Efficacy observation of long-time needle retaining at Baihui (GV20) combined with multidirectional pointtoward-point needle insertion with needle shaking at Fengchi (GB20) for cervical vertigo
2024-02-27GUOMin郭敏TONGXiang童翔SONGKaiyi宋开义
GUO Min (郭敏), TONG Xiang (童翔), SONG Kaiyi (宋开义)
1 Chun’an County Hospital of Traditional Chinese Medicine, Zhejiang Province, Hangzhou 311700, China
2 Center for Rehabilitation Medicine, Rehabilitation & Sports Medicine Research Institute of Zhejiang Province, Department of Rehabilitation Medicine, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou 310014, China
Abstract Objective: To observe the clinical curative effect of long-time needle retaining at Baihui (GV20) combined with multidirectional point-toward-point needle insertion with needle shaking at Fengchi (GB20) for the treatment of cervical vertigo (CV) and its influence on the blood flow velocity of vertebrobasilar arteries.
Keywords: Acupuncture Therapy; Point-toward-point Needling Method; Point, Baihui (GV20); Point, Fengchi (GB20); Vertigo;Vertebrobasilar Insufficiency; Blood Flow Velocity
Cervical vertigo (CV), the major type of vertigo, is a clinical syndrome caused by an insufficient blood supply to the extracranial segment of the carotid artery and vertebrobasilar arteries as a result of irritation to and compression on the surrounding nerves and blood vessels originating from the cervical spine[1-3].Epidemiological studies have shown that the prevalence of vertigo ranges from 1.78% to 35.4%[4-5]and tends to increase with age[6].However, patients are becoming younger in recent years[7].Current research on the pathogenesis of CV is multifaceted[8-9].Regardless of the theory, it is generally believed that CV is mainly caused by the destruction of the structural and mechanical balance of the head, neck, and surrounding tissues[10],especially dysfunction of the suboccipital muscle group[11-12], plays an important role in the development of CV.Based on the importance of the suboccipital muscles in the pathogenesis of CV and the precise targeting of treatment, as well as previous experience with long-time needle retaining at Baihui (GV20) for the treatment of CV[13-15], in this study, we investigated the efficacy of long-time needle retaining at Baihui (GV20)combined with multidirectional point-toward-point needle insertion with needle shaking at Fengchi (GB20)and its effects on the blood flow velocity of vertebrobasilar arteries.
1 Clinical Materials
1.1 Diagnostic criteria
We referred to the diagnostic criteria developed by theProceedings of the Third National Symposium on Cervical Spondylosisin 2008[16]: vertigo, dizziness,blurred vision, and other symptoms related to neck activities, often induced or aggravated by sudden head rotation and accompanied by vagus nerve excitation signs such as palpitations, nausea, vomiting, and sweating; cervical-occipital pain, headache, tension and stiffness of neck muscles; tenderness on the spinous process of the cervical spine or on both sides of the spinous process, limited cervical flexion and extension and a positive neck rotation test on physical examinations; cervical vertebral hyperplasia and instability, such as atlantoaxial or atlantodental joint instability, cervical instability, hook vertebral joint hyperplasia, and narrowing of the vertebral space indicated on cervical spine X-ray, CT, or MRI examinations; vertigo not caused by other diseases,such as cardiogenic, ophthalmologic, and otogenic vertigo, or intracranial lesions, such as tumors and simple psychogenic neurosis.
1.2 Inclusion criteria
Patients met the diagnostic criteria for CV; aged between 25 and 70 years; those who provided the informed consent; those who would cooperate with the treatment and could adhere to the plan for the entire treatment.
1.3 Exclusion criteria
Did not meet the inclusion criteria; had a history of neck trauma; had a concomitant serious cardiovascular or cerebrovascular disease, diabetes mellitus,psychiatric disease, bone tuberculosis, or bone tumor;pregnant or lactating; had another disease-causing vertigo, such as otogenic or ophthalmologic vertigo; had a brainstem, cerebellar or brain lesion.
1.4 Criteria for elimination and dropout
Refused to receive treatment after inclusion, though they met the inclusion criteria; experienced serious adverse reactions during the treatment and could not continue the treatment; could not complete the whole course of treatment as required or ended treatments on their own due to its poor efficacy; voluntarily requested to withdraw from the study for other reasons;lost contact and could not provide follow-up data.
1.5 Statistical methods
The SPSS version 27.0 statistical analysis software was applied to process the data, and measurement data all conformed to a normal distribution and were expressed as mean ± standard deviation (±s).The intra-group comparisons were analyzed by one-way analysis of variance, and the between-group comparisons were analyzed using the independent samplest-test.The count data were expressed as cases,and comparisons were made using the Chi-square test.P<0.05 was considered statistically significant.
1.6 General data
Between January 2021 and December 2021, 70 patients with CV visiting the Rehabilitation Department of Chun’an County Hospital of Traditional Chinese Medicine, Zhejiang Province were enrolled and randomly divided into a treatment group and a control group using random numbers generated by the SPSS version 27.0 statistical software, with 35 cases in each group.During the study, two patients in the control group and one in the treatment group dropped out.Of those, one patient in the control group did so because he could not complete the treatment after being transferred to another province for work, and the other two could not complete the treatment due to the pandemic.A total of 67 patients were finally included(33 in the control group and 34 in the treatment group).The differences in gender, age, and disease duration between the two groups were not statistically significant (P>0.05), and the groups were comparable(Table 1).The study was approved by the Ethics Committee of Chun’an County Hospital of Traditional Chinese Medicine, Zhejiang Province (Approval No.2021002).

Table 1 Comparison of the general data between the two groups
2 Treatment Methods
2.1 Control group
Patients in the control group were treated using conventional acupuncture.
Points: Baihui (GV20), Fengchi (GB20), Touwei (ST8),Taiyang (EX-HN5), Xuanzhong (GB39), Qihai (CV6),Xuehai (SP10), and Zusanli (ST36).
Method: The points were selected according to the prescribed treatment of vertigo in theAcupuncture and Moxibustion Therapeutics[17].The patient was asked to take a supine position and underwent routine sterilization.A filiform needle of 0.25 mm in diameter and 40 mm in length was subcutaneously inserted into Baihui (GV20) backward by 0.5-0.8 Cun; obliquely punctured Fengchi (GB20) toward the tip of the nose by 0.8-1.2 Cun, subcutaneously punctured Touwei (ST8)and Taiyang (EX-HN5) by 0.5-1.0 Cun backward, and perpendicularly punctured Xuanzhong (GB39), Zusanli(ST36), Qihai (CV6), and Xuehai (SP10) by 1.0-1.5 Cun.The manipulation was based on twisting and rotating with a balanced reinforcing and reducing manipulation,producing soreness, numbness, and heaviness at each point.The needles were retained for 30 min, and the treatment was performed every other day, 7 sessions as a treatment course, for a total of 2 courses.
2.2 Treatment group
The treatment for patients in the treatment group was performed with long-time needle retaining at Baihui (GV20) combined with multidirectional pointtoward-point needle insertion with needle shaking at Fengchi (GB20).
Points: Baihui (GV20), Fengchi (GB20), Fengfu (GV16),Tianzhu (BL10), and Yiming (EX-HN14).
Method: After routine sterilization, an acupuncture needle with a resin handle (0.25 mm in diameter and 40 mm in length) was used to puncture Baihui (GV20).Following the direction of the Governor Vessel, the needle tip was punctured at an angle of 15-30° relative to the scalp and quickly inserted into the subcutaneous layer.When the needle tip reached the subgaleal tissue,the resistance under the fingers decreased, allowing the needle body to lie flat and parallel to the scalp with a depth of approximately 35 mm.Then, a gentle twirling and rotating manipulation was performed so that the needle was neither too tight nor too loose.Most of the resin needle handle was then cut off, leaving only a small part (to prevent the exposed needle handle outside the scalp from being pressed or bumped by foreign objects).The needle was removed after 24 h of retaining.That was long-time needle retaining at Baihui(GV20).See Figure 1.For multidirectional point-towardpoint needle insertion with needle shaking at Fengchi(GB20), an acupuncture needle was first inserted into Fengchi (GB20) subcutaneously, with the needle body at 15° relative to the skin toward Fengfu (GV16).In the same way, the other two needles were inserted from Fengchi (GB20) toward Tianzhu (BL10) and from Fengchi(GB20) toward Yiming (EX-HN14).See Figure 2.Each needle body was then pressed with a disinfection swab and lifted to 90° by pinching the needle handle(Figure 3).Finally, all the needle handles were pinched together and shaken vertically for 5 min (Figure 4)before being removed.The same method was applied to the opposite Fengchi (GB20).Only the needle at Baihui (GV20) was retained for 24 h.The treatment was performed every other day, 7 sessions as a treatment course, for a total of 2 courses.

Figure 1 Long-time needle retaining at Baihui (GV20)

Figure 2 Multidirectional point-toward-point needle insertion

Figure 3 Folding of needle bodies to 90°

Figure 4 Vertical shaking of the needle handles
3 Observations of Therapeutic Efficacy
3.1 Observed indicators
3.1.1 Evaluation scale for symptoms and functions of cervical vertigo (ESCV)
The patients were evaluated before and after treatment using ESCV[18], which includes the following 5 aspects: vertigo (degree, frequency, and duration),degree of neck and shoulder pain, degree of headache,ability to perform daily life and work activities and psychological and social adaptation.
3.1.2 Mean blood flow velocity (Vm) of the vertebrobasilar arteries
Transcranial Doppler (TCD) ultrasonography was performed to record the changes in the Vm of the left vertebral artery (LVA), right vertebral artery (RVA), and basilar artery (BA) before and after treatment.The normal values of the test were determined by clinical Doppler ultrasonography[19].The normal reference values of the Vm were (31.26±4.90) cm/s for the LVA,(31.88±4.71) cm/s for the RVA, and (36.6±6.61) cm/s for the BA.The patients were classified according to the Vm of the vertebral arteries and BA before treatment as low-flow type (below the lower normal value), normalflow type (within the normal range), and high-flow type(above the upper normal value).
3.1.3 Occurrence of adverse reactions
The investigators recorded in detail any adverse reactions to needling, such as stagnant needles, broken needles, dizziness, and skin allergy or infection that occurred in patients during the treatment period.
3.2 Efficacy assessment criteria
The criteria applied to evaluating efficacy were as follows[20].
Cured: Complete disappearance of vertigo, relief from accompanying symptoms and signs, and a normal TCD examination.
Markedly effective: Nearly complete disappearance of vertigo, approximately normal TCD examination, and being able to live and work normally.
Effective: Relief from vertigo, reduction of accompanying symptoms and signs, an approximately normal TCD examination, and being able to continue working, but with influence on life and work.
Invalid: No change in vertigo, persistence of accompanying symptoms and signs, and no significant change in TCD examination.
The total effective rate was the percentage of the total number of people who were cured or showed markedly effective and effective.The cured plus markedly effective rate was the percentage of the total number of people who were cured and showed markedly effective.
3.3 Results
3.3.1 Comparison of the clinical efficacy
After treatment, the cured plus markedly effective rate in the treatment group was better than that in the control group (P<0.05), and the total effective rate in the treatment group was slightly higher than that in the control group, with no statistically significant difference(P>0.05), as detailed in Table 2.
3.3.2 Comparison of the ESCV score before and after treatment
The differences in all aspects of ESCV score between the two groups before treatment were not statistically significant (P>0.05).The ESCV scores of the two groups were significantly increased after treatment (P<0.05),and the ESCV scores in the treatment group were significantly higher than those in the control group(P<0.05), as shown in Table 3.
3.3.3 Comparison of the Vm in the vertebrobasilar arteries before and after treatment
Before treatment, the differences in the Vm of the LVA, RVA, BA (low flow rate, normal flow rate, and high flow rate) between the two groups were not statistically significant (P>0.05), and the values were comparable.After treatment, the flow rate of patients with low and normal flow rates in the treatment group was faster than that before treatment (P<0.05), and the flow rate of patients with a high flow rate was slower than that before treatment (P<0.05).The flow rates in the treatment group were significantly better than those in the control group (P<0.05), as shown in Table 4-Table 6.
3.4 Adverse reactions
During the treatment period, there were no adverse events in either group.

Table 2 Comparison of the clinical efficacy between the two groups Unit: case
Table 3 Comparison of the ESCV scores before and after treatment ( ±s) Unit: point
Note: ESCV=Evaluation scale for symptoms and functions of cervical vertigo; compared with the same group before treatment, 1)P<0.05; compared with the control group after treatment, 2) P<0.05.
Item Treatment group (n=34) Control group (n=33)Before treatment After treatment Before treatment After treatment Vertigo 6.56±2.32 14.57±1.461)2) 6.79±1.95 11.81±1.991)Neck and shoulder pain 2.08±0.71 3.62±0.551)2) 2.15±0.57 2.97±0.531)Headache 1.04±0.33 1.82±0.241)2) 1.11±0.37 1.51±0.291)Daily life and work 2.21±0.72 3.65±0.341)2) 2.39±0.58 3.17±0.471)Psychological and social adaptation 1.47±0.61 3.38±0.701)2) 1.51±0.57 2.76±0.711)
Table 4 Comparison of the Vm of the LVA before and after treatment ( ±s) Unit: cm/s
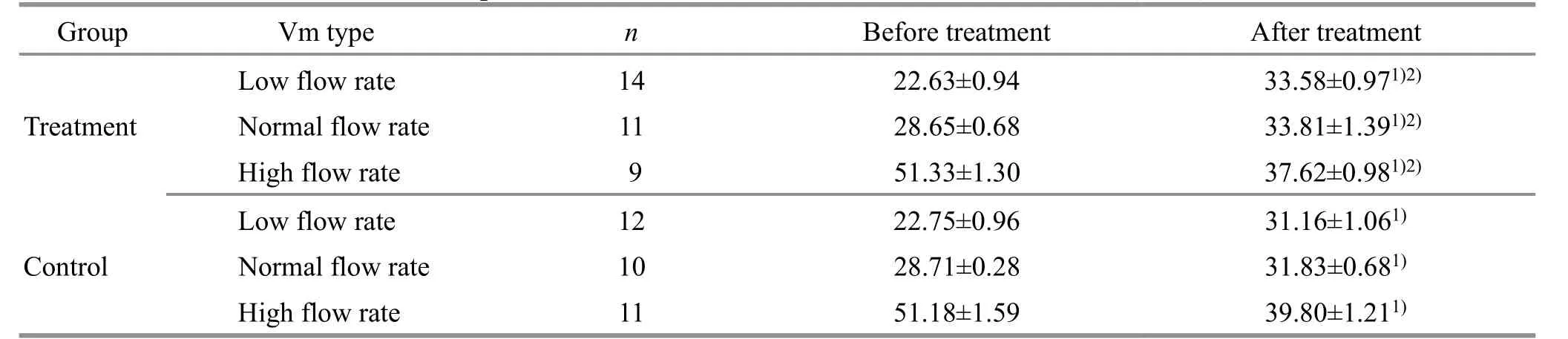
Table 4 Comparison of the Vm of the LVA before and after treatment ( ±s) Unit: cm/s
Note: Vm=Mean blood flow velocity; LVA=Left vertebral artery; compared with the same group before treatment, 1) P<0.05;compared with the control group after treatment, 2) P<0.05.
Group Vm type n Before treatment After treatment Low flow rate 14 22.63±0.94 33.58±0.971)2)Treatment Normal flow rate 11 28.65±0.68 33.81±1.391)2)High flow rate 9 51.33±1.30 37.62±0.981)2)Low flow rate 12 22.75±0.96 31.16±1.061)Control Normal flow rate 10 28.71±0.28 31.83±0.681)High flow rate 11 51.18±1.59 39.80±1.211)
Table 5 Comparison of the Vm of the RVA before and after treatment ( ±s) Unit: cm/s
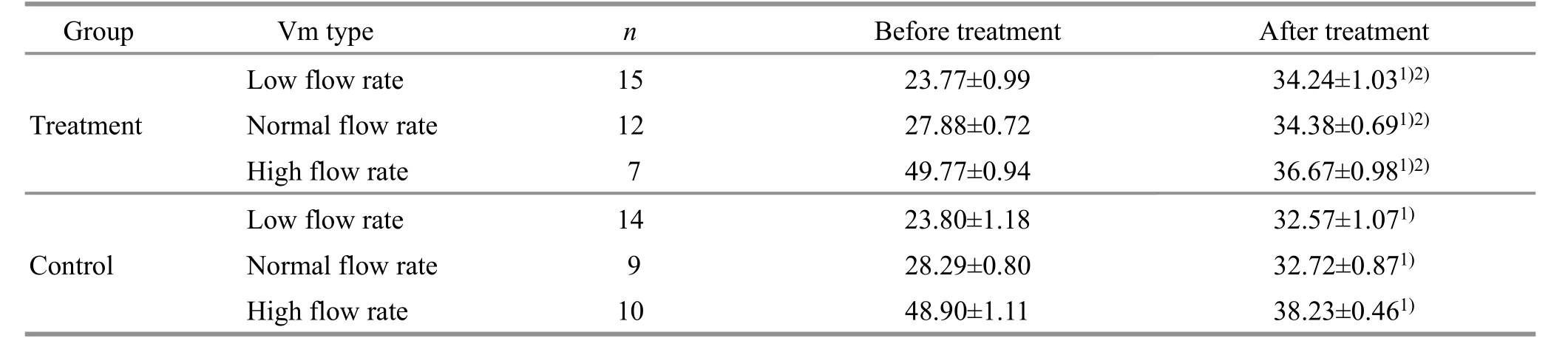
Table 5 Comparison of the Vm of the RVA before and after treatment ( ±s) Unit: cm/s
Note: Vm=Mean blood flow velocity; RVA=Right vertebral artery; compared with the same group before treatment, 1) P<0.05;compared with the control group after treatment, 2) P<0.05.
Group Vm type n Before treatment After treatment Low flow rate 15 23.77±0.99 34.24±1.031)2)Treatment Normal flow rate 12 27.88±0.72 34.38±0.691)2)High flow rate 7 49.77±0.94 36.67±0.981)2)Low flow rate 14 23.80±1.18 32.57±1.071)Control Normal flow rate 9 28.29±0.80 32.72±0.871)High flow rate 10 48.90±1.11 38.23±0.461)
Table 6 Comparison of the Vm of the BA before and after treatment ( ±s) Unit: cm/s
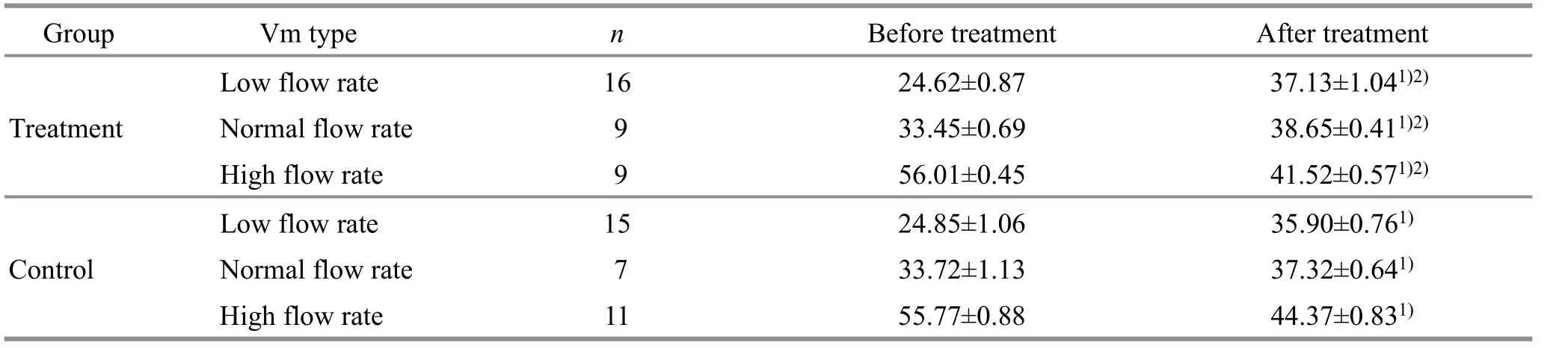
Table 6 Comparison of the Vm of the BA before and after treatment ( ±s) Unit: cm/s
Note: Vm=Mean blood flow velocity; BA=Basilar artery; compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05.
Group Vm type n Before treatment After treatment Low flow rate 16 24.62±0.87 37.13±1.041)2)Treatment Normal flow rate 9 33.45±0.69 38.65±0.411)2)High flow rate 9 56.01±0.45 41.52±0.571)2)Low flow rate 15 24.85±1.06 35.90±0.761)Control Normal flow rate 7 33.72±1.13 37.32±0.641)High flow rate 11 55.77±0.88 44.37±0.831)
4 Discussion
CV is a common and frequent clinical disease.It was first proposed by RYAN G and COPE S in 1955 that vertigo syndrome is mainly caused by the extracranial segment of the vertebral artery being affected by cervical lesions, resulting in impaired blood flow[1].It has been shown that soft tissue lesions of the neck,especially those causing dysfunction of the suboccipital muscle group, play a key role in the development of CV[21-22].The blood vessels and nerves passing through the suboccipital muscle group include the vertebral artery, the occipital artery, the inferior occipital nerve,the greater occipital nerve, and the greater auricular nerve.Tense muscles can compress the sheaths around the nerves in the neck, thereby aggravating contracture and disrupting the balance of tension between the muscles in the neck.Over time, displacement of the atlantoaxial joint and various small joints can narrow the intervertebral foramen, which is the root cause of shoulder and neck pain and vertigo[23-25].Therefore,improving the contraction and stiffness of the suboccipital muscle groups may be the key to treating CV.
There have been many clinical studies on acupuncture for CV focusing on applying special forms of acupuncture[26-29], selecting optimal points[30], and quantifying the parameters of different waveforms in electroacupuncture[31].However, there have been few studies on acupuncture techniques for the treatment of CV, especially on fast-acting, simple, and safe acupuncture techniques to relax the suboccipital muscles.In this study, the efficacy and possible mechanism of an acupuncture technique in the treatment of CV were investigated in depth to provide new ideas for the clinical treatment of CV.
Our research group has accumulated rich clinical experience in the treatment of CV and has successively created “long-time needle retaining at Baihui(GV20)”[13-15], “four points for brain disorders”[14], and“unblocking the Governor Vessel”[32].Additionally, our group has also researched and proven the close relationship between the Conception and Governor Vessels and CV[33].Recently, based on previous research on multidirectional point-toward-point needle insertion with needle shaking at tender points and much literature research and long-term clinical experience,our group created multidirectional point-toward-point needle insertion with needle shaking at Fengchi (GB20).This method is based on relaxing needling techniques and improvements in traditional Qi-boosting techniques,with one point leading to the surface and a combination of the point and surface, as well as the mesh-like surface, for the rapid transmission of meridian Qi and improvement in CV.Multidirectional point-toward-point needle insertion with needle shaking at Fengchi (GB20)adopts multiple needles at Fengchi (GB20), from Fengchi (GB20) toward Fengfu (GV16), Tianzhu (BL10),and Yiming (EX-HN14).The method mainly consists of subcutaneous needling with 30 mm lateral penetration depth, pressing the needle body using a disinfection swab, lifting the needle body to 90°, and vertically shaking the needle by pulling the handle up and down,thereby loosening the subcutaneous fascia in the affected area, reducing the tension, pain, and spasm severity of the suboccipital muscle group, and improving the cervical-basilar artery supply.Overall, this method improves vertigo by improving the blood supply to vertebrobasilar arteries.Multidirectional point-toward-point needle insertion with needle shaking at Fengchi (GB20) has two theoretical bases.First, the reason for combining the relaxing needling techniques with needle shaking is that contracture and stiffness of the suboccipital muscle group fall under the category of tendon paralysis in Chinese medicine.The relaxing needling technique is a single-needle multidirectional pricking method to treat tendon paralysis that can significantly expand the needling surface, expand the effect of needling, and improve the overall efficacy of needling[34].Therefore, relaxing needling techniques are preferred in the treatment of tendon diseases.In addition, it has been found that the relaxing needling technique has the effect of loosening adhesions and moving and promoting Qi and is representative of prizing puncture[35].With the multidirectional point-toward-point method, the effect of needling on the muscle group is expanded from a point on the surface to a network of loosening, and vertical shaking of the needle handle encourages the meridian Qi to arrive quickly, thus loosening and separating painful subcutaneous nodes and curing pain.Second, in terms of anatomical structure, Fengchi (GB20)is located below the occipital bone.The liver and gall bladder are externally and internally related to each other; as a key point of the Gallbladder Meridian,Fengchi (GB20) can clear the hyperactivity of the liver and gallbladder Yang, dispel wind and phlegm, and unblock meridians, and is a generic point for dizziness and light-headedness.Anatomically, it is located at the atlantoaxial spinal segment, where the vertebral artery undergoes a major bend and crosses the atlantooccipital fascia through the vertebral artery sulcus to the occipital foramen (the atlantovertebral segment of the vertebral artery).This is the segment where the vertebral artery is most likely to be compressed, affecting the blood supply to the basilar artery[36].The deep part of Fengfu (GV16) is also at the atlantoaxial spinal segment, which is covered by branches of the third cervical nerve and the occipital nerve.Tianzhu (BL10) corresponds with the penetration point of the greater occipital nerve, and Yiming(EX-HN14) corresponds with the penetration point of the lesser occipital nerve.These are all useful for treating vertigo; thus, Fengchi (GB20) is used with multidirectional point-toward-point needle insertion,namely, from Fengchi (GB20) toward Fengfu (GV16),Tianzhu (BL10), and Yiming (EX-HN14), to enhance the therapeutic effect.
The ESCV score of the patients in the treatment group was significantly higher than that in the control group, and the cured plus markedly effective rate in the treatment group was significantly better than that in the control group.This indicates that using the method of long-time needle retaining at Baihui (GV20) and multidirectional point-toward-point needle insertion with needle shaking at Fengchi (GB20) to treat CV can significantly improve the clinical symptoms and reduce the impact of the disease on patients’ lives.
TCD is simple, painless, noninvasive, economical,convenient, and repeatable, and it can directly and noninvasively detect blood flow velocity, blood flow direction, and spectral changes in vertebrobasilar arteries.It is widely used in the diagnosis of CV and assessments of therapeutic efficacy[37].Therefore, in this study, TCD was used to observe the effects of longtime needle retaining at Baihui (GV20) combined with multidirectional point-toward-point needle insertion with needle shaking at Fengchi (GB20) on the Vm of vertebrobasilar arteries.The results indicated that the efficacy of this treatment for CV might relate to the improvement in vertigo symptoms by regulating the blood flow rate of vertebrobasilar arteries.In addition,in this study, CV was found to exist in three functional states based on the blood flow rate, namely, a low, a normal (mainly low to moderate), and a high flow rate,with low and normal flow rates accounting for the largest proportion of cases.The two methods have a synergistic, bidirectional regulatory effect, allowing the blood flow rate of vertebrobasilar arteries to return to normal.
Nevertheless, this study has shortcomings, such as a small sample size and a lack of more objective evidence.It can be further expanded in the future to become a multi-center, large-scale clinical trial.In conclusion, this study has broadened the effect of acupuncture manipulation on CV and tentatively confirmed that long-time needle retaining at Baihui (GV20) combined with multidirectional point-toward-point needle insertion with needle shaking at Fengchi (GB20) can improve patients’ ESCV and regulate the vertebrobasilar blood flow velocity in both directions, with improved clinical efficacy, and can thus be used as an effective method for treating CV.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
This work was supported by the Health Science and Technology Program of Hangzhou City, Zhejiang Province(浙江省杭州市卫生科技计划项目, No.B20210062);Zhejiang Provincial Medical and Health Science and Technology Program (Youth Innovation Project) [浙江省医药卫生科技计划(青年创新项目), No.2023RC128].
Statement of Informed Consent
This research followed the ethical principles of medical research formulated in the World Medical Association Declaration of Helsinki.The study was approved by the Ethics Committee of Chun’an County Hospital of Traditional Chinese Medicine, Zhejiang Province(Approval No.2021002).Informed consent was obtained from the individual participants or their guardians.
Received: 26 February 2023/Accepted: 28 July 2023
猜你喜欢
杂志排行
Journal of Acupuncture and Tuina Science的其它文章
- Efficacy of electroacupuncture on the recovery of gastrointestinal function after laparoscopic cholecystectomy: a systematic review
- Fascia is the “sensor” for the coupling response of manipulative therapies
- Clinical study of electroacupuncture improving sleep electroencephalogram and event-related potential in patients with somatoform disorders
- Clinical observation of kidney-tonifying and mindcalming acupuncture therapy in the treatment of perimenopausal insomnia
- Effects of warming triple needling plus Chinese medication on inflammatory responses and daily functioning ability in knee osteoarthritis patients
- Clinical study of electroacupuncture combined with exercise therapy in improving the balance function of patients with knee osteoarthritis