procedure.
Comparison of the LVMCF based on LVEF
In total,7 articles compared the LVEF measured by 3D-STI between the DMs and controls.The findings showed that the difference in LVEF between DMs and healthy controls was not statistically significant (MD: -1.85,95%CI: -2.48 to -1.22,P=0.46;I2=0%;Figure 2).

Figure 2 Forest plot showing the comparison of the left ventricular myocardial contractile function between diabetes mellitus and controls based on left ventricular ejection fraction. 95%CI: 95% confidence interval.
Comparison of the LVMCF based on GLS
Furthermore,all 9 included studies reported GLS in DM patients and healthy controls.The results demonstrated that the LVGLS (MD: 1.41,95%CI: 1.11 to 1.71,P=0.000;I2=94%;Figure 3) was appreciably lower in the DMs than in the controls.
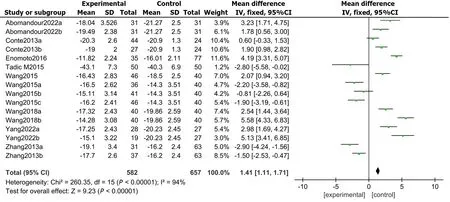
Figure 3 Forest plot showing the comparison of the left ventricular myocardial contractile function between diabetes mellitus and controls based on global longitudinal strain. 95%CI: 95% confidence interval.
Comparison of LVMCF based on GCS
There were 9 articles recording the GCS score in patients with DM and controls.The results demonstrated that the LVGCS (MD: 0.02,95%CI: -0.36 to 0.39,P=0.000;I2=92%;Figure 4) was markedly lower in the DMs than in the controls.

Figure 4 Forest plot comparing the left ventricular myocardial contractile function between diabetes mellitus and controls based on the global circumferential strain score. 95%CI: 95% confidence interval.
Comparison of LVMCF based on GRS
All 9 included studies reported GRSs in DM patients and healthy controls.The results demonstrated that the LVGRS (MD: -1.61,95%CI: -2.33 to -0.89,P=0.000;I2=88%;Figure 5) was markedly impaired in the DMs compared with the controls.
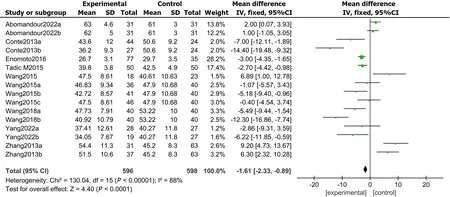
Figure 5 Forest plot showing the comparison of left ventricular myocardial contractile function between diabetes mellitus and controls based on global radial strain. 95%CI: 95% confidence interval.
Comparison of LVMCF based on GAS
In total,6 articles compared the GASs measured by 3D-STI between the DM and the control group.The results exposed that GAS was markedly impaired in DMs compared with controls (MD: 0.14,95%CI: -0.33 to 0.61,P=0.000;I2=90%;Figure 6).
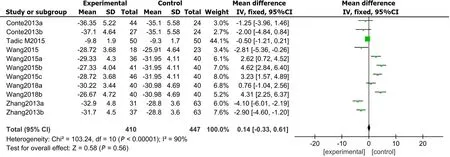
Figure 6 Forest plot showing the comparison of left ventricular myocardial contractile function between diabetes mellitus and controls based on global area strain. 95%CI: 95% confidence interval.
Risk of bias assessment and sensitivity analysis
Publication bias was evaluated through Egger’s test for the involved studies (Figure 7).We detected no publication bias in GLS (P=0.286) or LVEF (P=0.825).Moreover,there was publication bias for the GRS (P=0.022),GCS (P=0.032),and GAS (P=0.041).The trim-and-fill approach was further employed to find the modified merged values for the GRS,GCS,and GAS.A sensitivity analysis was also carried out to evaluate the stability of the strains.None of the articles confirmed a marked influence on the merged value,implying that the involved publications exhibited worthy stability.
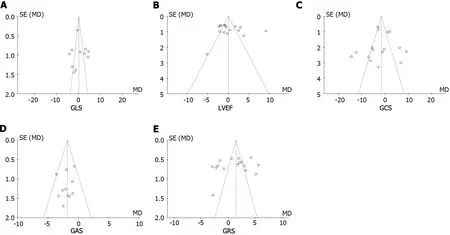
Figure 7 Risk of bias assessment for global longitudinal strain,left ventricular ejection fraction,global circumferential strain,global area strain,and global radial strain. A: Global longitudinal strain;B: Left ventricular ejection fraction;C: Global circumferential strain;D: Global area strain;E: Global radial strain.GLS: Global longitudinal strain;LEVF: Left ventricular ejection fraction;GCS: Global area strain;GAS: Global area strain;GRS: Global radial strain.
DISCUSSION
In the early stage of DCM,due to abnormal metabolism of subendothelial cardiomyocytes and more severe hypoxia,myocardial fibers are first affected[13].When damaged,the strain parameter GLS reflects myocardial mechanics abnormalities[14].However,due to the inconsistency of the duration of disease and the degree of blood glucose control in different patients,GLS and other left ventricular systolic strain parameters (GCS,GRS,and GAS) can decrease at the same time or successively[15].Therefore,the application of appropriate and accurate diagnostic tools to detect and monitor myocardial injury is an important aspect of managing DCM patients.
Conventional echocardiography is the most frequently used imaging approach for measuring and evaluating left ventricular function[16].Evaluation of left ventricular function according to the LVEF has been widely used in the clinic[17].The use of strain imaging of the myocardium opens a new window for the study of myocardial mechanics.Strain measurement according to the myocardial mechanics of the left ventricle can quickly and effectively evaluate changes in myocardial contractility[18].Speckle tracking imaging (STI) tracks myocardial tissue signals frame by frame through the principle of “block matching”,without significant displacement between adjacent frames,and can evaluate myocardial motion and quantify changes in cardiac function without angle dependence[19].With the emergence of 2D-STI,the abovementioned left ventricular myocardial strain parameters can be measured quantitatively[20].3D-STI combines realtime three-dimensional echocardiography and STI and can track myocardial tissue signals in three-dimensional space without the limitation of planes,which compensates for the deficiency of 2D-STI[21].This is the first meta-analysis evaluating the clinical utility of the 3D-STI for assessing LVMCF in patients with DM.
The consensus is that the LVEF is the stroke volume after the standardized change in left ventricular volume.It is a frequently used parameter for the clinical assessment of LVSF.At present,magnetic resonance imaging is considered the gold standard for detecting LVSF[22].The findings of this meta-analysis implied that there were anomalous alterations in left ventricular myocardial mechanics in DM patients without a significant decrease in LVEF.In addition,3D-STI can yield parameters such as the GRS,GLS,GAS,GCS,and 3D-strain.Saeedietal[23] reported that GLS,GRS,GCS and GAS were decreased in DM compared with those in the control group.Baberetal[24] reported that there was no marked difference in GGS or GRS between DMs and controls,but the GLS and GAS were considerably lower than those in controls.
The consequences of our meta-analysis indicated that the GLS,GRS,GCS,and GAS in DMs were decreased compared with those in controls,suggesting that the LVSF in DMs was impaired compared with that in controls.The decreases in GLS and GAS were more obvious,possibly because the left ventricular wall is composed of three layers of myocardial fibers.The subepicardial myocardial fibers are arranged counterclockwise oblique in the direction of the left ventricular longitudinal axis,approximately circular in the middle layer of the ventricular wall,and clockwise in the longitudinal axis to the innermost layer,namely,the subendocardial layer.The diversity of myocardial fiber arrangement determines the complexity of left ventricular three-dimensional motion[25].GLS represents the ability of the heart to move in the long axis direction and is caused by the contraction of longitudinal muscle fibers under the endocardium.These muscle fibers have the characteristics of strong contractility and high demand for oxygen,which may be the reason why longitudinal strain is more sensitive than that in other directions of the left ventricle during mild hypoperfusion of the subendocardial myocardium in the early stage of diabetes[26].The GRS and GCS are mainly affected by the contractility of annular fibers in the middle layer of the myocardium.The GAS reflects the rate of change in the endocardial area from the initial area to the area after deformation;this metric is a strain index integrated with longitudinal and circumferential strain,is inversely proportional to the radial strain,and can be regarded as the composite of GLS and GRS[27].As reported previously,the GAS has the best correlation with LVSF[28].Wangetal[29] suggested that the GAS could offer a more precise basis for quantifying global and local myocardial function with good reproducibility.Chenetal[30] reported that there was a negative correlation between GAS and GLS and between GAS and hemoglobin A1c,among which GAS had the strongest correlation.Additionally,another study confirmed that the GAS can provide a more accurate basis and good reproducibility for quantifying global and local myocardial function[31].
The present meta-analysis has several limitations.Firstly,the studies included in this meta-analysis included diseases such as hypertension or obesity in DM patients and good or poor control of blood glucose levels in DM patients.Therefore,there might be selection bias.Second,only 8 articles were involved in this study,and the sample size was rather small,so the results might be affected.However,we strictly established the selection criteria for the articles and strictly evaluated the quality of the studies to improve the overall quality of the meta-analysis and the credibility of the results.
CONCLUSlON
In conclusion,the 3D-STI might be used to precisely calculate early LVSF in patients with DM.The measurement of left ventricular strain in DM patients through 3D-STI could estimate the LVSF damage in patients with early diabetes.
ARTlCLE HlGHLlGHTS
Research background
Diabetic cardiomyopathy is a chronic complication,which is a critical reason of poor prognosis and even death in patients with diabetes mellitus (DM).Additionally,numerous reports have implied that DM could raise the occurrence of heart disorder,hypertension,and other illnesses,and could worsen coronary artery illness.Therefore,early detection of left ventricular systolic function (LVSF) damage in DM,necessary treatment is especially essential.Three-dimensional speckle tracking technique (3D-STI) is of beneficial worth in the assessment of primary or secondary LVSF.However,the 3D-STI evaluating capability of left ventricular myocardial contractile function (LVMCF) in DM remains uncertain and further reports are needed.
Research motivation
To explore the application value of 3D-STI in assessing LVMCF in DM by meta-analysis.
Research objectives
To investigate the assessment of 3D-STI in estimating early left ventricular systolic dysfunction in DM by meta-analysis.3D-STI provides a feasible and accurate new technique for clinical measurement of LVSF in left ventricular caused by DM,which might play an important role in the evaluation of cardiac function injury.
Research methods
We carried out a meta-analysis to evaluate myocardial function in patients with DM compared with controls according to myocardial strain attained by 3D-STI.We searched he PubMed,Embase,Scopus databases,and the Cochrane library from the initial accessible time to 29 April 2023.PRISMA guidelines were used.Data for meta-analysis were pooled using a random-effects model.We extracted data and used the Cochrane “Risk of bias” tool to assess methodological quality.Effect was presented as mean difference with 95% confidence interval using RevMan 5.3.The current study is the first meta-analysis to report that 3D-STI could precisely assess early left ventricular systolic dysfunction in DM.
Research results
The findings of this meta-analysis implied that there existed anomalous alterations in left ventricular myocardial mechanics in DM without a significant decrease in LVEF.In addition,3D-STI could obtain parameters such as GRS,GLS,GAS,GCS,3D-Strain and so on.Among them,the decrease of GLS and GAS was more obvious,which may be since the left ventricular wall is composed of three layers of myocardial fibers: The subepicardial myocardial fibers are arranged counterclockwise oblique in the direction of the left ventricular longitudinal axis,approximately circular in the middle layer of the ventricular wall,and clockwise in the longitudinal axis to the innermost layer,namely the subendocardial layer.
Research conclusions
Our data provided the first evidence for the essential role of 3D-STI in assessing the early left ventricle systolic dysfunction in DM precisely.The assessment of left ventricular strain in DM patients through 3D-STI might estimate the damage of LVSF in DM in the early stage.
Research perspectives
We believe that with the continuous improvement of computer and three-dimensional ultrasound technology,the shortcomings will be overcome,and 3D-STI is expected to become the gold standard for clinical non-invasive determination of LVSF.
FOOTNOTES
Author contributions:Li Z and Qian Y were responsible for the study concept and designed the systematic review protocol;Qian Y and Huang Y performed the study selection and data extraction;Li Z and Fan CY performed the statistical analyses;Qian Y and Huang Y prepared the outlines and wrote the manuscript;and all the authors have contributed to the completion of this paper.
Conflict-of-interest statement:No conflicts of interest exit in the submission of this manuscript.
PRlSMA 2009 Checklist statement:The authors have read the PRISMA 2009 Checklist,and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Yong Huang 0009-0001-1989-8223.
S-Editor:Chen YL
L-Editor:A
P-Editor:Chen YX
杂志排行

World Journal of Diabetes的其它文章
- Nε-carboxymethyl-lysine and inflammatory cytokines,markers and mediators of coronary artery disease progression in diabetes
- Non-pharmacological interventions for diabetic peripheral neuropathy: Are we winning the battle?
- Application and management of continuous glucose monitoring in diabetic kidney disease
- Role of renin-angiotensin system/angiotensin converting enzyme-2 mechanism and enhanced COVlD-19 susceptibility in type 2 diabetes mellitus
- Are treatment options used for adult-onset type 2 diabetes mellitus (equally) available and effective for children and adolescents?
- Prevalence and risk factors of wound complications after transtibial amputation in patients with diabetic foot