Single-incision laparoscopic transabdominal preperitoneal repair in the treatment of adult female patients with inguinal hernia
2024-03-07XiaoJunZhuJingYiJiaoHuiMinXuePengChenChangFuQinPengWang
Xiao-Jun Zhu,Jing-Yi Jiao,Hui-Min Xue,Peng Chen,Chang-Fu Qin,Peng Wang
Abstract BACKGROUND Women have a 3% lifetime chance of developing an inguinal hernia,which is not as common in men.Due to its cosmetic benefits,single-incision laparoscopic transabdominal preperitoneal (SIL-TAPP) inguinal hernia repair is becoming increasingly popular in the management of inguinal hernia in women.However,there are no studies comparing the safety and applicability of SIL-TAPP repair with conventional laparoscopic transabdominal preperitoneal (CL-TAPP) inguinal hernia repair for the treatment of inguinal hernia in women.AIM To compare the outcomes of SIL-TAPP and CL-TAPP repair in adult female patients with inguinal hernia and to estimate the safety and applicability of SILTAPP repair in adult female inguinal hernia patients.METHODS We retrospectively compared the clinical information and follow-up data of female inguinal hernia patients who underwent SIL-TAPP inguinal hernia repair and those who underwent CL-TAPP inguinal hernia repair at the Affiliated Hospital of Nantong University from February 2018 to December 2020 and assessed the long-term and short-term outcomes of both cohorts.RESULTS This study included 123 patients,with 71 undergoing SIL-TAPP repair and 52 undergoing CL-TAPP repair.The two cohorts of patients and inguinal hernia characteristics were similar,with no statistically meaningful difference.The rate of intraoperative inferior epigastric vessel injury was lower in patients in the SIL-TAPP cohort (0,0%) than in patients in the CL-TAPP cohort (4,7.7%) and was significantly different (P < 0.05).In addition,the median [interquartile range (IQR)] total hospitalization costs were significantly lower in patients in the SIL-TAPP cohort [$3287 (3218-3325)] than in patients in the CLTAPP cohort [$3511 (3491-3599)].Postoperatively,the occurrence rate of trocar site hernia was lower in the SILTAPP cohort (0,0%) than in the CL-TAPP cohort (4,7.7%),and the median (IQR) cosmetic score was significantly higher in the SIL-TAPP cohort [10 (10-10)] than in the CL-TAPP cohort [9 (9-10)].CONCLUSION SIL-TAPP repair did not increase the incidence of intraoperative and postoperative complications in female inguinal hernia patients.Moreover,female inguinal hernia patients who underwent SIL-TAPP repair had a lower probability of trocar site hernia and inferior epigastric vessel injury than female inguinal hernia patients who underwent CL-TAPP repair.In addition,female inguinal hernia patients who underwent SIL-TAPP repair reported a more aesthetically pleasing postoperative abdominal incision.Therefore,SIL-TAPP repair is a better option for the treatment of inguinal hernias in women.
Key Words: Single-incision;Groin hernia;Female;Inguinal hernia;Laparoscopic transabdominal preperitoneal inguinal hernia repair
lNTRODUCTlON
An inguinal hernia (also called a groin hernia) is an extra-abdominal hernia formed when an intra-abdominal organ protrudes towards the body surface through a congenital or acquired defect in the groin region.The cause of inguinal hernia is mainly weakness of the muscles and tissues in the inguinal region.Causes of inguinal hernias include persistent coughing,smoking,being overweight,and straining while urinating or defecating[1].Inguinal hernia is not common in men,and women have a 3 percent chance of developing an inguinal hernia in their lifetime[2].In addition,femoral hernias occur most often in women and most often require surgery.
An inguinal hernia will not improve on its own,and surgery is often needed when a patient develops symptoms of a groin hernia[3].Tension-free groin hernia repair is now the primary option for groin hernia treatment[4].Tension-free groin hernia repair includes open groin hernia repair surgery and laparoscopic groin hernia repair surgery.Compared to open groin hernia repair,laparoscopic groin hernia repair is more minimally invasive,and patients experience less postoperative abdominal incision pain and a shorter time to return to normal life[5-8].Laparoscopic groin hernia repair allows for the use of the posterior approach,which is of particular significance.Using the posterior approach has one benefit: it allows for accurate identification of the groin hernia and the placement of a larger and more stable mesh[9].As a result,laparoscopic groin hernia repair has become the primary method of treatment for groin hernia over open surgery.To ensure minimal invasiveness,single-incision laparoscopic groin hernia repair is gradually being applied for the treatment of clinical groin hernia patients.Single-incision laparoscopic groin hernia repair further reduces pain,and the abdominal incision is more aesthetically pleasing after single-incision laparoscopic groin hernia surgery compared to conventional laparoscopic surgery,so it is preferred by many patients,especially female patients with aesthetic concerns.
However,there is a lack of comparative studies between single-port laparoscopic groin hernia repair and conventional laparoscopic groin hernia repair to investigate the safety and applicability of single-incision laparoscopic groin hernia repair in adult female patients with groin hernia.Therefore,we conducted a single-centre retrospective study to evaluate the safety and applicability of single-incision laparoscopic transabdominal preperitoneal (SIL-TAPP) repair in female patients by comparing the clinical data of female patients who underwent SIL-TAPP and conventional laparoscopic transabdominal preperitoneal (CL-TAPP) repair and by analysing the long-term and short-term outcomes of both cohorts.
MATERlALS AND METHODS
Research design and patients
Our study retrospectively explored a dataset between February 2018 and December 2020 in the hernia follow-up system.The dataset consisted of prospectively recorded data of 165 female groin hernia patients who underwent SIL-TAPP or CLTAPP repair at the General Surgery Department of the Affiliated Hospital of Nantong University.These following factors could prevent participation: (1) Being under 18 years old;(2) having an acute and incarcerated inguinal hernia;and (3) having hernia repair combined with other surgeries.Ultimately,140 patients (81 patients in the SIL-TAPP cohort and 59 patients in the CL-TAPP cohort) were eligible for the study.During follow-up,17 patients (10 patients in the SIL-TAPP cohort and 7 patients in the CL-TAPP cohort) were lost to follow-up.We ultimately collected data from 123 patients,comprising 71 patients in the SIL-TAPP cohort and 52 patients in the CL-TAPP cohort (Figure 1).The study was conducted with the informed consent of all the patients.All procedures in this study were performed by the same surgeon.

Figure 1 Flow chart for patient selection and study.SIL-TAPP: Single-incision laparoscopic transabdominal preperitoneal inguinal hernioplasty;CL-TAPP: Conventional laparoscopic transabdominal preperitoneal inguinal hernioplasty;SILS-TAPP: Single-incision laparoscopic transabdominal preperitoneal inguinal hernioplasty.
Surgical techniques
After routine disinfection of the abdomen and groin with a towel,we disinfected the navel 2-3 times with an alcohol cotton ball.In SIL-TAPP repair,we generally made a longitudinal incision of approximately 2 cm in the umbilicus and placed one 10 mm trocar and two 5 mm trocars (Figure 2A),and in CL-TAPP repair,one 10-mm trocar was placed at the umbilical opening and one 5-mm trocar was placed on each side of the umbilicus (Figure 2B and C).With the hernia site rotated upwards,the patient was positioned in the reverse Trendelenburg position.The surgical incision was made from the inner umbilical crease to the anterior superior iliac spine at a distance of 2-3 cm from the top of the internal ring aperture (Figure 3A).Then,the preperitoneal space was accessed by separating the top and bottom edges of the peritoneal flap.The lateral edge of the hernia sac was dissected to the midpoint of the iliopsoas muscle and further to the Bogros space.Starting at the middle of the inferior epigastric vessel,the transversalis fascia and the bladder were dissected to gain access to the Retzius space.The exposure was widened to the pubic symphysis from the pectineal ligament,extending medially through the median line and out to the inner edge of the hernia sac.The hernia sac was then divided (Figure 3B).The hernia sac was completely removed to the apex after separation,if possible.If the hernia sac was extensive and adherent to the adjacent tissue,it was incised,and the distal tip was opened.The round ligament of the uterus was usually preserved.The hernia sac was dissected towards the midline,and both sides of the bilateral hernia were joined.A 10 cm × 15 cm mesh was selected for implantation in the preperitoneal cavity to overlie the separation area described above (Figure 3C).For direct hernias and indirect hernias with sac diameters greater than 4 cm,we usually fix the mesh with a staple gun after placement,while the mesh is not usually fixed for other types of inguinal hernias.We recommend the use of 4-0 V-lock sutures for continuous suturing of the peritoneum,laterally to medially with no knots (Figure 3D).After completion of the suture,the suture was cut without leaving a residual end to avoid bowel injury and obstruction.If there was high peritoneal tension,the remaining end of the suture was clamped with titanium clamps.Finally,all trocars were removed,and the abdominal incisions were closed.For the midline longitudinal incision of the umbilicus,the suture was usually divided into two layers.First,the umbilical fascia layer was sutured continuously with 1-0 v-lock sutures,and then the midpoint of the standing flap at the umbilical ring was sutured with an absorbable protein line.Both ends were sutured intradermally,and the rest were sutured intermittently.After blood was cleaned with gauze,the standing flap was pushed back to the umbilical fossa to achieve a perfect repair.
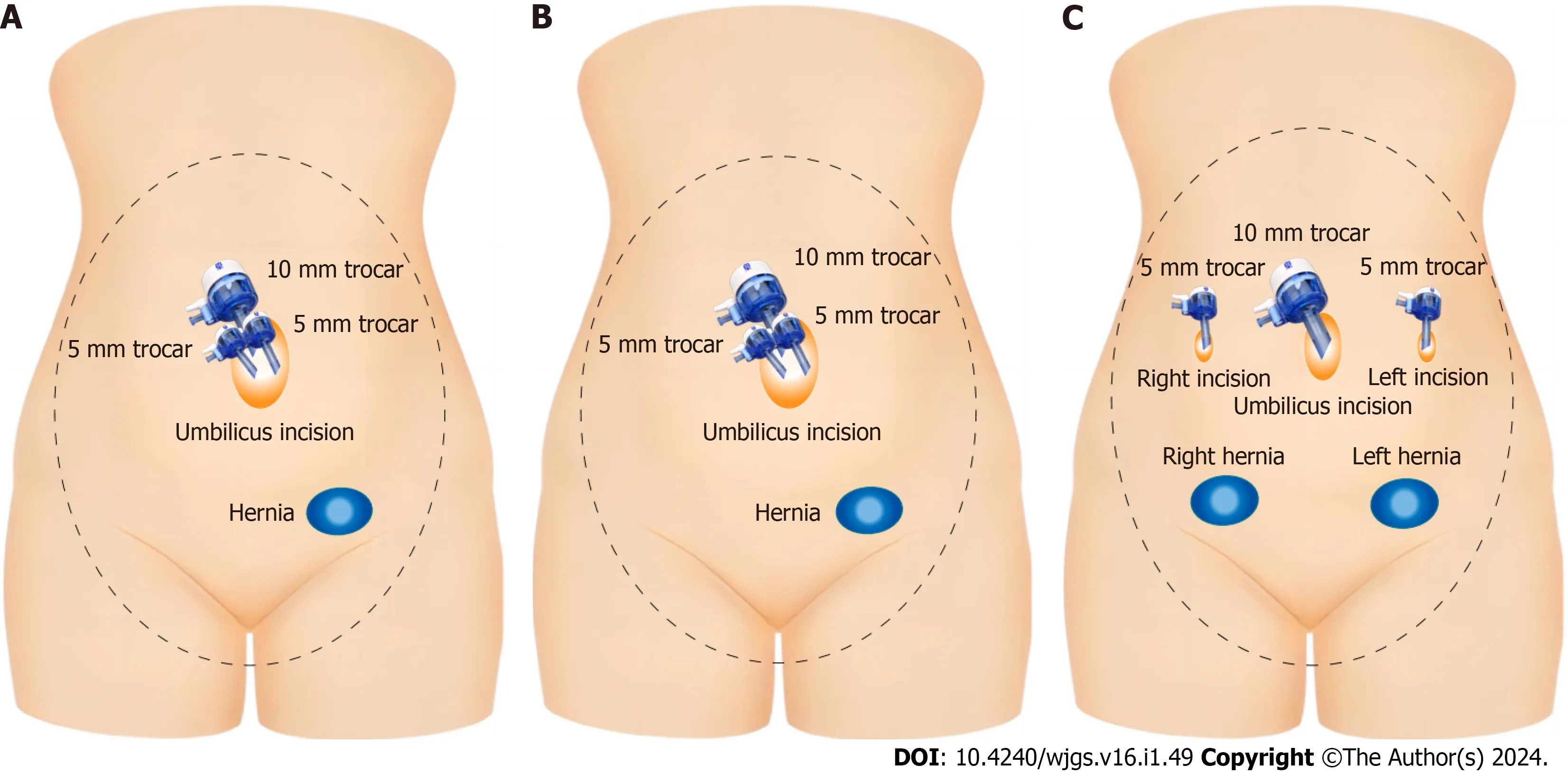
Figure 2 Schematic of trocar placement. A: Trocar placement in single-incision laparoscopic transabdominal preperitoneal inguinal hernioplasty repair;B: Trocar placement in unilateral Conventional laparoscopic transabdominal preperitoneal inguinal hernioplasty (CL-TAPP) repair;C: Trocar placement in bilateral CLTAPP repair.
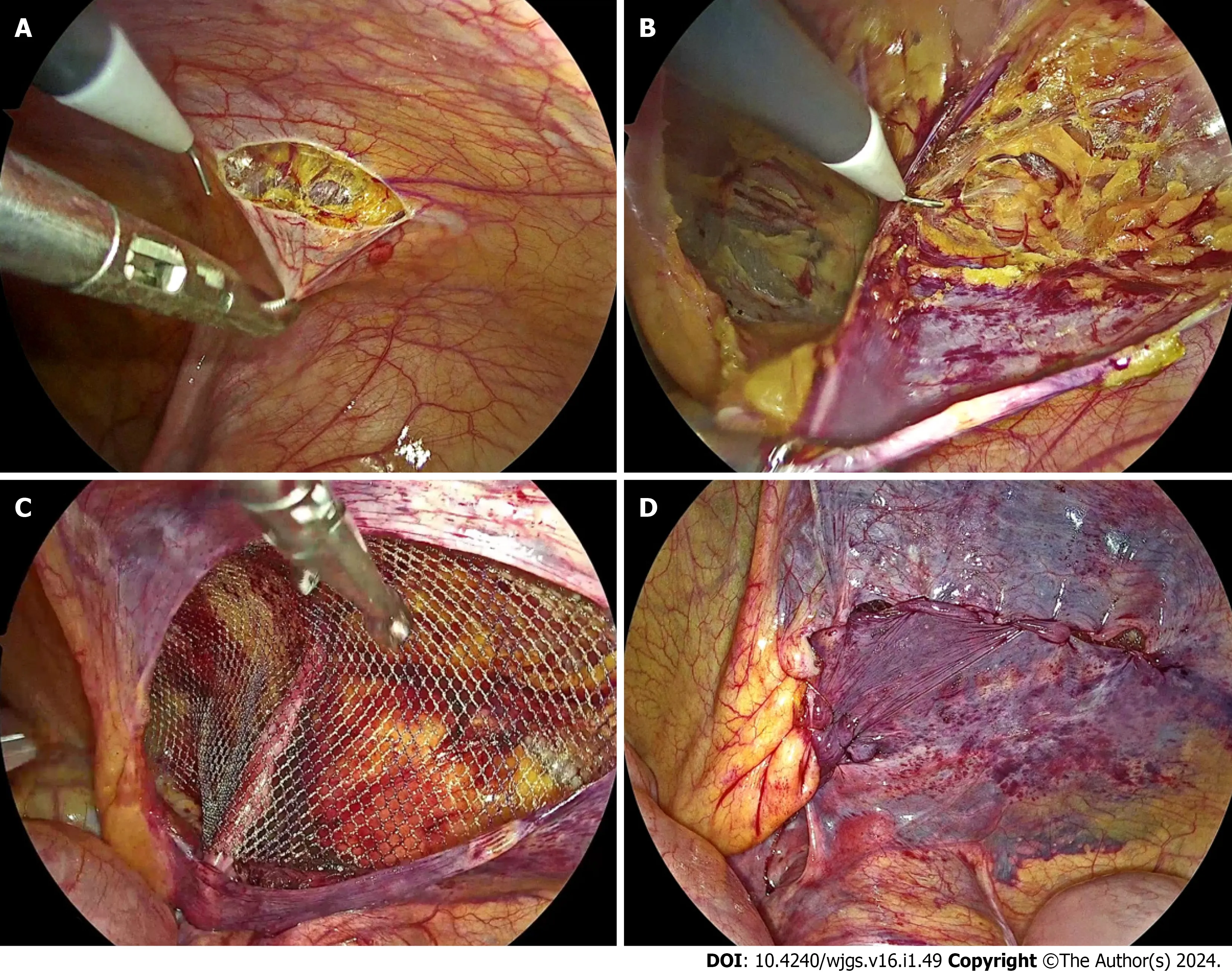
Figure 3 Photographs of some surgical details. A: At the level of 2-3 cm along the upper margin of the inner ring opening,the peritoneum was cut from the medial umbilical fold to the anterior superior iliac spine;B: The hernia sac was disposed of;C: The mesh was placed and unfolded fully;D: The peritoneum was sutured continuously.
Follow up
All patients underwent a physical examination in the outpatient clinic at 1 wk and 1 mo postoperatively to determine whether they had recovered well or whether short-term complications including seroma,haematoma,etc.,had occurred.In addition,patients returned to the hospital every 6 mo for physical examination and CT to determine whether there were long-term complications,such as trocar hernia and recurrence,had occurred.Patients were followed up by telephone to rate the cosmesis of the postoperative abdominal incision.
Statistical analysis
All statistical procedures were conducted using SPSS version 26 (IBM).We express distributions of continuous variables using the median and interquartile range (IQR) and tested them using the Mann-WhitneyUtest.We used the chi-squared test to test categorical variables and percentages.Statistical differences were indicated byPvalues less than 0.05.
RESULTS
Between February 2018 and December 2020,a total of 123 patients participated in this study,of whom 71 underwent SILTAPP repair and 52 underwent CL-TAPP repair.The characteristics of the adult female patients in our study and their groin hernias are summarized in Table 1.The median (IQR) age of the patients in the SIL-TAPP cohort and the patients in the CL-TAPP cohort was 46 (41-53) and 47 (42-53) years,respectively,with no meaningful difference (P> 0.05).The median body mass index (IQR) was 22.46 (20.93-22.95) kg/m2and 22.35 (21.76-23.06) kg/m2for patients in the SIL-TAPPand CL-TAPP cohorts,res-pectively,which was also not significantly different (P> 0.05).In addition,hernia characteristics,including the type of hernia and the location and size of the hernia ring,were similar in both cohorts.A history of lower abdominal operation was reported by 8 (11.3%) patients in the SIL-TAPP cohort compared to 9 (17.3%) patients in the CL-TAPP cohort,but there was no difference between the two cohorts.

Table 1 Patients and inguinal hernias characteristics
Table 2 shows the intraoperative and hospitalization periods of the two cohorts of patients.The median (IQR) operative time was 32 (29-35) minutes and 33.5 (30-39.5) minutes for patients in the SIL-TAPP and CL-TAPP cohorts,respectively,with no meaningful difference (P> 0.05).Moreover,there was no meaningful difference between the two cohorts in terms of intraoperative nerve injury,adjacent organ injury,pain in the groin area within 24 h postoperatively or length of hospital stay.However,no patients in the SIL-TAPP cohort had intraoperative inferior epigastric vessel injury,while 4 (7.7%) patients in the CL-TAPP cohort had inferior epigastric vessel injury,with a significant difference between the two cohorts (P< 0.05).All four cases of injury to the inferior epigastric artery occurred at the time of trocar placement on both sides,one on the left and three on the right.In addition,the median (IQR) hospitalization cost of patients in the CL-TAPP cohort was $3511 (3491-3559),which was significantly higher than that of the patients in the SILTAPP cohort [$3287 (3218-3325)],and there was a meaningful difference (P< 0.001).

Table 2 Surgery and hospitalization information
Table 3 demonstrates the postoperative complications as well as cosmetic scores of the two cohorts of patients.Among the patients,trocar site hernia was seen in 4 (7.7%) patients in the CL-TAPP cohort,whereas it was not seen in the patients in the SIL-TAPP cohort,and there was a meaningful difference (P< 0.05).There was no meaningful difference between the two cohorts in terms of postoperative complications such as seroma,patch infection,chronic pain,labia majora oedema,sensory abnormalities in the perineal area,uterine prolapse,fertility abnormalities and recurrence.The cosmetic score was 10 (10-10) for patients in the SIL-TAPP cohort and 9 (9-10) for patients in the CL-TAPP cohort,and the cosmetic score of the patients in the SIL-TAPP cohort was meaningfully better than that of patients in the CL-TAPP cohort (P< 0.001).
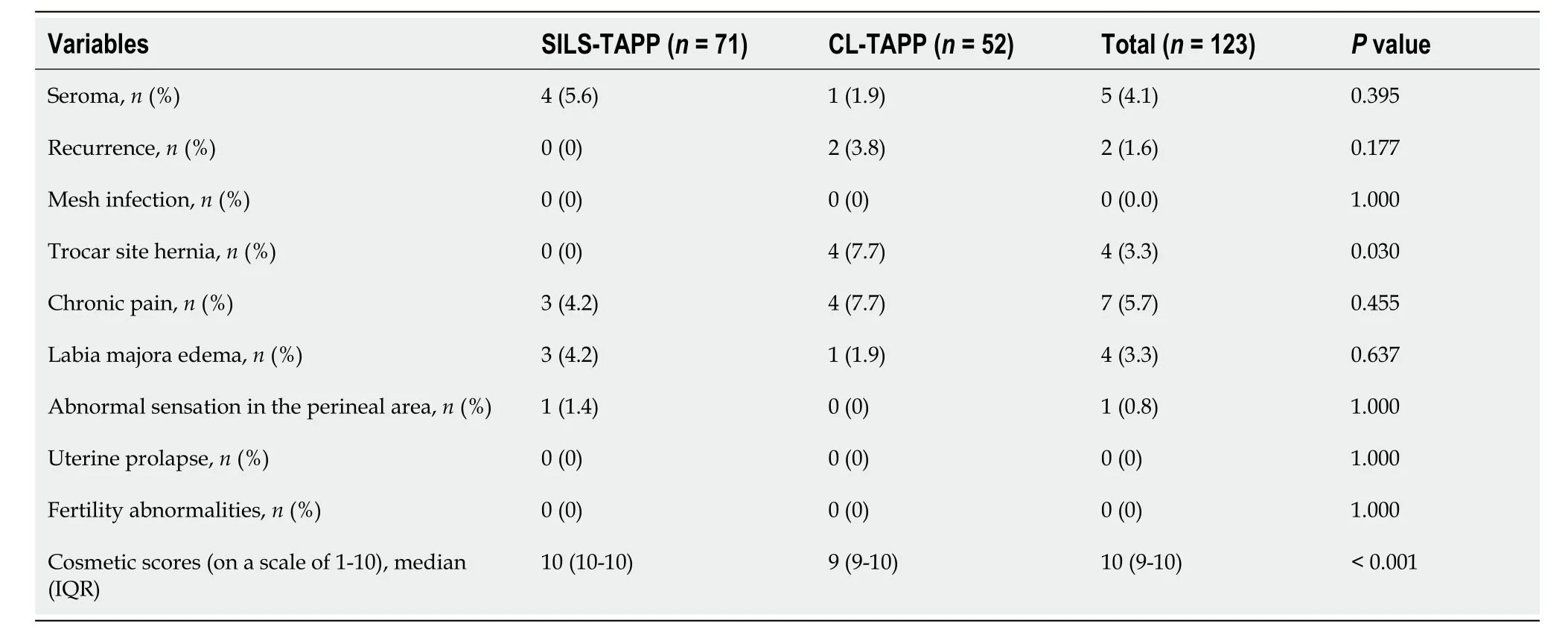
Table 3 Postoperative complications and cosmetic scores
DlSCUSSlON
With the development of modern surgical concepts,doctors and patients are paying increasing attention to quality of life after surgery[10].To reduce the physical pain and psychological burden associated with surgery,surgeries are now becoming more minimally invasive,and this is also true of groin hernia repair surgery[11].Single-incision laparoscopic groin hernia repair results in less surgical trauma and a faster recovery for the patient[12].Previous studies have shown that single-incision laparoscopic groin hernia repair is safe and feasible[13].However,because groin hernias occur more often in male patients,previous reports lack separate studies in female patients.In addition,we know that the outcome of hernia repair in female patients is significantly different from that in male patients[14-16].Therefore,we included all female patients with inguinal hernia as a way to research the safety and applicability of single-incision laparoscopic groin hernia repair in female patients with inguinal hernia.Because of the broader surgical indications for TAPP repair,we chose to compare the results of SIL-TAPP and CL-TAPP repair in female patients[17].
In many studies,the operative time of SIL-TAPP repair was much longer than that of CL-TAPP repair due to the absence of the "chopstick effect" and the "operating triangle" caused by the single incision,as well as the greatly increased difficulty of peritoneal suture under a single incision[18].However,our study,as well as our previous study,showed that after overcoming the learning curve,there was no statistically meaningful difference in the surgery time between the SILTAPP and CL-TAPP cohorts,which did not lead to complications associated with the long operative time[13].
In a retrospective study that included 3100 traditional multiport laparoscopic tension-free groin hernia repairs,the rate of damage to the inferior epigastric vessels was 0.47%[19].The body surface projection of the inferior epigastric vessels is the midpoint of the groin ligament towards the umbilicus,and traditional multiport laparoscopic groin hernia repair carries the potential for damage to the inferior epigastric vessels during puncture of the trocar on both sides.In contrast,SIL-TAPP repair does not require blind puncture of the trocar on both sides of the umbilicus as the operative hole;therefore,our research found that no patients in the SIL-TAPP cohort suffered any injuries to the inferior epigastric vessels during surgery,whereas four patients (7.7%) in the CL-TAPP cohort suffered intraoperative inferior epigastric vessel injuries,and the difference between the two cohorts was statistically significant (P< 0.05).
It is well known that female groin hernia patients are more likely to develop chronic pain after groin hernia repair[16,20],so the occurrence rate of postoperative chronic pain is also an important indicator for evaluating the feasibility of groin hernia repair surgery.In our study,three patients (4.2%) in the SIL-TAPP cohort experienced postoperative chronic pain in the inguinal area,compared with four patients (7.7%) in the CL-TAPP cohort,which shows that the occurrence rate of postoperative chronic pain in the SIL-TAPP cohort was lower than that in the CL-TAPP cohort,suggesting that SIL-TAPP repair is more conducive to improving the postoperative quality of life of female inguinal hernia patients.
Abdominal trocar site hernia often presents as an abdominal incisional mass or bulge,which greatly affects patients’ quality of life and causes a very significant psychological burden,especially in female patients.Previous studies have shown that single-incision laparoscopic surgery carries a higher risk of trocar site hernia in patients than conventional multiport laparoscopic surgery[21].To compare the trocar site hernia incidence between patients in the SIL-TAPP cohort and the CL-TAPP cohort,we followed up the patients in both groups and determined whether they had trocar site hernias by physical examination and CT.Through follow-up,we found that four (7.7%) patients in the CL-TAPP cohort developed trocar site hernias,whereas there were no trocar site hernias in the SIL-TAPP cohort,and the difference between the two cohorts was statistically significant (P< 0.05).Therefore,we conclude that SIL-TAPP repair does not increase the incidence of trocar site hernia in patients but rather decreases it,and this result supports SIL-TAPP repair as a better option for female patients.
As mentioned earlier,the invisibility and cosmetic nature of the incision is also an important indicator improving the postoperative quality of life and reducing the postoperative psychological burden in female patients.Unlike the singleincision laparoscopic groin hernia repair surgery in many previous studies,our SIL-TAPP repair surgery involves a completely transumbilical approach,and the postoperative umbilical incision is completely hidden in the umbilical fossa folds,making the surgical incision completely invisible to the patient after recovery.The results indicated that patients in the SIL-TAPP cohort had a cosmetic score of 10 (10-10),and those in the CL-TAPP cohort had score of 9 (9-10),and patients in the SIL-TAPP cohort had a significantly higher cosmetic score than patients in the CL-TAPP cohort (P< 0.001).Concealed incisions resulted in higher confidence and a higher postoperative quality of life in female patients.
However,our research has several limitations.First,this study retrospectively compared patients who underwent SILTAPP and CL-TAPP repair.In addition,our sample size was not large enough.Therefore,further studies are needed to validate our ideas.
CONCLUSlON
Our findings suggest that female inguinal hernia patients who underwent SIL-TAPP repair had a lower probability of trocar site hernia and inferior epigastric vessel injury than those who underwent CL-TAPP repair.Furthermore,patients who underwent SIL-TAPP repair reported a more cosmetically pleasing postoperative abdominal incision,making SILTAPP repair a better option for female inguinal hernia patients.
ARTlCLE HlGHLlGHTS
Research background
Single-incision laparoscopic transabdominal preperitoneal (SIL-TAPP) inguinal hernia repair is becoming increasingly popular for the treatment of inguinal hernia in women due to its cosmetic benefits.However,there is no comparative study of SIL-TAPPvsconventional laparoscopic transabdominal preperitoneal (CL-TAPP) inguinal hernia repair to illustrate the safety and applicability of SIL-TAPP repair in the treatment of inguinal hernia in female patients.Therefore,a comparative study of SIL-TAPP and CL-TAPP repair in the treatment of inguinal hernia in women is urgently needed and important.
Research motivation
The aim was to compare intraoperative conditions,postoperative complication rates and cosmetic outcome scores of SILTAPPvsCL-TAPP repair in the treatment of inguinal hernia in women.
Research objectives
The safety and applicability of SIL-TAPP repair in the treatment of inguinal hernia in women was analysed by comparing the intraoperative and postoperative data of SIL-TAPP repair and CL-TAPP repair in the treatment of inguinal hernia in women.
Research methods
We ultimately obtained clinical data for a total of 123 patients (71 who underwent SIL-TAPP repair and 52 who underwent CL-TAPP repair) who participated in this study between February 2018 and December 2020.The safety and applicability of SIL-TAPP repair in the treatment of female inguinal hernia patients was analysed by comparing the hernia characteristics,intraoperative conditions,postoperative complication rates and postoperative cosmetic scores between the two groups.
Research results
SIL-TAPP repair did not increase the incidence of intraoperative and postoperative complications in female inguinal hernia patients.Moreover,female inguinal hernia patients who underwent SIL-TAPP repair had a lower probability of trocar site hernia and inferior epigastric vessel injury than female inguinal hernia patients who underwent CL-TAPP repair.In addition,female inguinal hernia patients who underwent SIL-TAPP repair reported a more aesthetically pleasing postoperative abdominal incision.
Research conclusions
SIL-TAPP repair is safe and feasible for the treatment of female inguinal hernia patients and will be a preferred option for female inguinal hernia patients.
Research perspectives
In the future,multicentre studies with larger samples are needed to analyse the safety and applicability of SIL-TAPP repair.
FOOTNOTES
Co-first authors:Xiao-Jun Zhu and Jing-Yi Jiao.
Co-corresponding authors:Chang-Fu Qin and Peng Wang.
Author contributions:Zhu XJ,Jiao JY,Xue HM,Qin CF and Wang P conceived,designed and refined the study protocol;Zhu XJ,Jiao JY and Chen P were involved in the data collection;Zhu XJ,Jiao JY,Qin CF and Wang P analyzed the data;Zhu XJ and Jiao JY drafted the manuscript;All authors were involved in the critical review of the results and have contributed to,read,and approved the final manuscript.Zhu XJ and Jiao JY contributed equally to this work as co-first authors.Qin CF and Wang P contributed equally to this work as co-corresponding authors.The reasons for designating Zhu XJ and Jiao JY as co-first authors/ Qin CF and Wang P as cocorresponding authors are threefold.First,the research was performed as a collaborative effort,and the designation of co-first and cocorresponding authorship accurately reflects the distribution of responsibilities and burdens associated with the time and effort required to complete the study and the resultant paper.This also ensures effective communication and management of post-submission matters,ultimately enhancing the paper's quality and reliability.Second,the overall research team encompassed authors with a variety of expertise and skills from different fields,and the designation of co-first and co-corresponding authors best reflects this diversity.This also promotes the most comprehensive and in-depth examination of the research topic,ultimately enriching readers' understanding by offering various expert perspectives.Third,the choice of these researchers as co-first and co-corresponding authors acknowledges and respects this equal contribution,while recognizing the spirit of teamwork and collaboration of this study.In summary,we believe that designating Zhu XJ and Jiao JY as co-first authors/Qin CF and Wang P as co-corresponding authors of is fitting for our manuscript as it accurately reflects our team's collaborative spirit,equal contributions,and diversity.
Supported byWu Jieping Medical Foundation,No.320.6750.18396;Nantong “14th Five-Year” Science and Education to Strengthen Health Project,General Surgery Medical Key Discipline,No.42;and Nantong Municipal Commission of Health and Family Planning,No.MS2022005.
lnstitutional review board statement:The study was reviewed and approved by the Affiliated Hospital of Nantong University Institutional Review Board (Approval No.2023-K117-01).
lnformed consent statement:All study participants,or their legal guardian,provided informed written consent prior to study enrollment.
Conflict-of-interest statement:The authors declare that they have no conflicts of interest.
Data sharing statement:The datasets generated during and/or analysed during the current study are available from the corresponding author upon reasonable request.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Xiao-Jun Zhu 0000-0001-5265-6800;Jing-Yi Jiao 0000-0002-9560-4725;Hui-Min Xue 0009-0006-6012-1674;Peng Chen 0009-0009-9711-4613;Chang-Fu Qin 0000-0002-3272-8595;Peng Wang 0000-0003-3735-1229.
S-Editor:Lin C
L-Editor:A
P-Editor:Xu ZH
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Sarcopenia in cirrhotic patients: Does frailty matter while waiting for a liver transplant?
- Novel prognostic factors after radical resection of hepatocellular carcinoma: Updating an old issue
- Paravertebral block's effect on analgesia and inflammation in advanced gastric cancer patients undergoing transarterial chemoembolization and microwave ablation
- Predictive factors and model validation of post-colon polyp surgery Helicobacter pylori infection
- Practical effect of different teaching modes in teaching gastrointestinal surgery nursing
- Predictive value of NLR,Fib4,and APRl in the occurrence of liver failure after hepatectomy in patients with hepatocellular carcinoma