Two different autorefractors for vision screening in children and adolescents
2024-02-23XiaoJunChenLinJieLiuBingSunDanDanJiangShuShuZuoYanHuiWangChunHuaZhangYanYanChen
Xiao-Jun Chen, Lin-Jie Liu, Bing Sun, Dan-Dan Jiang, Shu-Shu Zuo, Yan-Hui Wang,Chun-Hua Zhang, Yan-Yan Chen
1School of Optometry and Ophthalmology, Wenzhou Medical University, Wenzhou 325027, Zhejiang Province, China
2National Clinical Research Center for Ocular Diseases,Eye Hospital, Wenzhou Medical University, Wenzhou 325027,Zhejiang Province, China
Abstract
● KEYWORDS: refractive error; autorefractors; school-age myopia children
INTRODUCTION
Myopia, alternatively referred to as short-sightedness or near-sightedness, is a prevalent condition often initiating during childhood.It is conventionally defined as a spherical equivalent (SE) of ≤-0.5 D.Globally, myopia poses a major threat to the eye health of young people[1].According to the World Report on Vision published by the WHO[2], 2.6 billion people worldwide are myopic, 312 million of whom are children under 19 years of age.The prevalence of myopia is relatively high in Southeast Asia (approximately 23%-31% for children and adolescents in Europe and the U.S.and 47%-62%for children and adolescents in Southeast Asia).According to the National Health Commission Report, in 2020, the overall myopia rate for children and adolescents in China was 52.7%[3].
The high rate of myopia among Chinese children and adolescents has long been a matter of active concern for parents, schools and the state.A 2021 policy mandated regular vision screening for Chinese students using noncycloplegic and uncorrected methods[4].Noncycloplegic autorefraction inevitably overestimates myopia and underestimates hyperopia, particularly in children with strong accommodative reserve[5].Although cycloplegic autorefractor refraction is considered the gold standard for epidemiological assessment of refractive errors in children, there are numerous limitations to this approach, such as parental informed consent, the time required for cycloplegia, ocular discomfort, inconvenience,and additional costs[6-7].Cycloplegia autorefraction cannot be performed due to the limitations of the school learning environment.In contrast, a study by Thornet al[8]confirmed that noncycloplegic autorefraction combined with uncorrected visual acuity is popular for school screening; this approach may improve the sensitivity of noncycloplegic autorefraction in screening and further referral.A study by Maet al[9]confirmed that noncycloplegic autorefraction screening is quite accurate and reproducible, and it is fast and rarely requires child cooperation.Screening children with a noncycloplegic autorefraction technique is therefore important.More than one autorefractor is sometimes used in a single study, particularly in multicenter studies, long-term follow-up, or large-scale vision screening[10].Consistency and accuracy between instruments can help clinicians and researchers trust the results of a study.
The universality of vision screening[4]and the diversity of autorefractors[9]indicate that it is necessary to evaluate the consistency of instruments, which can not only compare data across different studies but also mix them in the same study.This is of great significance for long-term monitoring and dynamic assessment of children’s myopia.
SUBJECTS AND METHODS
Ethical ApprovalThis study adhered to the ethical principles,regulations, and the Helsinki Declaration, with approval number: 2022-117-K-89-01 from the Ethics Committee of the Ophthalmology Hospital at Wenzhou Medical University.Written informed consent was obtained from at least one parent or legal guardian for each participant.
SubjectsThe refractive data without cycloplegia were collected in May 2022 from patients with refractive errors in the optometry outpatient clinic of the Eye Hospital of Wenzhou Medical University.As both eyes have a strong correlation(P=0.83 for Tianle,P=0.81 for Topcon), only right eyes were enrolled in the analyses to avoid artificially narrowing the confidence intervals near the consistency limit[11].
Only children and adolescents under 18 years of age were included in our study.Before measurement, subjects with manifest strabismus, contact lenses (orthokeratology), a history of eye trauma or surgery, and poor cooperation were omitted by the triage nurse of the optometric clinic.All subjects underwent refraction using two autorefractors (Tianle RM-9000 and Topcon KR-800) in random order without cycloplegia by the same examiner following the same procedure in the whole automatic optometry process to reduce examiner bias.Automatic measurement mode was generally used unless the child’s cooperation was poor and manual measurement wasneeded (Table 1).Automatic fogging control adjustment was used for refraction, and it was read by blurring the target to relax the accommodation.The right eye was examined first,then the left eye.Refractive errors [spherical diopters (DS),cylinder diopters (DC), axis (A)] were measured three times in each eye.If any two measurements of one instrument differed by more than 0.50 D, another set of three consecutive measurements was required until the difference between any two measurements within a group was less than 0.50 D.Currently, many studies suggest ±0.50 D as the acceptable error range for clinically reliable refractive measurements to avoid poor measurements caused by overaccommodation or underaccommodation in the measurement process of children[12-14].

Table 1 Comparison of measuring parameters of Tianle RM-9000 and Topcon KR-800
Parameters and DefinitionsWe used power vectors (Thiboset al[11]) to express clinical measurements: SE=DS+DC/2;J0=-DC/2×cos(2A); J45=-DC/2×sin(2A), where DS is sphere,DC is cylinder and Ais axis.J0and J45represent horizontal/vertical and oblique astigmatism, respectively.
We defined refractive errors based on noncycloplegic measurements: myopia (SE ≤-0.50 D) was categorized as mild(-0.50 to -2.99 D), moderate (-3.00 to -5.99 D) or high (≤-6.00 D);hyperopia (SE ≥+0.50 D) was categorized as mild (+0.50 to+1.99 D) or mild-to-high (≥+2.00 D); astigmatism (cylinder≤-0.75 D) was categorized as low (-0.75 to -2.99 D) or high(≤-3.00 D); and emmetropia was defined as a measurement ranging from -0.5 to +0.5 D[15].
Statistical AnalysisWe used Epidata 3.1 to create a database and entered data by two researchers independently and in duplicate.We divided subjects into three age groups: 4-8y,9-13y, and 14-18y.We used parametric tests to compare SE,DS, DC, J0andJ45between and within groups and calculated the difference as Tianle minus Topcon.We assessed the correlation and agreement of the two autorefractors by Spearman correlation analysis, Bland-Altman plots, and intraclass correlation coefficients (ICC) analysis[16-17].We analyzed the distribution and diagnostic capacity of refractive errors by the Chi-square test.We used univariate and multiple linear regression to examine the factors associated with SE differences.We estimated the proportion of individuals with significant differences (≥0.50 D myopic shift in SE)and explored the related factors by logistic regression.We calculated and classified axis differences and analyzed the distribution of eyes with cylinder power ≤-0.50 or -0.75 D on both autorefractors.We used IBM SPSS 26.0 and MedCalc 18.2.1 for statistical analyses, andP<0.05 indicated statistical significance.

Figure 1 Distribution of the refractive errors measured by Tianle RM-9000 (A-C) and Topcon KR-800 (D-F).
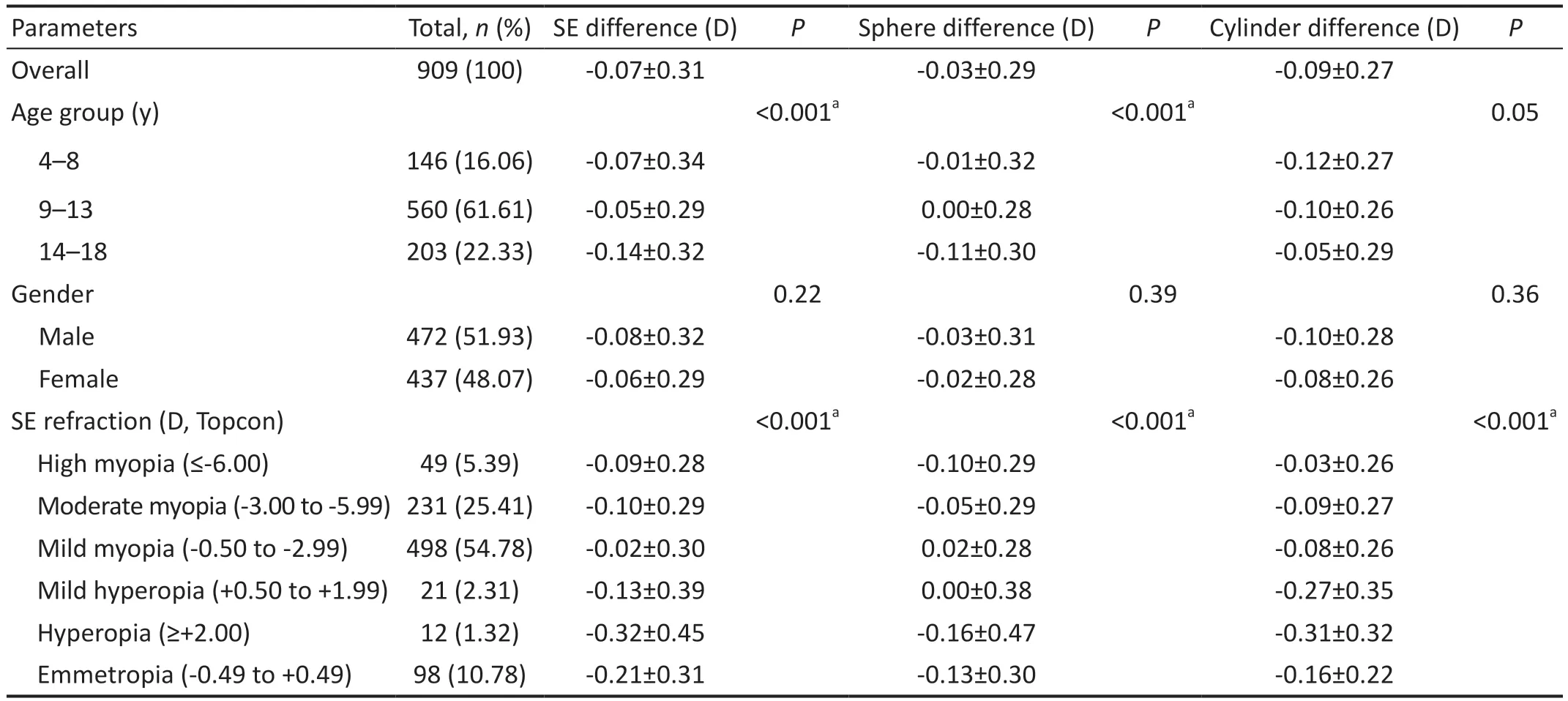
Table 2 Differences in the refractive measurements by demographic groups between Tianle RM-9000 and Topcon KR-800 mean±SD
RESULTS
Differences by Demographics and Refractive ErrorThis study included 909 subjects aged 4 to 18y (mean: 11.35±2.94;median: 11.19), with 437 females (48.07%).They were divided into three age groups: 4-8y (n=146), 9-13 (n=560),and 14-18y (n=203; Table 2).Figure 1 shows the distribution of refractive errors (SE, sphere, and cylinder) measured by the Tianle RM-9000 and Topcon KR-800 for 909 eyes.All parameters were nonnormally distributed and skewed toward myopia.Table 2 shows the differences in refractive components between the two autorefractors by age and refractive error groups.Refractive error groups had significant effects on SE,DS, and DC differences.Age group had significant effects on SE and DS differences but not on DC differences.Gender had no effect on any difference.
Correlations and Differences Between the Two AutorefractionsTable 3 compares the noncycloplegicautorefraction measurements of Tianle RM-9000 and Topcon KR-800.The two devices had significant differences in SE,DS, and DC (allP<0.001) but not in J0and J45(P=0.43 andP=0.85, respectively).

Table 3 Comparison of the non-cycloplegic refraction measured by Tianle RM-9000 and Topcon KR-800 mean±SD
Correlation analysis showed high correlations and agreements in SE, DS, and DC between Tianle and Topcon, withRand ICC values of 0.98 and 0.99, 0.98 and 0.99, and 0.83 and 0.93,respectively.However, J0and J45had low correlations and agreements (R=-0.004 and -0.034; both ICC<0.10).There was no clear relation between the J0and J45differences of the two autorefractors.
Comparison of Cylindrical AxesThe consistency of the cylindrical axes can be observed in Table 4.When eyes with a cylinder ≤-0.50 D were included in the result analysis, the mean (SD) axial difference was 0.72° (SD: 11.33°), and the axial differences of 73.78% (743/1007) of eyes were within±10°.
Factors Associated with Significant DifferencesMultiple linear regression results showed that older age was associated with a lower SE difference (B: -0.013; 95%CI: -0.021 to-0.006).Gender and SE (Topcon KR-800, D) did not have a significant effect on the SE difference (Table 5).In a logistic regression model adjusted for age group, gender, refractive error type and magnitude, age group and gender were not significant factors for having at least a 0.50 D myopic SE difference (P=0.072, 0.063, respectively).However, this difference was less likely in those with moderate [odds ratio(OR): 0.32, 95%CI: 0.15-0.68] or mild myopia (OR: 0.43,95%CI: 0.23-0.81; Table 6).
Mean Differences, 95% LoA, and Proportions Within±0.50 DTable 7 shows the mean differences (SD) and 95%LoA in SE, DS, DC, J0and J45between Tianle and Topcon.The mean differences in SE, DS and DC were not zero (P<0.05 for all).For SE, DS and DC, the maximum absolute differences within the 95% LoA were 0.63 D, 0.50 D and 0.62 D,respectively.For J0and J45, the minimum absolute differences within the 95% LoA were 1.07 D and 0.97 D, respectively.The proportions of the absolute differences within ±0.50 D were high for SE (90.54%), DS (94.83%) and DC (93.84%) but lower for J0(81.52%) and J45(82.62%; Figure 2).
Subgroup analysis across age groupsFigures 3-5 compare SE, DC, DS,J0andJ45between Tianle RM-9000 and TopconKR-800 by age group.At 4-8-year-olds (Figure 3), SE and DC had significant mean differences of -0.07 and -0.12 D (P<0.05),while DS had no significant mean difference of -0.009 D(P>0.05).The 95% LoAs of SE, DC and DS were -0.73 to 0.59,-0.64 to 0.41, and -0.63 to 0.61, respectively.At 9-13-yearolds (Figure 4), SE and DC had significant mean differences of -0.048 and -0.10 D (P<0.05), while DS had no significant mean difference of 0.0014 D (P>0.05).The 95% LoAs of SE,DC and DS were -0.63 to 0.53, -0.61 to 0.41, and -0.54 to 0.55,respectively.At 14-18-year-olds (Figure 5), SE, DC and DS had significant mean differences of -0.14, -0.052 and -0.11 D,respectively (P<0.05).The 95% LoAs of SE, DC and DS were-0.76 to 0.48, -0.63 to 0.52, and -0.71 to 0.48, respectively.J0andJ45had no significant mean differences close to 0 (P>0.05)in all age groups, with similar ranges of 95% LoA.

Table 4 Comparison of cylindrical axes measured by Tianle RM-9000 and Topcon KR-800 n (%)

Table 5 Multivariate linear regression analysis of the association of the SE difference between Tianle RM-9000 and Topcon KR-800

Table 6 Factors associated with at least 0.50 D of more myopic SE

Figure 2 Bland-Altman plots of the differences between Tianle and Topcon for 4-18-year-olds Solid line represents the mean of the differences, dotted line indicates zero, long dotted line indicates the corresponding 95% limit of agreement (LoA), and solid line of “H”type shows the 95%CI of LoA.A: Spherical equivalent; B: Sphere diopter; C: Cylinder diopter; D: J0; E: J45.

Figure 3 Bland-Altman plots of the differences between Tianle and Topcon for 4-8-year-olds Solid line represents the mean of the differences, dotted line indicates zero, long dotted line indicates the corresponding 95% limit of agreement (LoA), and solid line of “H”type shows the 95%CI of LoA.A: Spherical equivalent; B: Sphere diopter; C: Cylinder diopter; D: J0; E: J45.

Figure 4 Bland-Altman plots of the differences between Tianle and Topcon for 9-13-year-olds Solid line represents the mean of the differences, dotted line indicates zero, long dotted line indicates the corresponding 95% limit of agreement (LoA), and solid line of “H”type shows the 95%CI of LoA.A: Spherical equivalent; B: Sphere diopter; C: Cylinder diopter; D: J0; E: J45.

Figure 5 Bland-Altman plots of the differences between Tianle and Topcon for 14-18-year-olds Solid line represents the mean of the differences, dotted line indicates zero, long dotted line indicates the corresponding 95% limit of agreement (LoA),and solid line of “H”type shows the 95%CI of LoA.A: Spherical equivalent; B: Sphere diopter; C: Cylinder diopter; D: J0; E: J45.

Table 7 Meand and corresponding 95% LoA of refractive errors measured by Tianle RM-9000 and Topcon KR-800
Agreement in Prevalence RatesThe prevalence rates presented here were used as another measure of comparison but not to reflect the prevalence rates of the population in our city or the examined ethnicity.According to the Chi-square test results, there was no difference in the distribution of refractive error between Topcon and Tianle.The prevalence rates of myopia in the examined population calculated using Tianle and Topcon were 86.47% and 85.59%, respectively, and those of hyperopia were 3.41% and 3.63% (χ2test,P=0.68).However,the differences in the prevalence rates of astigmatism were significant (χ2test,P=0.011; Table 8).
DISCUSSION
In our study involving 909 school-age Chinese children and adolescents, we assessed the difference in refractive results obtained from two autorefractors, namely the Tianle RM-9000 and Topcon KR-800.Our findings indicate a high level of consistency between the two autorefractors, as the differences in SE, DS, and DC fell within clinically acceptable ranges.These results suggest that the Tianle RM-9000 and Topcon KR-800 can be employed interchangeably for vision screening or research purposes in 4- to 18-year-old children and adolescents.Compared to previous similar studies[12],the innovation of this research lies in the utilization of a larger sample size.The comparison of two autorefractors was approached from the perspective of school-based screening,meeting the demand for establishing refractive profiles for adolescents.
The sphere, cylinder, and SE between Topcon KR-800 and Tianle RM-9000 showed negative deviations, suggesting that Topcon relaxed accommodation more than Tianle under the same conditions.Although both autorefractors had similar optometry principles with internal fixed targets, infrared light sources, and automatic fogging systems, their fogging images were different: Topcon used a red house, while Tianle used a hot air balloon[18].This might affect the accuracy of the surface accommodative response, which depends on stimulus characteristics such as brightness, contrast, and color[19].Other possible factors contributing to the differences include the inadequate control of accommodation by the automatic fogging system in young hyperopic participants[20]and the changes in accommodation levels during the examination, such as attention and accommodation lag in myopic children[21].In previous studies, we found a mean difference between instruments of -0.12 D.This difference was larger than the 0.072 D difference we calculated in our study, which was similarly larger than that reported in Xionget al’s[22]study for Nidek ARKA-510A and Topcon KR-8900 (0.07±0.26 D,95%CI: -0.44 to 0.57).In contrast, Jinet al[18]reported that Tianle RM-9000 was more hyperopic by 0.44 D than Topcon RM-8900, which could not be used interchangeably in Chinese children aged 6-16y without corrections.
The age and refractive error had a large influence on the SE measurement bias between the Tianle RM-9000 and Topcon KR-800.Lower SE differences (<0.5 D) were more common in less myopic subjects.The overall SE difference was larger in younger individuals, which supported existing evidence[15].However, the SE difference decreased with increasing age.This could be due to the age-related decrease in accommodation.The higher proportion of mild and moderate myopia in the younger population may explain the lower SE differences in this group[22].These findings suggest that age and refractive error are important factors to consider when comparing SE measurements from different instruments.
The mean differences of SE and DC were not zero in all three age groups, and they all showed negative deviations (Tianle minus Topcon), which matched the overall analysis that Topcon could relax accommodation more.However, in the 14-to 18-year-old group, these differences were less than -0.1 (bothP<0.05), and the lower limits of 95% LoA were both less than-0.70.The study[18]suggested that myopic bias was related to age and refractive error, and larger SE differences were more common in subjects with higher myopia.The 14- to 18-yearold group had 3.8- to 4.5-fold more subjects with high myopia than the 9- to 13-year-old group.There were no subjects with high myopia in the 4- to 8-year-old group.This could explain why older subjects had larger DS differences,which might be due to the higher prevalence of high myopia,offsetting the reduced accommodation from older age[23];another reason was that highly myopic eyes might have ocular shape changes, which could increase the self-refraction error significantly[24].
For J0andJ45, the two autorefractions had near 0 mean difference (P=0.43, 0.84) and 1.00-D consistency range, similar to Jinet al’s[18]study.However, Linet al[25]found narrower agreement limits between VX120 and Topcon KR-800 for these components.The absolute differences within ±0.50 D were lower for J0(81.52%) and J45(82.62%), which many studies said was the acceptable error range for the minimum refractive results[12-14].This pattern underscores their unreliability as effective measures for assessing astigmatism.For axial differences, the percentage within ±10° was 73.78% in eyes with a cylinder ≤-0.50 D.The findings revealed a significant difference in the cylinder axis, surpassing 10 degrees in about 25% of eyes.This suggests that, for one in every four patients,the variance in cylinder axis extends beyond the clinically acceptable threshold.
Tianle RM-9000 and Topcon KR-800 agreed well in DC and myopia and hyperopia prevalence but poorly in J0and J45components and astigmatism prevalence.These results are important for astigmatism diagnosis and treatment and provide a reference for more instrument comparisons.This inconsistency with previous studies[25]could be due to the different measurement principles and algorithms of the two instruments[26].The measurement consistency and repeatability might have been affected by some errors or biases, such as tear film instability,instrument alignment, and participant response[27].
Our study has some limitations.First, the lack of cycloplegia autorefraction does not stop some accommodation and convergence, which may bias the measurements to more myopia.However, the autorefraction compared in this study was mainly for vision screening or progression studies in school-aged children, not for clinical optometry.Second, the study only tested two types of autorefraction instruments;thus, the findings may not apply to other instruments.Third,our findings may only suit 4- to 18-year-old children and adolescents in China and not other ages or ethnicities.Last, our results mostly focused on myopia and few hyperopia patients,and more hyperopia patients are needed later to improve the research reliability.
In conclusion, Tianle RM-9000 measures more myopic SE,DS, and DC than Topcon KR-800, but both autorefractors are clinically acceptable.The refractive difference grows with younger age and higher myopia.However, J0and J45are less consistent, and the axial difference varies greatly in low astigmatism eyes.We advise that clinicians and researchers should be careful when using instruments to measure astigmatism, especially in low astigmatism eyes.Overall,Tianle RM-9000, as a domestic brand, matches well with the more commonly used Topcon KR-800, which can be a valuable supplement to any optometry or ophthalmic practice that can use them together to estimate refractive error and track refractive development in children and adolescents.Readers can benefit from this because they can compare data measured by either device in different studies or make a data pool that both can analyze in the same study.
ACKNOWLEDGEMENTS
Authors’ contributions:Chen YY, Chen XJ, Liu LJ, and Sun B conceived and designed the experiments.Sun B,Jiang DD, Zuo SS, Wang YH and Zhang CH performed the experiments.Chen XJ and Liu LJ analyzed the data and wrote the paper.Chen YY revised the paper.All authors reviewed the manuscript and approved the final manuscript.
Foundation:Supported by the National Natural Science Foundation of China (No.81873683).
Conflicts of Interest: Chen XJ,None;Liu LJ,None;Sun B,None;Jiang DD,None;Zuo SS,None;Wang YH,None;Zhang CH,None;Chen YY,None.
杂志排行

International Journal of Ophthalmology的其它文章
- Using choroidal thickness to detect myopic macular degeneration
- lmpact of multifocal gas-permeable lens designs on short-term choroidal response, axial length, and retinal defocus profile
- Baerveldt glaucoma implant with Supramid© ripcord stent in neovascular glaucoma: a case series
- Efficacy and safety of Usights UC100 illuminated microcatheter in microcatheter-assisted trabeculotomy
- Quantifying peripapillary vessel density and retinal nerve fibre layer in type 1 diabetic children without clinically detectable retinopathy using OCTA
- Nomogram to predict severe retinopathy of prematurity in Southeast China