lmpact of open hepatectomy on postoperative bile leakage in patients with biliary tract cancer
2024-03-07GangWuWenYingLiYuXingGongFengLinChenSun
Gang Wu,Wen-Ying Li,Yu-Xing Gong,Feng Lin,Chen Sun
Abstract BACKGROUND Bile leakage is a common and serious complication of open hepatectomy for the treatment of biliary tract cancer.AIM To evaluate the incidence,risk factors,and management of bile leakage after open hepatectomy in patients with biliary tract cancer.METHODS We retrospectively analyzed 120 patients who underwent open hepatectomy for biliary tract cancer from February 2018 to February 2023.Bile leak was defined as bile drainage from the surgical site or drain or the presence of a biloma on imaging.The incidence,severity,timing,location,and treatment of the bile leaks were recorded.The risk factors for bile leakage were analyzed using univariate and multivariate logistic regression analyses.RESULTS The incidence of bile leak was 16.7% (20/120),and most cases were grade A (75%,15/20) according to the International Study Group of Liver Surgery classification.The median time of onset was 5 d (range,1-14 d),and the median duration was 7 d (range,2-28 d).The most common location of bile leakage was the cut surface of the liver (70%,14/20),followed by the anastomosis site (25%,5/20) and the cystic duct stump (5%,1/20).Most bile leaks were treated conservatively with drainage,antibiotics,and nutritional support (85%,17/20),whereas some required endoscopic retrograde cholangiopancreatography with stenting (10%,2/20) or percutaneous transhepatic cholangiography with drainage (5%,1/20).Risk factors for bile leakage include male sex,hepatocellular carcinoma,major hepatectomy,blood loss,and blood transfusion.CONCLUSION Bile leakage is a frequent complication of open hepatectomy for biliary tract cancer.However,most cases are mild and can be conservatively managed.Male sex,hepatocellular carcinoma,major hepatectomy,blood loss,and blood transfusion were associated with an increased risk of bile leak.
Key Words: Open hepatectomy;Bile leak;Biliary tract cancer;Risk factors;Management;Complication
lNTRODUCTlON
Biliary tract cancer is a rare but aggressive malignancy originating from the epithelium of the intrahepatic or extrahepatic bile ducts or the gallbladder[1,2].The incidence and mortality rates of biliary tract cancer vary widely according to the geographic region,with the highest rates occurring in Asia and Eastern Europe[3].The primary treatment for biliary tract cancer is surgical resection,which offers a chance for cure and long-term survival[4,5].However,surgery for biliary tract cancer is often complex and challenging,especially when employing major hepatectomy or hilar dissection[6].
Bile leakage is a common and serious complication of hepatectomy for biliary tract cancer[7,8].It can cause abdominal pain,fever,infection,biloma formation,delayed wound healing,prolonged hospital stays,increased morbidity and mortality,and impaired quality of life.The reported incidence of bile leak after hepatectomy ranges from 3% to 27% depending on the definition,diagnosis,and classification criteria[9].Several risk factors for bile leakage after hepatectomy have been identified,including the tumor location,extent of resection,operative time,blood loss,liver function,biliary pressure,surgical techniques,and drainage management[10].
Bile leakage is diagnosed based on clinical signs and symptoms,biochemical tests,imaging studies,and endoscopic or percutaneous interventions[11].Treatment depends on the severity,timing,location,and source of bile leakage[11].The International Study Group of Liver Surgery (ISGLS) has proposed a classification system for bile leak after hepatectomy based on the clinical impact and the need for therapeutic interventions[12].According to this system,bile leaks can be classified into three grades: grade A,bile leaks that do not require any change in the initial treatment plan;grade B,bile leaks that require a change in the initial treatment plan but can be managed without laparotomy;and grade C,bile leaks that require laparotomy.
Open hepatectomy is a conventional surgical approach for biliary tract cancer that allows direct visualization and manipulation of the liver and bile ducts.However,open hepatectomy is associated with a higher risk of bile leakage than laparoscopic or robotic hepatectomy.This is because of the larger cut surface of the liver,longer operative time,and greater blood loss[13].Therefore,it is important to evaluate the effect of open hepatectomy on postoperative bile leakage in patients with biliary tract cancer and identify optimal management strategies for this complication[14].
We retrospectively analyzed 120 patients who underwent open hepatectomy for biliary tract cancer at our institution from February 2018 to February 2023.We aimed to assess the incidence,risk factors,and management of bile leak after open hepatectomy for biliary tract cancer and to provide suggestions for improving surgical outcomes.
MATERlALS AND METHODS
Study design and population
This retrospective cohort study was conducted at a tertiary referral center.We reviewed the medical records of 120 patients who underwent open hepatectomies for biliary tract cancer from February 2018 to February 2023.Biliary tract cancer was defined as a malignant tumor arising from the intrahepatic or extrahepatic bile ducts or the gallbladder.Diagnosis of biliary tract cancer was confirmed by histopathological examination of the resected specimens.The inclusion criteria were age ≥ 18 years,performance status 0-2,Child-Pugh class A or B,no evidence of distant metastasis,no previous history of liver surgery or liver transplantation,and no concomitant extrahepatic bile duct resection.The exclusion criteria included incomplete medical records,conversion to laparoscopic or robotic hepatectomy,intraoperative death,or postoperative death within 30 d.The Institutional Review Board approved the study protocol and waived the requirement for informed consent owing to the retrospective nature of the study.
Surgical procedure
All patients underwent open hepatectomy under general anesthesia,performed by experienced hepatobiliary surgeons.The type and extent of hepatectomy were determined based on liver function and remnant liver volume as well as on the location,size,and number of tumors.The surgical approach was either a right or bilateral subcostal incision,with or without midline extension.The Pringle maneuver was performed intermittently or continuously to minimize the blood loss.The liver parenchyma was transected using an ultrasonic dissector or Cavitron ultrasonic surgical aspirator.The intrahepatic bile ducts were identified and ligated using clips or sutures.The cut surface of the liver was treated with fibrin glue or an argon beam coagulator to prevent bile leakage and bleeding.A closed suction drain was placed near the cut surface of the liver before closing the abdomen.
Postoperative management
All patients were transferred to the intensive care unit after surgery and closely monitored for vital signs,fluid balance,hemoglobin levels,liver function,coagulation profile,and drain output.The drain fluid was routinely checked for bilirubin levels on postoperative day three.Bile leak was diagnosed when the bilirubin level in the drain fluid was three times higher than the serum level.The management of bile leakage was based on the ISGLS classification and clinical condition of the patient.Grade A bile leaks were managed using conservative measures such as drainage,antibiotics,and nutritional support.Grade B bile leaks were managed using endoscopic or percutaneous interventions such as endoscopic retrograde cholangiopancreatography (ERCP) with stenting or percutaneous transhepatic cholangiography (PTC) with drainage.Grade C bile leaks were managed using laparotomy and surgical repair.
Data collection and analysis
The following data were collected from the medical records: demographic characteristics,preoperative liver function test results,tumor characteristics,type and extent of hepatectomy,operative time,blood loss and transfusion,postoperative complications,length of hospital stay,and mortality.The primary outcome measure was bile leakage after open hepatectomy for biliary tract cancer.Secondary outcomes were risk factors,management,and bile leak outcomes.Data were analyzed using SPSS software (version 25.0;IBM Corp.,Armonk,NY,United States).Continuous variables are expressed as mean ± SD or median (range),and categorical variables are expressed as number (percentage).Univariate analysis was performed using Student’st-test or the Mann-WhitneyUtest for continuous variables and the chi-squared test or Fisher’s exact test for categorical variables.Multivariate logistic regression analysis was performed to identify independent risk factors for bile leakage.Statistical significance was set atP< 0.05.
RESULTS
Patient characteristics and operative details
This study included 120 patients who underwent open hepatectomies for biliary tract cancer from February 2018 to February 2023.Baseline characteristics and operative details of the patients are shown in Table 1.The mean age was 62.3 ± 10.4 years,and 68 (56.7%) patients were male.The most common tumor type was intrahepatic cholangiocarcinoma (n=54,45%),followed by gallbladder cancer (n=36,30%) and extrahepatic cholangiocarcinoma (n=30,25%).The most common type of hepatectomy was right hemihepatectomy (n=48,40%),followed by left hemihepatectomy (n=24,20%),and segmentectomy (n=18,15%).The mean operative time was 312.5 ± 87.6 min,and the mean blood loss was 712.5 ± 345.6 mL.Blood transfusions were required in 36 patients (30%).
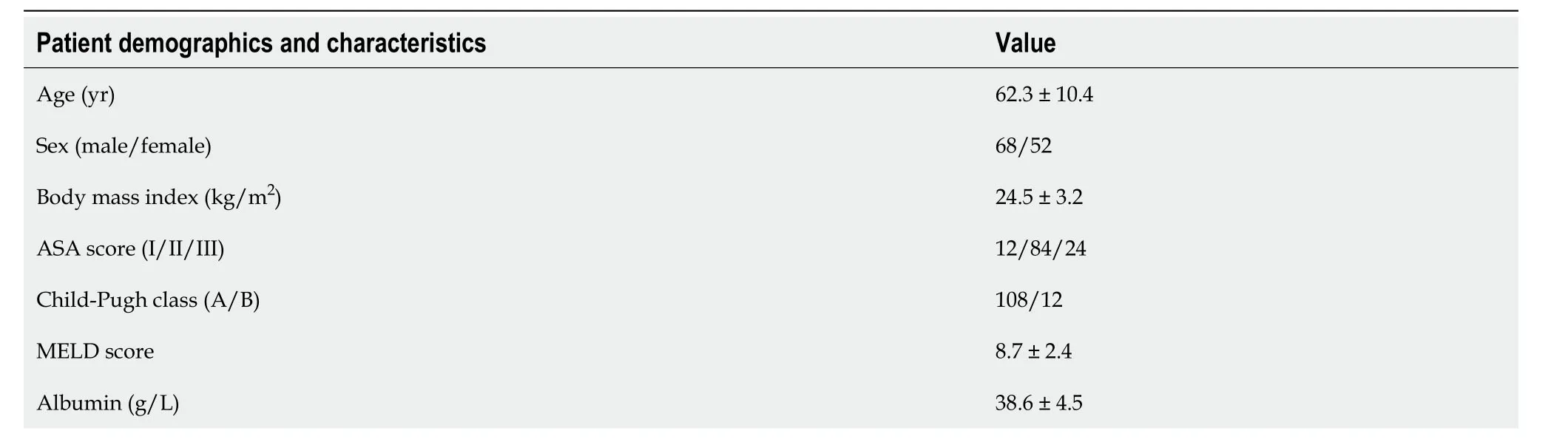
Table 1 Patient characteristics and operative details
Postoperative complications and outcomes
Postoperative complications and patient outcomes are shown in Table 2.The overall morbidity rate was 38.3% (46/120) and the most common complications were bile leakage (16.7%,20/120),wound infections (10%,12/120),and ascites (8.3%,10/120).The median length of hospital stay was 12 d (range,7-35 d).The mortality rate was 1.7% (2/120);both deaths were due to liver failure.

Table 2 Postoperative complications and outcomes,n (%)
Incidence and characteristics of bile leak
Of the 120 patients,20 (16.7%) developed bile leak after open hepatectomy for biliary tract cancer.Patient characteristics are shown in Table 3.The median time of bile leak onset was 5 d (range,1-14 d),and the median duration was 7 d (range,2-28 d).According to the ISGLS classification,most bile leaks were grade A (75%,15/20),followed by grades B (20%,4/20) and C (5%,1/20).The most common location of bile leakage was the cut surface of the liver (70%,14/20),followed by the anastomosis site (25%,5/20) and the cystic duct stump (5%,1/20).

Table 3 Characteristics of bile leak
Management and outcomes of bile leak
The management and outcomes of patients with bile leakage are presented in Table 4.Most bile leaks (85%,17/20) were treated conservatively with drainage,antibiotics,and nutritional support.Four patients (20%) required endoscopic or percutaneous interventions such as ERCP with stenting (n=2) or PTC with drainage (n=2).One patient (5%) required relaparotomy and surgical repair because of a grade C bile leak with biliary peritonitis.The outcomes of bile leak management were favorable in most cases,with resolution in 18 patients (90%).Two patients (10%) experienced persistent bile leakage and required long-term drainage.
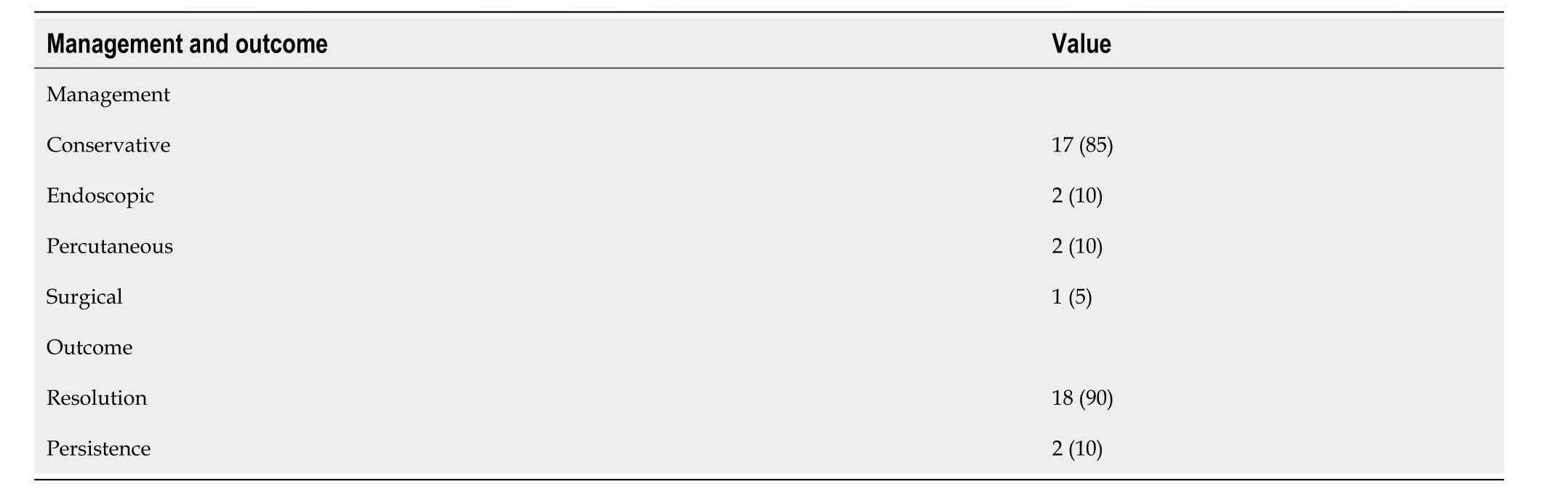
Table 4 Management and outcomes of bile leak,n (%)
Risk factors for bile leak
Univariate and multivariate analyses of risk factors for bile leakage are shown in Table 5.The univariate analysis revealed that male sex,hepatocellular carcinoma,major hepatectomy,blood loss,and blood transfusion were significantly associated with bile leakage.Multivariate analysis confirmed that these factors were independent risk factors,with odds ratios of 2.6,3.1,4.2,2.7,and 3.4,respectively.
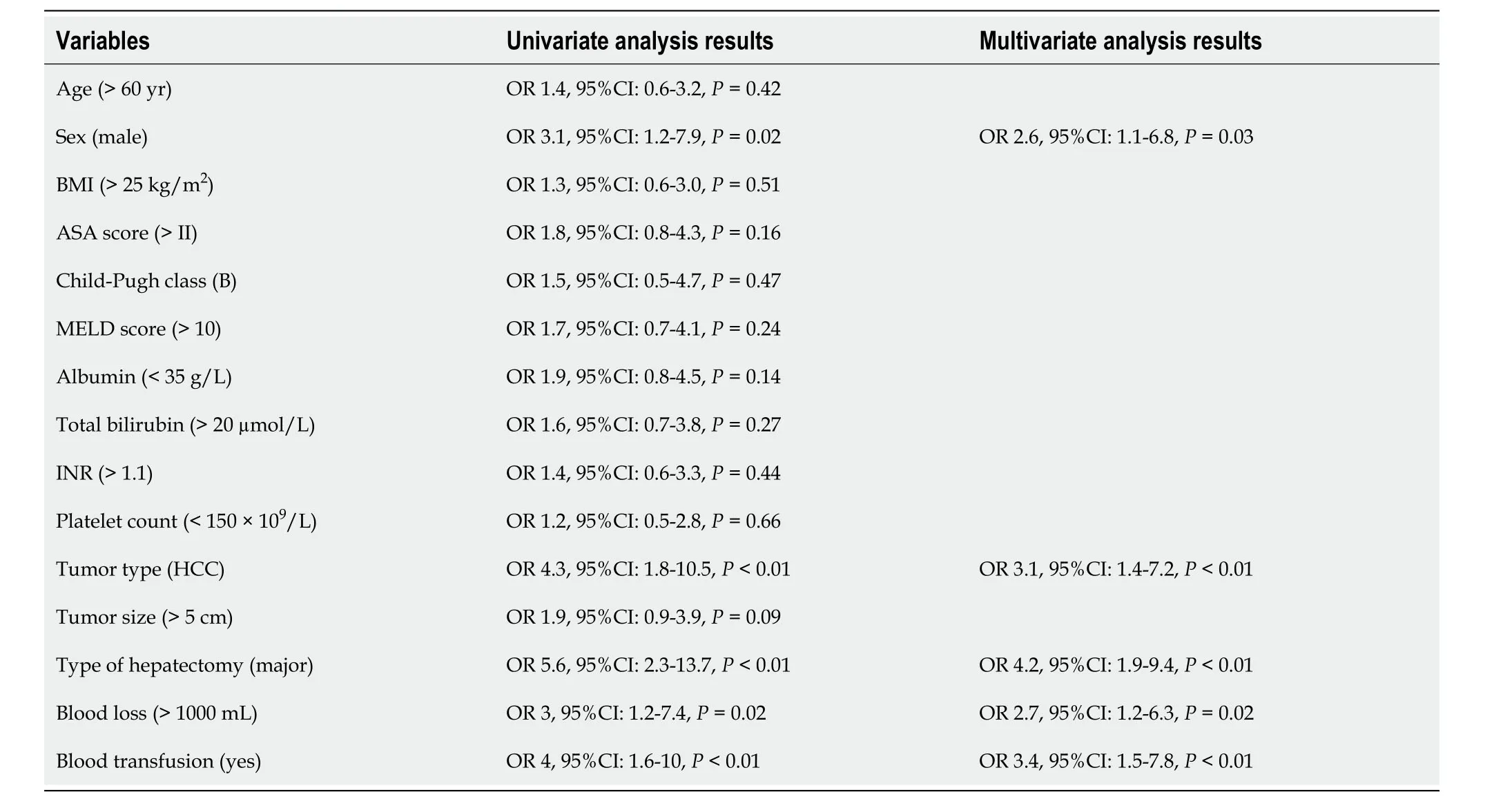
Table 5 Risk factors for bile leak
DlSCUSSlON
This study evaluated the effect of open hepatectomy on postoperative bile leakage in patients with biliary tract cancer and found that the incidence of bile leakage was 16.7%.This value is consistent with previous reports[10].Most bile leaks were mild and could be managed conservatively,while some required endoscopic or percutaneous interventions,and only one required laparotomy and surgical repair.
The risk factors for bile leakage are male sex,hepatocellular carcinoma,major hepatectomy,blood loss,and blood transfusion[15].Bile leakage is a common and serious complication of hepatectomy for biliary tract cancer and can cause significant morbidity and mortality[8].The pathogenesis of bile leak is multifactorial and involves technical,anatomical,physiological,and pathological factors[10].Technical factors include the surgical technique,extent of resection,type of anastomosis,and use of drainage[16,17].Anatomical factors include variations in the bile ducts,the presence of accessory ducts or ducts of Luschka,and tumor location[18].Physiological factors include biliary pressure,liver function,and coagulation status[19,20].Pathological factors include the type and stage of the tumor,presence of inflammation or fibrosis,and response to chemotherapy or radiotherapy[5].Bile leakage is diagnosed based on clinical signs and symptoms,biochemical tests,imaging studies,and endoscopic or percutaneous interventions[21].
The most common symptom of bile leakage is abdominal pain accompanied by fever,jaundice,or ascites[22].Biochemical tests measure the bilirubin level in the drain or peritoneal fluid and are considered diagnostic if the bilirubin is three times higher than the serum bilirubin level.Imaging studies include ultrasonography,computed tomography,magnetic resonance cholangiopancreatography,and hepatobiliary iminodiacetic acid scans,which reveal the presence and location of bile leaks or biloma[23].Endoscopic or percutaneous interventions include ERCP or PTC,which can not only confirm the diagnosis but also provide therapeutic options such as stenting or drainage[9,20].
The treatment of bile leakage depends on its severity,timing,location,and source of the bile leak.The ISGLS classification provides a useful guide for the management of bile leaks based on the clinical impact and the need for therapeutic interventions[6].In general,grade A bile leaks can be managed conservatively with drainage,antibiotics,and nutritional support,whereas grade B and C bile leaks may require endoscopic or percutaneous interventions or even laparotomy and surgical repair[24].Endoscopic interventions include ERCP with stenting or sphincterotomy,which canreduce biliary pressure and divert bile flow to the duodenum,thereby facilitating bile leak healing[25].Percutaneous interventions include the drainage or embolization of PTCs,which can decompress the biliary system and occlude the leaking duct.Surgical interventions,including suture repair,omental patches,and hepaticojejunostomy,can restore biliary continuity and prevent further leakage[26].
The management of bile leaks should be individualized according to the patient’s condition,availability of expertise and resources,and the potential risks and benefits of each intervention.The goal of treatment is to resolve bile leaks with minimal morbidity and mortality.
Despite the valuable insights provided by this study,we acknowledge several limitations.First,the retrospective nature of the study may have introduced selection and information bias.Patients were selected based on specific inclusion criteria,and data were collected from medical records,which may not capture all the nuances of clinical presentations and interventions.Second,this study was conducted at a single tertiary referral center,which may limit the generalizability of the findings to other settings or populations.Third,the sample size of 120 patients,while substantial for rare conditions,may still be too small to detect subtle associations or allow for the generalization of results across a broader patient population with biliary tract cancer.Additionally,relevant variables that could influence the incidence of bile leakage,such as the exact surgical technique used or the surgeon’s experience,were not assessed.Lastly,the lack of long-term follow-up data limits the ability to evaluate the impact of bile leakage on long-term outcomes,such as cancer recurrence or long-term survival.Future prospective studies with larger sample sizes and multicenter collaborations are needed to validate our findings and further refine the risk stratification of bile leakage after open hepatectomy for biliary tract cancer.
CONCLUSlON
In conclusion,this study demonstrated that open hepatectomy for biliary tract cancer is associated with a high incidence of bile leakage,which can be challenging.However,most bile leaks are mild and can be managed conservatively,while some require endoscopic or percutaneous interventions and rarely require surgical repair.Male sex,hepatocellular carcinoma,major hepatectomy,blood loss,and blood transfusion are risk factors for bile leakage.Further studies are needed to explore optimal strategies for preventing and treating bile leakage after open hepatectomy for biliary tract cancer.
ARTlCLE HlGHLlGHTS
Research background
Bile leakage is a common and significant complication of open hepatectomy,a surgical procedure performed to treat biliary tract cancer.Bile leaks are characterized by the drainage of bile from the surgical site or drain or the formation of a biloma (a localized collection of bile),as observed on imaging scans.This complication can lead to various adverse outcomes including infection,abscess formation,sepsis,delayed wound healing,and prolonged hospital stay.Therefore,understanding the incidence,risk factors,and management strategies of bile leaks is crucial to improve patient outcomes and reduce the burden on the healthcare system.
Research motivation
Bile leakage is a significant complication of open hepatectomy for the treatment of biliary tract cancer.However,few studies have focused on the incidence,risk factors,and management of these complications.Therefore,this study aimed to address this knowledge gap by conducting a comprehensive analysis of 120 patients who underwent open hepatectomy for biliary tract cancer.The motivation for this study lies in the need to better understand the frequency,associated risk factors,and effective management strategies of bile leaks.By identifying these factors,healthcare professionals can improve patient outcomes,reduce complications,and optimize treatment approaches in patients undergoing open hepatectomy for biliary tract cancer.
Research objectives
Evaluate the incidence of bile leak after open hepatectomy for biliary tract cancer.Identify the risk factors associated with bile leakage in this patient population.Investigate the management strategies employed for bile leaks,including conservative approaches and interventional procedures.Assess the severity,timing,location,and duration of bile leaks following open hepatectomy.Determine the association between specific risk factors,such as male sex,hepatocellular carcinoma,major hepatectomy,blood loss,and blood transfusion,and the occurrence of bile leaks.By achieving these objectives,the study aimed to provide valuable insights into the incidence,risk factors,and management of bile leak complications after open hepatectomy for biliary tract cancer,ultimately contributing to improved patient care and surgical outcomes.
Research methods
Study population: Patient data from open hepatectomy for biliary tract cancer (February 2018 to February 2023) were retrospectively analyzed.Data Collection: Information on bile leak complications (incidence,severity,timing,location,and treatment) was obtained from patient records and charts.Bile Leak Definition: Defined as bile drainage or presence of biloma observed on imaging.Statistical Analysis: Univariate and multivariate logistic regression analyses were used to assess the risk factors (sex,hepatocellular carcinoma,major hepatectomy,blood loss,and transfusion).Utilizing existing data allows for cost-effective investigations,while statistical analyses enhance understanding.These findings provide insights into bile leak management and may improve the care of patients undergoing open hepatectomy.
Research results
Bile leak occurred in 16.7% (20/120) of patients who underwent open hepatectomy for biliary tract cancer.Most cases were grade A,with a median onset time of 5 d and duration of 7 d.The cut surface of the liver was the most common site of leakage (70%).Conservative treatment was successful in 85% of cases,while 10% required endoscopic retrograde cholangiopancreatography (ERCP) with stenting and 5% required percutaneous transhepatic cholangiography (PTC) with drainage.Male sex,hepatocellular carcinoma,major hepatectomy,blood loss,and blood transfusion were identified as risk factors for bile leak.
Research conclusions
This study provides new insights into the incidence,risk factors,and management of bile leak after open hepatectomy for biliary tract cancer.It highlights that bile leakage is a common complication,with an incidence rate of 16.7%.This study identified male sex,hepatocellular carcinoma,major hepatectomy,blood loss,and blood transfusion as significant risk factors for bile leakage.This suggests that conservative management,including drainage,antibiotics,and nutritional support,is effective in most cases.The study also mentioned the use of ERCP with stenting or PTC with drainage as alternative treatment options.
Research perspectives
Future studies should focus on developing strategies to reduce the incidence of bile leakage after open hepatectomy for biliary tract cancer.Investigating the use of advanced imaging techniques for early detection and assessment of bile leaks could improve patient outcomes.Additionally,the potential of minimally invasive surgical techniques and perioperative interventions to reduce the risk of bile leakage warrants further investigation.Long-term follow-up studies are needed to evaluate the effects of bile leak on patient survival and quality of life.Collaborative efforts are necessary to establish standardized guidelines and protocols for the prevention,diagnosis,and management of bile leakage in clinical practice.
FOOTNOTES
Author contributions:Wu G and Sun C proposed the concept of this study;Li WY contributed to data collection;Wu G and Gong YX drafted the first draft;Lin F contributed to the formal analysis of this study;Sun C conducted guidance research,methodology,and visualization;all authors participated in the study,validated the study,and jointly reviewed and edited the manuscript.
lnstitutional review board statement:This study has been approved by the Clinical Research Project Ethics Review of the Medical Ethics Committee of the Second Affiliated Hospital of Harbin Medical University,with the Ethics Review Approval Document (No.KY2023-111).
lnformed consent statement:All study participants or their legal guardians provided written informed consent before study enrollment.
Conflict-of-interest statement:All authors declare that there are no conflicts of interest.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Gang Wu 0009-0009-7388-1025;Chen Sun 0009-0002-6472-9709.
S-Editor:Gong ZM
L-Editor:A
P-Editor:Yu HG
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Prospects in the application of ultrasensitive chromosomal aneuploidy detection in precancerous lesions of gastric cancer
- Prognostic value of ultrasound in early arterial complications post liver transplant
- Added value of ratio of cross diameters of the appendix in ultrasound diagnosis of acute appendicitis
- Single-incision laparoscopic transabdominal preperitoneal repair in the treatment of adult female patients with inguinal hernia
- Predictive value of machine learning models for lymph node metastasis in gastric cancer: A two-center study
- Micro-power negative pressure wound technique reduces risk of incision infection following loop ileostomy closure