Added value of ratio of cross diameters of the appendix in ultrasound diagnosis of acute appendicitis
2024-03-07FengWaGuSiZeWu
Feng-Wa Gu,Si-Ze Wu
Abstract BACKGROUND The maximum outer diameter (MOD) of the appendix is an essential parameter for diagnosing acute appendicitis,but there is space for improvement in ultrasound (US) diagnostic performance.AIM To investigate whether combining the ratio of the cross diameters (RATIO) of the appendix with MOD of the appendix can enhance the diagnostic performance of acute appendicitis.METHODS A retrospective study was conducted,and medical records of 233 patients with acute appendicitis and 112 patients with a normal appendix were reviewed.The MOD and RATIO of the appendix were calculated and tested for their diagnostic performance of acute appendicitis,both individually and in combination.RESULTS The RATIO for a normal appendix was 1.32 ± 0.16,while for acute appendicitis it was 1.09 ± 0.07.The cut-off value for RATIO was determined to be ≤ 1.18.The area under the receiver operating characteristic curve (AUC) for diagnosing acute appendicitis using RATIO ≤ 1.18 and MOD > 6 mm was 0.870 and 0.652,respectively.There was a significant difference in AUC between RATIO ≤ 1.18 and MOD > 6 mm (P < 0.0001).When comparing the combination of RATIO ≤ 1.18 and MOD > 6 mm with MOD > 6 mm alone,the combination showed increased specificity,positive predictive value (PPV),and AUC.However,the sensitivity and negative predictive value decreased.CONCLUSION Combining RATIO of the appendix ≤ 1.18 and MOD > 6 mm can significantly improve the specificity,PPV,and AUC in the US diagnosis of acute appendicitis.
Key Words: Acute appendicitis;Diameter;Ratio;Diagnosis;Ultrasound
lNTRODUCTlON
Acute appendicitis is the most common abdominal emergency in the world.The clinical diagnosis of acute appendicitis is based on history,physical examination,laboratory tests,and medical imaging.Although biomarkers and imaging are valuable adjuncts to history and physical examination,accurate preoperative diagnosis is still challenging[1].Ultrasound (US) has been recommended for the evaluation of suspected appendicitis in recent dacades[2].Previous studies[2-7] have showed that an appendix with a maximum outer diameter (MOD) of more than 6 mm,scanned at the point of maximum tenderness using US,is the main feature of acute appendicitis.Other findings include incompressibility of the enlarged appendix,presence of appendicoliths,equivocality or loss of mural stratification,increased echogenicity of periappendiceal epiploic appendages,abnormal anechoic focal fluid on graded compression US;and hypervascularity of the appendix wall.The diagnostic performance of US for acute appendicitis varies considerably.Previous studies show that the sensitivity and specificity of US for the acute appendicitis are 0.821 and 0.81,and 0.859 and 0.87,respectively,and the area under the receiver operating characteristic (ROC) curve is 0.9249[3,4].Chicaizaet al[7] found that the MOD of the appendix for the diagnosis of acute appendicitis should be 7 mm instead of 6 mm.The MOD and other features of acute appendicitis are diverse,and they are affected by many factors,which may cause a diagnostic dilemma.The normal appendix appears as an ovoid or round shape on transverse section;when the appendix undergoes acute inflammation,the appendiceal size and tension increase[8-10].With the progression of the appendix inflammation,the appendix becomes tumefaction,stiff,and incompressible,the shape on transverse section becomes round or closer to round (without perforation),and the ratio of cross diameters on transverse section becomes one or approximate to one[10,11].Herein,we hypothesize that taking a ratio of the cross diameters (RATIO) on the transverse section of the appendix as an additional diagnostic US parameter is helpful for the evaluation of the appendix.The objective of this study was to investigate whether a combination of the RATIO of the appendix and the MOD of the appendix is valuable for the diagnosis of acute appendicitis.
MATERlALS AND METHODS
Study population
In this cross-sectional retrospective study,medical documents of 21624 consecutive patients who had undergone US of the appendix for suspected acute appendicitis between January 2017 and August 2023 in a tertiary hospital were retrieved,and some selected materials were reviewed.The inclusion criteria were that the patients who underwent US evaluation,the quality of US images was eligible,the patients underwent appendectomy,and the patients without acute appendicitis according to US,other examinations and clinical management.The exclusion criteria were that the patients with acute appendicitis did not have US images (undetected),acute appendicitis occurred perforation,pregnant women in the second and third trimesters,patients with a huge abdominal or pelvic tumor,and appendicitis with appendiceal tumor coexist.If a patient underwent two or more appendiceal US,only the latest US images and results were included.Based on these inclusion and exclusion criteria,1033 patients were recruited,and 20591 patients were excluded.Finally,233 patients [37.0 years (interquartile range: 28.0,49.5)] with US-detected acute appendicitis and undergoing surgical excision were included,and 112 patients [median 31.0 years (interquartile range: 24.0,39.8)] were selected in a randomized way from 9967 of 20591 patients with the final diagnoses of a normal appendix other than chronic bowel inflammation after US and other examination as a control.The diseases of the patients with a normal appendix included 39 cases of stone in the right ureter and/or kidney,16 cases of gastritis,17 cases of ovarian benign diseases,13 cases of nonspecific fallopian tube inflammation,5 cases of psoas injury,9 cases of mesenteric lymphadenitis,and 3 cases of gastric ulcer.Baseline characteristics of the patients with a normal appendix and acute appendicitis are summarized and compared in Tables 1 and 2.
Acquisition of US images of the appendixes
Patients who were referred to a tertiary hospital with suspected acute appendicitis received an appendix examination by physicians skilled in US.These physicians had between 1 to 30 years of experience in performing appendix USs.Multiparameter US systems (Mindray DC 8,Aloka Prosound α-7,Aloka Prosound α-10,Mindray Resona 7,Phillips EPIQ5,and GE Logiq E9) with a linear array transducer were used for the examination.The working frequencies ranged from 10 MHz to 15 MHz,but lower frequencies were used if the appendix could not be visualized.
During the examination,the US systems were adjusted to the small parts mode for bowel imaging.The patients were positioned supine on the table with their abdominal region fully exposed.The bowel and abdominal cavity were carefully scanned to detect any abnormalities.A graded compression US protocol was performed,allowing visualization of the right psoas muscle and right external iliac artery and vein during compression.Once the appendix was visualized,various characteristics were examined,including its location,shape,size,boundary,luminal and mural echogenicity,thickness and stratification of the appendiceal wall,vascularity,mesoappendix,periappendiceal epiploic appendages,omentum,periappendiceal fluid,and any associating findings (such as lymphadenitis).The size of the appendix was determined at its greatest dimension in both longitudinal and transverse views.The measurement of size in the transverse view was taken at the middle part of the appendix,neither the proximal nor the distal part.Color Doppler flow imaging was used to detect appendiceal vascularity or mural hyperemia.Representative images were saved in the informatics database of the picture archiving and communications system.Figures 1 and 2 show representative sonographies of a normal appendix and acute appendicitis,respectively.
Interpretation of the US images of the appendixes
Two physicians-in-US (radiologists) (a junior with 2 years and a senior physician with 20 years of abdominal US experience) evaluated the images of all the patients.They assessed the shape,size,echogenicity of the appendiceal lumen and wall,thickness and lamina of the appendiceal wall,the ratio on transverse section (dividing the larger diameter by the smaller diameter),appendicolithiasis,and vascularity.Appendicolithiasis was defined as an intraluminal echogenic focus or foci with distal acoustic shadowing.Luminal obstruction was defined as appendicolithiasis in the proximal lumen and was accompanied by fluid or other substances filling the lumen.Fluid in the appendiceal lumen and vascularity in the appendiceal wall were also specific findings for appendicitis.However,the vascularity of the appendiceal wall was difficult to detect by color Doppler flow imaging in the majority of the patients,so the analysis of fluid in the appendiceal lumen and the mural vascularity was waived.The appendix was considered enlarged when its MOD was 6 mm or larger under compression,measured from outer wall to outer wall in the transverse section[2].Appendiceal wall edema was defined as an obliteration of the layers.Uncomplicated appendicitis was defined as the presence of an enlarged appendix with or without luminal liquid and appendicolithiasis,where the appendiceal wall was continuous,and no periappendiceal fluid was identified.
Histopathological classification
The histopathology of acute appendicitis and its grade was recorded based on the post-surgical evaluation,which was assessed by two certified pathologists.Acute appendicitis was classified as phlegmonous,gangrenous,and perforated appendicitis.
Statistical analysis
Continuous variables with a normal distribution were represented as mean ± SD,while those that did not meet the normal distribution were represented as median (interquartile range).The Kolmogorov-Smirnov test was used for the distribution analysis.Categorical variables were represented as numbers (percentage).Primary descriptive statistics of the study were reported.Independent samplet-test and Mann-WhitneyUtest were used for the analysis of continuous variables with and without a normal distribution,respectively.The diagnostic performance of acute appendicitis was studied based on MOD > 6 mm on the transverse section of the appendix and a combination of RATIO ≤ 1.18 and MOD > 6 mm,as determined by literature and this study[2].Theχ2test was used for the analysis of categorical variables.McNemar test was used to test the sensitivity,specificity positive predictive value (PPV),and negative predictive value (NPV).The ROC curve was drawn,the area under the ROC curve (AUC) was calculated,and the Youden index was determined to establish the cut-off value for sensitivity and specificity.PPV and NPV were also calculated.All analyses were conducted using SPSS software for Windows,version 26 (IBM Corp,Armonk,NY,United States) and/or Medcalc statistical software version 15.2.2 (Medcalc software BVBA,Ostend,Belgium).A two-tailedP< 0.05 was considered statistically significant.
RESULTS
The MODs and RATIOs of the normal appendix and acute appendicitis were 6.5 ± 1.0 mm and 10.7 ± 2.2 mm,and 1.32 ± 0.16 and 1.09 ± 0.07,respectively,with significant differences between them (allP< 0.001).The MODs on the transverse section and RATIOs of the normal appendix and acute appendicitis were all normally distributed.The baseline demographic characteristics of the patients and color Doppler US characteristics of the appendix with and without acute inflammation are summarized in Table 1.The ROC curve based on the RATIO of the 233 appendixes showed an AUC of 0.870 (95% confidence interval of 0.830-0.904),the best cutoff value for the RATIO of the appendix in diagnosing acuteappendicitis was ≤ 1.18,with a sensitivity of 91.0% and specificity of 83.0%.The AUC for the RATIO and MOD > 6 mm on the transverse section of the appendix for predicting acute appendicitis were 0.870 and 0.652,respectively;with a significant difference in AUC between RATIO ≤ 1.18 and MOD > 6 mm (P< 0.0001).The MOD > 6 mm on the transverse section of the appendix for diagnosing acute appendicitis had a sensitivity of 99.1%,specificity of 31.3%,and AUC of 0.652.The combination of RATIO ≤ 1.18 and MOD > 6 mm on the transverse section of the appendix for diagnosing acute appendicitis had a sensitivity of 90.1%,specificity of 92.0%,PPV of 95.9%,NPV of 81.7%,and AUC of 0.910.When comparing the combination of RATIO ≤ 1.18 and MOD > 6 mm to MOD > 6 mm alone for diagnostic performance,there was a significant increase in specificity,PPV,and AUC,but a decrease in sensitivity and NPV.The diagnostic performances of different reference criteria for the evaluating acute appendicitis are shown in Table 2.Figure 3 illustrates the comparisons among the AUCs of RATIO,MOD > 6mm,and the combination of RATIO ≤ 1.18 and MOD > 6 mm.

Figure 1 A normal appendix. A: On the longitudinal view,the appendix appears as a blind-ending structure extending from the cecum in the abdominal cavity,the mural structures are clearly visible,there is no filling in the lumen,and the mucosa appears slightly hyperechoic with a thread-like appearance;B: On the transverse view,the appendix appears as an ovoid shape,the mural structures are visible,there is no filling in the lumen,and the ratio of the cross diameters on the transverse section is 5.9/5.3=1.11.Subsequent ultrasound examination revealed that the patient had a right ureter stone (not shown).
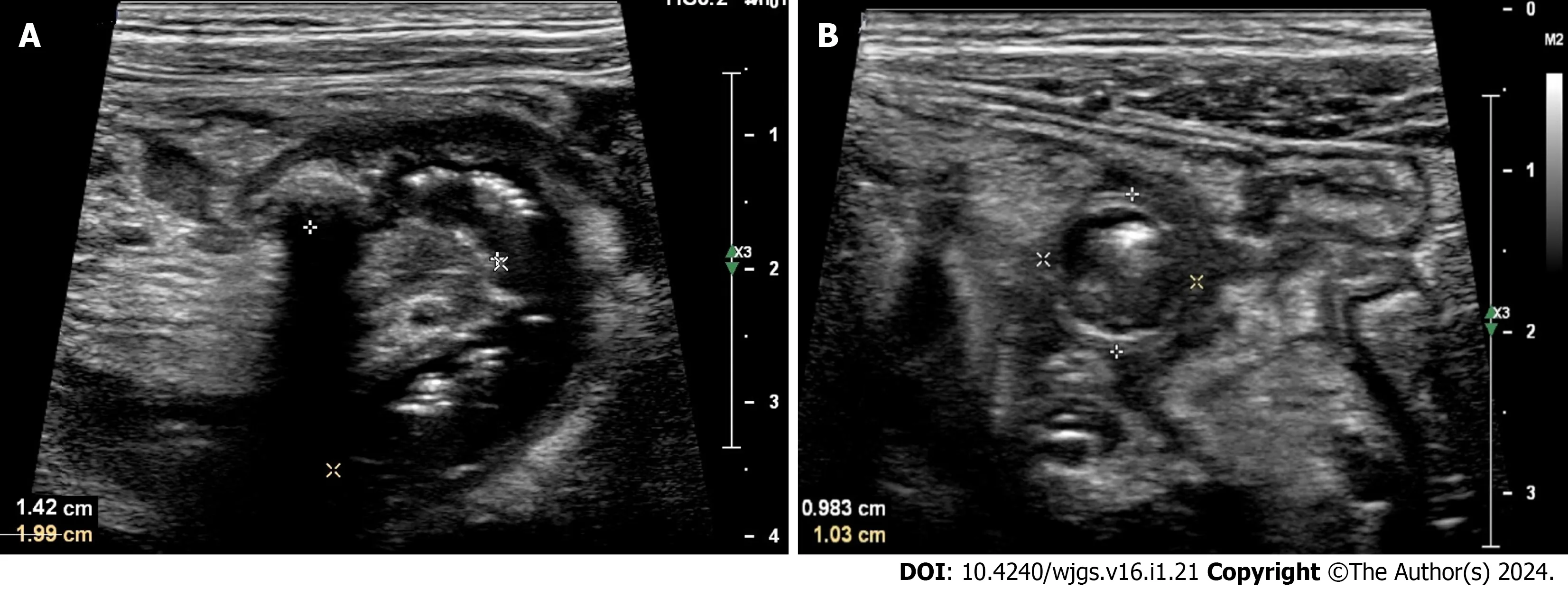
Figure 2 Acute appendicitis. The images obtained using ultrasound from a 12-year-old female patient who presented with right inferior quadrant abdominal pain,tenderness of the abdominal wall,and abdominal guarding.A: On the longitudinal view,the appendix appears as a bent,blind-ending tubular structure extending from the cecum,the mural structures of the appendix are unclear,and there are heterogeneous complex echogenic fillings in the lumen;B: On the transverse view,the appendix appears as a round shape,with dilating lumen,there are heterogeneous complex echogenic fillings in the lumen,and the ratio of the cross diameters on the transverse section is 10/9.8=1.02.Postoperative histopathology confirmed that the patient had acute phlegmonous appendicitis.

Figure 3 The receiver operating characteristic curves of ratio of the cross diameters on transverse section of the appendix,maximum outer diameter> 6 mm,and maximum outer diameter > 6 mm+ratio of the cross diameters on transverse section of the appendix.MOD: Maximum outer diameter;AUC: Area under the receiver operating characteristic curve;RATIO: Ratio of the cross diameters of the appendix.
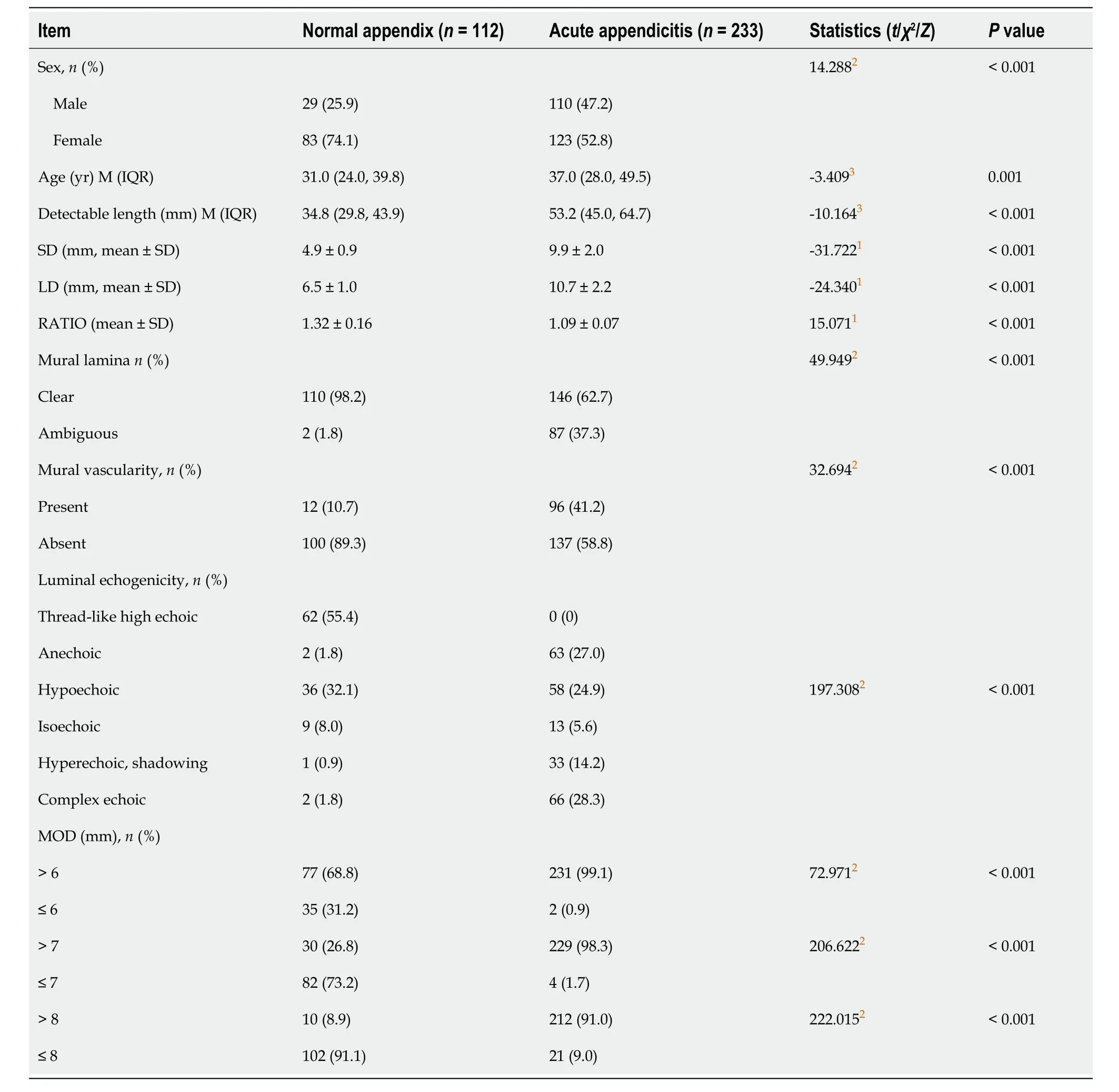
Table 1 The baseline characteristics of the patients with a normal appendix and acute appendicitis and sonographic characteristics

Table 2 Diagnostic performances of different criteria for evaluating acute appendicitis
DlSCUSSlON
The clinical manifestations of acute appendicitis vary greatly,and the diagnosis is usually comprehensive,often requiring medical imaging for many patients with suspected acute appendicitis[1].US is an important technique in the study of appendicitis.A meta-analysis has shown that US,computed tomography,and magnetic resonance imaging have comparable and high accuracy in helping diagnose appendicitis[12].In experienced sonographers or physicians-in-US,US can visualize the appendix in the majority of the examined population,except for obese individuals[11,13].However,some patients may have equivocal sonographic features of the appendix,resembling both a normal appendix and acute appendicitis,such as a slightly thickened appendix or an ovoid shape on transverse section[14].A study by Sezeret al[14] reported that US for the evaluation of acute appendicitis had an overall sensitivity of 71.4%,specificity of 78.5%,PPV of 94.8%,NPV of 33.3%,and accuracy of 72.5%.This suggests that US alone may not be satisfactory for the diagnosis of acute appendicitis.Rettenbacheret al[15] found that the presence of an ovoid shape on the transverse section of the appendix,covering the entire appendiceal length on US,can reliably rule out acute appendicitis.However,distinguishing between an ovoid shape and a round shape on sonography can sometimes be challenging when the two cross diameters have a marginal difference.In such cases,introducing the RATIO as a quantifying variable to characterize and analyze the features of the appendix may provide a more objective and reliable approach.
When using MOD > 6 mm as a reference for evaluating the appendix,the outcomes were a sensitivity of 99.1%,specificity of 31.3%,PPV of 75.0%,NPV of 94.6%,and AUC of 0.652.These results were lower than those reported by Rettenbacheret al[5],which showed a sensitivity of 100%,specificity of 68%,NPV of 100%,accuracy of 79%,and a lower PPV of 63%.The difference in sample size may contribute to the variation in outcomes.This finding is consistent with the study by Chicaizaet al[7],where using a cutoff of MOD 6 mm resulted in sensitivity and specificity of 100% and 43%,respectively,while using a cutoff of MOD 7 mm decreased the sensitivity to 94% and increased the specificity to 71%.Previous studies[16,17] have shown that lymphoid hyperplasia of the appendix,due to hypertrophy of lymphoid follicles in response to gastrointestinal inflammatory diseases,chronic constipation,and cystic fibrosis,can increase the MOD of the appendix.This can result in a noncompressible appendix with a borderline size of 6-8 mm in outer diameter,potentially leading to false-positive diagnoses of acute appendicitis based on MOD[16,17].
In this study,when using MOD > 6 mm and a combination of RATIO ≤ 1.18 and MOD > 6 mm as references for evaluating the appendix,the AUC of the combination of RATIO ≤ 1.18 and MOD > 6 mm increased significantly,along with an increase in specificity and PPV,and a decrease in sensitivity and NPV compared to using MOD > 6mm alone.These findings indicate that the combination of RATIO ≤ 1.18 and MOD > 6mm can address the bias of using MOD > 6 mm alone and significantly improve specificity,PPV,and AUC.
The strengths of this study include a large sample of patients with histopathologically confirmed acute appendicitis,ensuring the reliability of the results.Additionally,the establishment of the RATIO of cross diameters on the transverse section of the appendix introduces a new concept,adding valuable information to the existing literature.
There were some potential limitations in this study.Firstly,the retrospective study design may have resulted in the loss of certain information regarding the appendiceal structure.Secondly,patients with appendiceal perforation and appendiceal tumors were excluded,which means that not all US features of acute appendicitis were collected and analyzed.The appendiceal MOD in patients with appendiceal perforation may be smaller than 6 mm,and the shape and RATIO of the cross diameters on the transverse section of the appendix may differ from those without appendiceal perforation.Additionally,the inter-and intra-observer agreements of appendiceal measurements by different US performers were not determined due to the retrospective design,which may have affected the overall analysis of acute appendicitis.Furthermore,the patients without appendiceal identification and the US visualization rate of the appendix were not analyzed.This may have resulted in missed diagnoses of acute appendicitis with false-negative results,and nonappendiceal findings may have been present alongside appendiceal findings,which were not analyzed.These limitations may compromise the complete understanding of the vermiform appendix and acute appendicitis in this study.
CONCLUSlON
A combination of a ratio ≤ 1.18 on the cross diameters on the transverse section of the appendix and MOD > 6 mm can significantly increase the specificity,PPV,and AUC compared to using MOD > 6 mm alone.
ARTlCLE HlGHLlGHTS
Research background
Ultrasound (US) is commonly used for diagnosing acute appendicitis,but the diagnostic performance remains for further improvement.The size of the appendix is crucial for distinguishing between a normal appendix and acute appendicitis.
Research motivation
The maximal outside diameter on the cross section of the appendix > 6 mm has been recommended as a cut-off value for diagnosing acute appendicitis,but the minimal outside diameter and the ratio of the two outside diameters have not been adequately studied.
Research objectives
To investigate if the ratio of the two outside diameters on the cross section of the appendix is a useful parameter for diagnosing acute appendicitis.
Research methods
The investigators measured the two outside diameters on the cross section of a normal appendix and acute appendicitis without perforation using ultrasonography and calculated their ratio.The diagnostic performance of the maximal outside diameter,the ratio of two diameters on the cross section of the appendix,and their combination were compared.
Research results
A ratio of the diameter on the cross section of the appendix ≤ 1.18 was identified as a cut-off value for predicting acute appendicitis.The diagnostic performance based on the ratio of two diameters on the cross section of the appendix ≤ 1.18 was significantly higher than that of the maximal outside diameter.
Research conclusions
Combining the maximal outside diameter and the ratio of two diameters on the cross section of the appendix improved diagnostic performance compared to using the maximal outside diameter alone.
Research perspectives
Further prospective studies are needed to validate the findings and the use of a combination of the maximal outside diameter and the ratio of two diameters for US diagnosis of acute appendicitis.
FOOTNOTES
Author contributions:Gu FW participated in the study design,obtained the materials,analyzed the data,and wrote the first manuscript;Wu SZ participated in the study design,data obtaining and analysis,and wrote and revised the manuscript;all authors read and approved the final manuscript.
lnstitutional review board statement:The study was approved by the ethics committee of First Affiliated Hospital of Hainan Medical University.
lnformed consent statement:No informed consent was required,because the data are anonymized.
Conflict-of-interest statement:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Data sharing statement:Technical appendix,statistical code,and dataset available from the corresponding author at wsz074@aliyun.com.
STROBE statement:The authors have read the STROBE Statement-checklist of items,and the manuscript was prepared and revised according to the STROBE Statement-checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Si-Ze Wu 0000-0002-1086-764X.
S-Editor:Qu XL
L-Editor:A
P-Editor:Xu ZH
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Prospects in the application of ultrasensitive chromosomal aneuploidy detection in precancerous lesions of gastric cancer
- Prognostic value of ultrasound in early arterial complications post liver transplant
- Single-incision laparoscopic transabdominal preperitoneal repair in the treatment of adult female patients with inguinal hernia
- Predictive value of machine learning models for lymph node metastasis in gastric cancer: A two-center study
- Micro-power negative pressure wound technique reduces risk of incision infection following loop ileostomy closure
- Unraveling the efficacy network: A network meta-analysis of adjuvant external beam radiation therapy methods after hepatectomy