Systematic review and meta-analysis of endometrial thickening during endocrine therapy combined with Chinese herbal medicine intervention after breast cancer surgery
2023-12-29PANYuancanCHENDongWANGYueLUTaichengCHENXingMATingtingZHANGYiWANGXiaomin
PAN Yuan-can, CHEN Dong, WANG Yue, LU Tai-cheng, CHEN Xing, MA Ting-ting,ZHANG Yi, WANG Xiao-min✉
1.Beijing Traditional Chinese Medicine Hospital Affiliated to Capital Medical University, Beijing 100010, China
2.Beijing University of Chinese Medicine, Beijing 100029, China
Keywords:Postoperative breast cancer Endocrine therapy Chinese herbal medicine Thickening of the endometrium Meta-analysis
ABSTRACT
1.Introduction
At present, breast cancer is the most common malignant tumor in female tumor patients worldwide, accounting for about 24.5%of female malignant tumors, and accounting for about 15.5% of malignant tumor-related deaths[1, 2].The patient’s treatment regimen is a comprehensive treatment regimen that mainly involves surgical resection of the lesion and receives standardized endocrine therapy after surgery.Although surgery is a common clinical treatment for breast cancer patients, there is still a risk of recurrence in some patients[3].Patients with breast cancer have a higher overall 5-year survival rate, approximately 89%, but in the presence of metastasis,this survival rate drops to 25%[4]; Hongchao Pan’s[5] Studies have shown that the risk of recurrence in breast cancer patients is closely related to the initial T and N states of patients, and the risk of recurrence of T2N4-9 can be as high as 41%, and the life and health of patients with serious danger are serious; The application of endocrine drugs, commonly used drugs are estrogen antagonists and aromatase inhibitors, in the case of continuous treatment for 5 years,estrogen receptor (ER)-positive patients with early breast cancer can significantly reduce the recurrence rate during and after treatment;And endocrine therapy continued beyond 5 years can further reduce the risk of breast cancer recurrence, but it also produces additional adverse effects.The main mechanism of endocrine therapy to reduce the recurrence rate of tumor patients is to inhibit the growth of tumor cells and reduce the recurrence risk of tumor patients by regulating the endocrine hormone environment that is essential for the survival and development of tumor cells in the human body[6].At the same time, endocrine therapy will have adverse effects on the endometrium, endometrial thickening is one of the adverse effects,abnormal uterine bleeding is one of its clinical symptoms, which causes great trouble to women’s reproductive health and quality of life[7].The use of Chinese herbal medicine has a long and rich clinical experience in the treatment of endometrial thickening; A metaanalysis of the literature of randomized controlled trials (RCTs)of postoperative combination with Chinese herbal medicines for endometrial thickening during endocrine therapy for breast cancer is conducted to provide evidence-based medical evidence for the efficacy of Chinese herbal medicines in the treatment of endometrial thickening during endocrine therapy after breast cancer surgery.
2.Information and methodology
2.1 Data Sources
RCTs of endometrial thickening combined with Chinese herbal interventions during postoperative endocrine therapy for breast cancer.CBM, CNKI, Wanfang Data, Vipu.com, PubMed, Embase,Cochrane were searched.Chinese search formula: (breast tumor,OR, breast cancer, OR mamma, mammary rock, OR, breast cancer),AND (endocrine therapy), AND (endometrial OR, endometrial thickening, OR endometrial hyperplasia), AND (traditional Chinese medicine, OR, traditional Chinese medicine, OR, traditional medicine), AND (randomized controlled trial, OR, randomized OR controlled OR trial).English Search Formula: ((“Breast Neoplasms OR Breast Tumor OR Breast Cancer) AND (Endocrine therapy)AND(endometrium OR endometrial hyperplasia OR endometrial thickening) AND (Traditional Chinese Medicine OR Chinese Traditional Medicine OR Chinese Herbal Drugs OR Chinese Medicine Herb)AND (Random controlled trials OR random OR control OR trials).The search scope was established for databases up to January 2023.Literature is not limited to the type of publication,and the limited language is Chinese and English literature.
2.2 Inclusion criteria
(1) Study type: RCT of endometrial thickening during endocrine therapy after breast cancer surgery combined with Chinese herbal medicine; (2) Study subjects: patients with endometrial thickening during endocrine therapy after breast cancer surgery; (3)Intervention/control measures: the treatment group was Chinese herbal medicine combined with conventional endocrine therapy drugs, and the control group was conventional endocrine therapy drugs.
2.3 Exclusion Criteria
(1) Non-randomized controlled trials, such as individual cases,reviews, theoretical discussions, animal experiment literature, etc.;(2) duplicate literature; (3) Literature for which full text is not available; (4) literature that did not contain outcome measures and whose outcome measures were not relevant.
2.4 Outcome measures
Primary outcomes: endometrial thickness; Secondary outcomes were KPS score, modified Kupperman score, TCM clinical symptom score, CA153, CEA, FSH, E2.
2.5 Data screening and data extraction
One review author independently screened studies using Endnote software for inclusion and exclusion and extracted relevant data(age, sample size, interventions, outcome measures) from the studies, while another review reviewed the selected data.When two investigators disagree, a third investigator is required to participate in the discussion to reach a final conclusion.
2.6 Literature quality evaluation
Two review authors assessed the risk of bias for the methodological quality of RCTs in six domains: selection bias, performance bias, detection bias, attrition bias, reporting bias and other biases according to the ‘Risk of bias’ tool recommended by the Cochrane Collaboration.If there is disagreement, a third investigator needs to discuss and resolve it.
2.7 Data Analysis
3.Results
3.1 Literature search
Through the search of domestic and foreign databases, a total of 779 articles were obtained.Using the Revman 5.4 deduplication function, 110 duplicate articles could be excluded, 649 articles that did not meet the inclusion criteria could be excluded by reading the title and abstract, and 8 articles could be excluded after reading the full text, as follows: 1 duplicate publication, 2 unrelated outcome indicators, 2 non-randomized controlled experiments, 2 non-breast cancer postoperative articles, 1 full text could not be viewed, and finally 12 articles were selected for inclusion in this study, the process is shown in Figure 1.
3.2 Basic characteristics of the literature are included
Twelve RCTs[8-19] with a total of 710 patients were included in this review.The endpoint indicators used in the report mainly included endometrial thickness, improved Kupperman score total score, TCM clinical symptom score, KPS score status, CA153, CEA,FSH, E2.The basic characteristics of the included studies are shown in Table 1.

Tab1 Basic characteristics of the literature are included
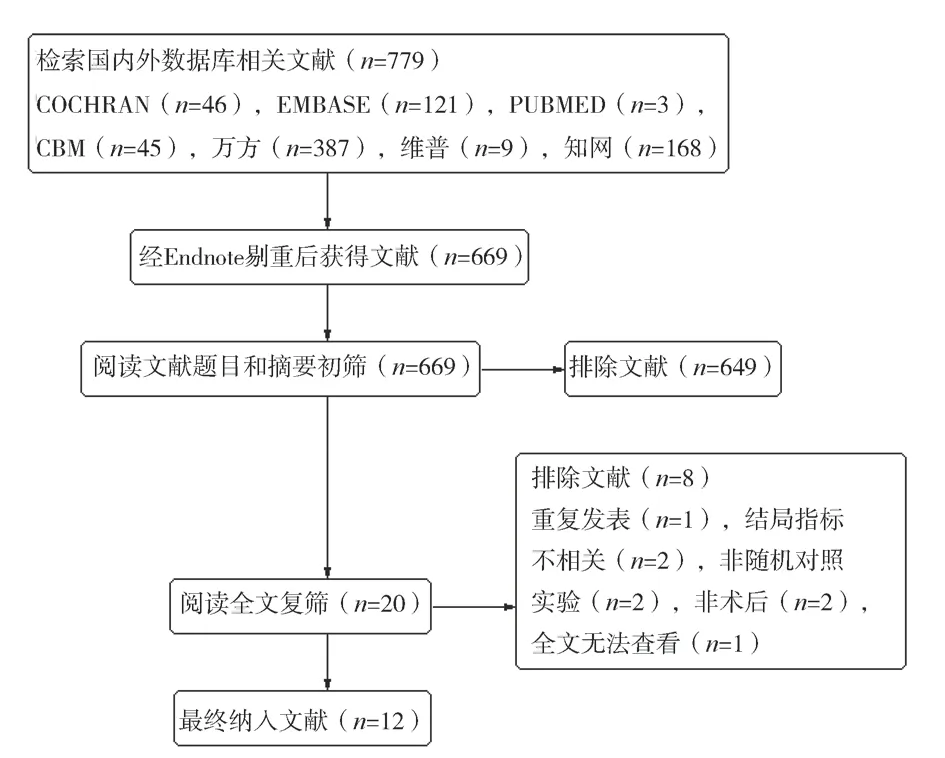
Fig 1 Flow chart of literature retrieval
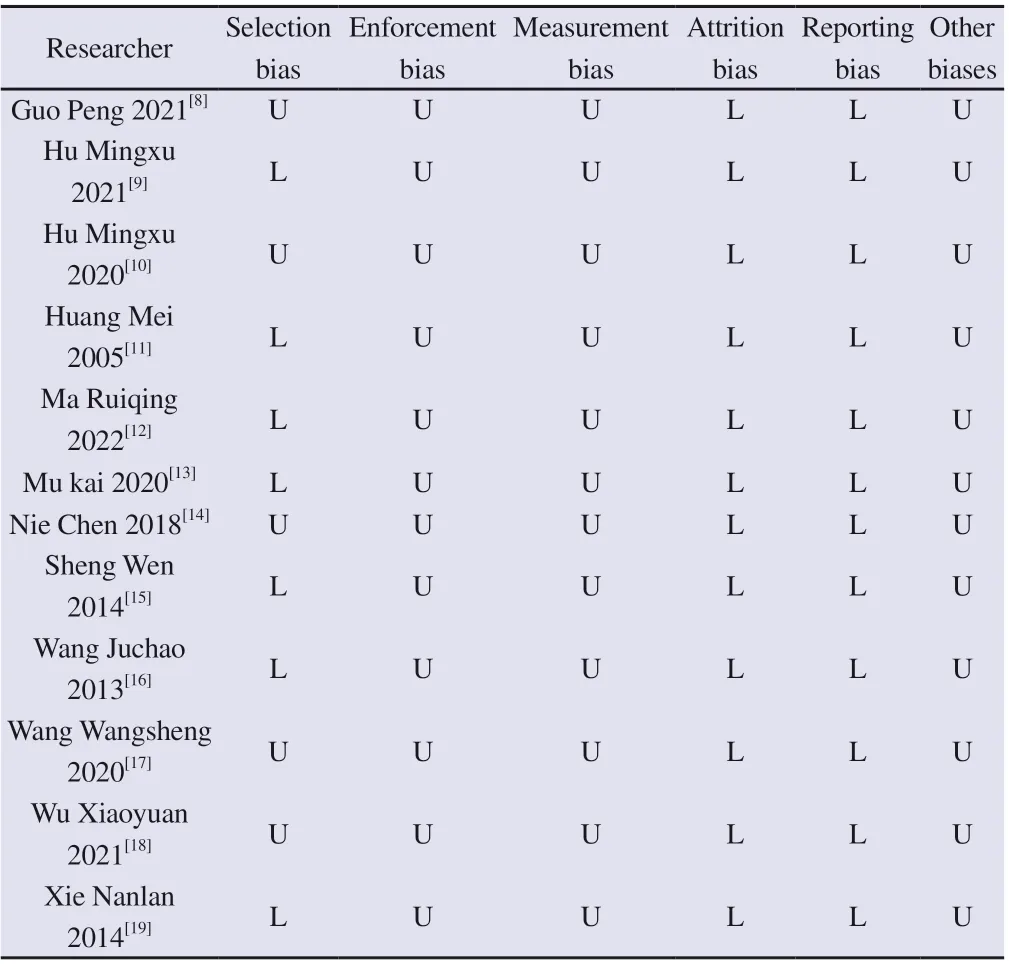
3.3 Literature quality evaluation was included
According to the Cochrane Collaboration Quality Assessment Tool, the possibility of bias cannot be completely excluded.The methodological quality of the included studies is shown in Table 2 and Figure 2.
3.4 Analysis of meta-results
Twelve RCTs were meta-analysed, of which four were statistically significant, including: endometrial thickness, improved Kupperman score, TCM clinical symptom score, KPS score; There were 4 items that were not statistically significant, including: CA153, CEA, FSH,and E2.
Tab2 Risk of bias assessment of included studies
Fig 2 Cochrane Risk of Bias Assessment Table
3.4.1 Endometrial thickness
3.4.1.1 3 months endometrial thickness
Seven studies reported endometrial thickness at 3 months, involving the following number of patients: total n=376, treatment group n=188, control group n=188.There was no significant heterogeneity between the two groups (P=0.61, I2=0%), and a fixed-effect model was used.ResultsAfter 3 months of treatment, the endometrial thickness in the treatment group was statistically significantly lower than that in the control group (MD=-1.12, 95% CI [-1.47 to -0.77],Z=6.27, P<0.00001).See Figure 3.
3.4.1.2 6 months endometrial thickness
Five studies reported endometrial thickness at 6 months, involving the following number of patients: total n=334, treatment group n=167, control group n=167.The results of heterogeneity test showed that there was statistical heterogeneity between the two groups (P=0.04, I2=60%), and after sensitivity analysis, it was found that the study of Huang Mei et al.[11] may be the source of heterogeneity.The results of sensitivity analysis showed that after 6 months of treatment, the endometrial thickness in the treatment group was lower than that in the control group, which was statistically significant (MD = -1.90, 95% CI [-2.38 to -1.42], Z =7.82, P < 0.00001).See Figure 4A.B.
3.4.1.3 12 months endometrial thickness
Two studies reported endometrial thickness at 12 months, involving the following number of patients: total n=124, treatment group n=62,control group n=62.There was no significant heterogeneity between the two groups (P=0.65, I2=0%), and a fixed-effect model was used.ResultsAfter 12 months of treatment, the endometrial thickness in the treatment group was statistically significantly lower than that in the control group (MD=-2.24, 95% CI [-2.96 to -1.52], Z=6.13,P<0.00001).See Figure 5.
3.4.2 Improved Kupperman score
Three studies reported the improved Kupperman score with the following number of patients: total n=166, treatment group n=83,control group n=83.Whether there was statistical heterogeneity between the two groups (P<0.1, I2=95%), a random-effects model was used.As a result, the modified Kupperman score in the treatment group was statistically significantly lower than that in the control group (MD=-10.45, 95% CI [-19.10 to -1.80], Z=2.37, P=0.02).See Figure 6.

Fig 3 Forest plot of endometrial thickness at 3 months
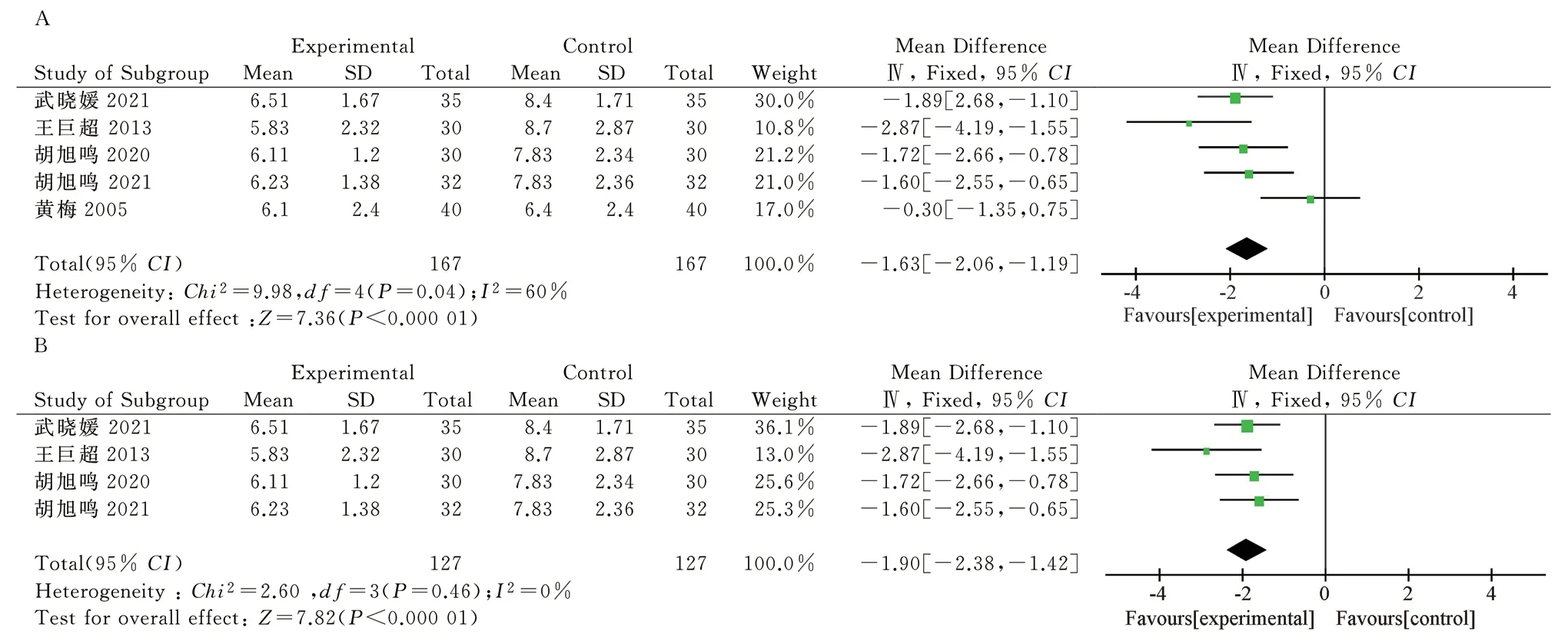
Fig 4 A.6-month endometrial thickness forest plot B.6-month endometrial thickness forest plot (sensitivity analysis)

Fig 5 Forest plot of endometrial thickness at 12 months

Figu 6 Improved Kupperman scoring forest chart
3.4.3 TCM clinical symptom points
Four articles reported the score of clinical symptoms of traditional Chinese medicine, and the number of patients involved was as follows: total n=210, treatment group n=105, control group n=105.There was no significant heterogeneity between the two groups(P=0.11, I2=50%), and a fixed-effect model was used.As a result,the clinical symptoms of patients were effectively relieved after the combination of Chinese herbal medicine (SMD=-1.53, 95% CI [-1.84 to -1.22], Z=9.58, P<0.00001).See Figure 7.

Fig 7 Integral forest diagram of clinical symptoms of traditional Chinese medicine
3.4.4 KPS Score Status Five studies reported KPS scores, involving the following number of patients: total n=286, treatment group n=143, control group n=143.There was no significant heterogeneity between the two groups (P=0.88, I2=0%), and a fixed-effect model was used.As a result, the KPS score of the patients after the treatment of Chinese herbal medicine was higher than that of the control group, which showed that it could effectively improve the health status of the patients (MD=3.75, 95% CI [2.81 to 4.68], Z=7.88, P<0.00001).See Figure 8.
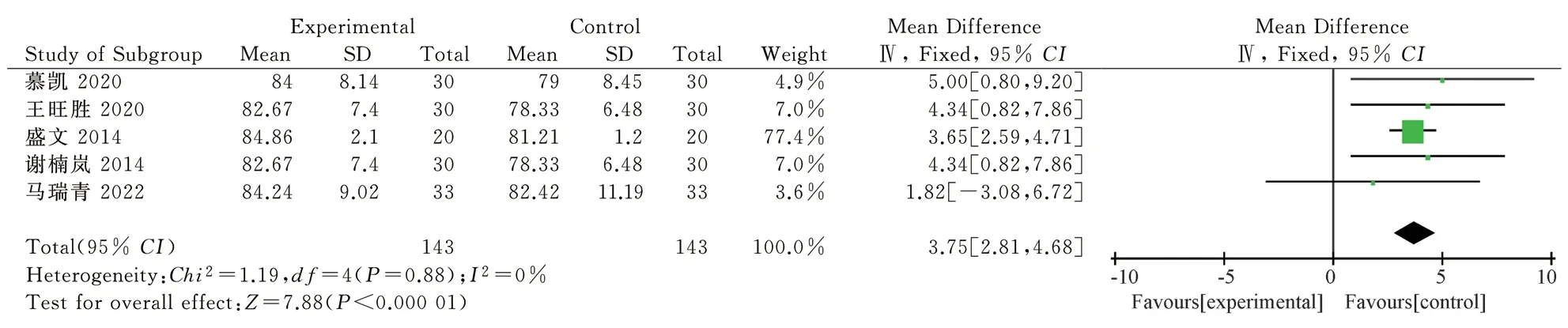
Fig 8 KPS scoring forest plot
3.4.5 CA153
Three articles reported the tumor marker CA153, involving the following number of patients: total n=166, treatment group n=83,control group n=83.There was no significant heterogeneity between the two groups (P=0.99, I2=0%), and a fixed-effect model was used.As a result, there was no statistically significant difference between the two groups (MD = -1.60, 95% CI [-4.10 to 0.91], Z = 1.25, P =0.21).See Figure 9.

Fig 9 CA153 forest diagram
3.4.6 CEA
Three articles reported the tumor marker CEA, involving the following number of patients: total n=166, treatment group n=83,control group n=83.There was no significant heterogeneity between the two groups (P=0.43, I2=0%), and a fixed-effect model was used.As a result, there was no statistically significant difference between the two groups (MD = 0.11, 95% CI [-0.37 to 0.59], Z = 0.45, P =0.65).See Figure 10.

Fig 10 CEA forest diagram
3.4.7 FSH
Two studies reported the FSH of sex hormones, and the number of patients involved was as follows: total n=100, treatment group n=50,control group n=50.There was no significant heterogeneity between the two groups (P=0.44, I2=0%), and a fixed-effect model was used.As a result, there was no statistically significant difference between the two groups (SMD = -0.06, 95% CI [-0.45 to 0.33], Z = 0.31, P =0.76).See Figure 11.

Fig 11 FSH forest diagram
3.4.8 E2
Two studies reported the situation of sex hormone E2, and the number of patients involved was as follows: total n=100, treatment group n=50, control group n=50.There was no significant heterogeneity between the two groups (P=0.47, I2=0%), and a fixed-effect model was used.As a result, there was no significant difference between the two groups (SMD=0.24, 95%CI -0.15 to 0.64], Z=1.21, P=0.22).See Figure 12.

Fig 12 E2 forest diagram
3.5 Analysis of publication bias
3-month endometrial thickness literature inverted funnel using Revman 5.4, see Figure 13.Render incomplete symmetry in this funnel; Suggested possible publication bias.The low number of included literature may have contributed to this bias.

Fig 13 3-month endometrial thickness funnel diagram
4.Discussion
During endocrine therapy after breast cancer surgery, endometrial thickening is one of the common adverse reactions, which greatly affects the quality of life of patients, and a small number of patients have the risk of malignant endometrial transformation, threatening the life and health of patients[20].The use of endocrine therapy drugs can lead to excessive endometrial hyperplasia, endometrial thickening belongs to the category of “leakage” in traditional Chinese medicine,and there are countless discussions among traditional Chinese medicine practitioners, “Jingyue Quanshu Women’s Rule” cloud:“Leakage continues, and the chaos is even worse”[21], describe its possible pathogenesis; “Medical Sect Jinjian Gynecological Heart Method Essentials”: “After a woman goes through the process, she does not stop dripping, and her name leaks from the day.Menstrual blood suddenly fell into a big way, called meridian collapse”[22] ,describing its different clinical manifestations; To summarize its pathogenesis, it can be described as impulse injury, unfavorable meridians, uterine stasis, poor qi and blood, accumulation of sputum,and thickening of the endometrium, resulting in menstrual period,menstrual flow disorders and other gynecological diseases[23, 24].Chinese herbal medicine has a long history of treating endometrial thickening, or “leakage”, and “Thousand Golden Wings” says that thistle root wine can “cure women’s collapse and remove blood”[25];The Pulse Sutra says: “The pulse of the mouth is large...The woman is half-born and leaks, and the soup is the master.”[26] , which can be seen in detail introduces the use of Chinese herbal medicine to solve the actual clinical problems of patients.Modern studies have shown that the main reason for endometrial hyperplasia and thickening is the long-term lack of antagonistic estrogen progesterone in the body,resulting in the inability of the endometrium to undergo periodic exfoliation and bleeding, and is closely related to hypothalamicpituitary-ovarian axis (HPOA) dysfunction[27, 28] ; There are studies[29] indicateAngelica can regulate HPOA through the tumor metastasis inhibitor gene Kisspeptin/G protein-coupled receptor 54(GPR54) system, thereby regulating the secretion of estradiol and progesterone.Modern medicine to prevent endometrial thickening includes oral progestogen, but long-term use of progestogen can produce additional adverse effects, including abnormal liver and kidney function, obesity and increased risk of breast lesions[30] ;Although the levonorgestrel intrauterine extended-release system can obtain certain efficacy, it has a high dropout rate and causes guttate bleeding in the vagina[31]; Repeated curettage, uterine removal and other surgical treatment options, the acceptance of patients is generally not high; The use of Chinese herbal medicine can avoid the occurrence of adverse reactions, reduce the trauma to patients, and at the same time improve the relevant clinical symptoms of patients,improve the quality of life of patients, and be more acceptable to patients.
Therefore, the effect of Chinese herbal medicines in the treatment of endocrine thickening during breast cancer surgery was summarized and evaluated, in order to provide a strong evidence-based medical basis for the use of Chinese herbal medicines for this condition.This study showed that after 3, 6 and 12 months of standardized Chinese herbal medicine treatment, ultrasound tests showed that Chinese herbal medicines could significantly improve the degree of endometrial thickening.Shan Haiyan[32] Studies have also shown that Chinese medicine motherwort can improve the thickness of the endometrium in patients, and there are no adverse reactions in the patients involved; Qin Chengxia[33] Studies have also shown that Poria Guizhi capsules have the effect of activating blood, removing stasis and eliminating accumulation, and can reduce the thickness of endometrial thickening.At the same time, it can reduce the modified Kupperman score, an internationally used tool to evaluate menopausal symptoms in patients, involving the most common perimenopausal symptoms such as night sweats, fatigue, and emotional agitation, and evaluate by assigning symptoms to points,and the higher the score, the more severe the menopausal symptoms[34], The results showed that the use of Chinese herbal medicine had obvious improvement effect; KPS score is a commonly used tool in clinical practice to evaluate the functional status of malignant tumor patients, and cancer patients with KPS scores ranging from 60 to 100 are generally considered suitable for standard cancer treatment or clinical trials, suggesting that the body can accept certain adverse reactions and side effects accompanied by certain treatments[35],The results showed that the use of Chinese herbal medicine had obvious improvement effect; KPS score is a commonly used tool in clinical practice to evaluate the functional status of malignant tumor patients, and cancer patients with KPS scores ranging from 60 to 100 are generally considered suitable for standard cancer treatment or clinical trials, suggesting that the body can accept certain adverse reactions and side effects accompanied by certain treatments[36]、Studies such as Du Kexin[37] shows that Chinese herbal medicine can play a role in reducing tumor markers;Huo Chaoyue[38]、Li Zhaopin[39]、Zhang Li[40] have shown that Chinese herbal medicine can effectively regulate the level of sex hormones; This result may be closely related to the small number of included articles and small sample sizes.
Limitations and shortcomings of this study: 1.The total sample size of the 12 RCTs included in this study was small, involving 710 patients; 2.Some outcome indicators, such as FSH, E2,were included in the literature, which may lead to differences in the final outcome; 3.Some of the included literature may have methodological design flaws, particularly in the use of blinding.
ConclusionsIt is necessary to include higher quality and large sample RCTs for demonstration, and combine Chinese herbal medicines in the process of postoperative endocrine therapy for breast cancer to observe the effect of intervention on endometrial thickening, so as to provide evidence-based medical support for better prevention of endometrial thickening in the process of endocrine therapy.
Authors’ Contribution and Conflict of Interest Pan Yuancan and Chen Dong were responsible for the idea of the article and writing the paper, and Wang Yue, Chen Xing and Lu Taicheng collected the literature related to the research content and completed the screening work.Ma Tingting and Zhang Yi conducted statistical analysis of the article; Corresponding author Wang Xiaomin is responsible for the idea and final review of the article.There is no conflict of interest associated with the author of the content of the article.
杂志排行

Journal of Hainan Medical College的其它文章
- Clinical observation on the efficacy and safety of different doses of alfentanil for painless gastroscopy
- Expression and significance of ADAM12 in bladder cancer
- Effects of intravenous infusion of esketamine on analgesia and postpartum antidepressant after cesarean section
- The expression of TUSC3 in Preeclampsia and the function in trophoblast cell
- Effect of hepatocyte growth factor on inflammatory factors associated with CCL4-induced hepatocyte injury
- Inhibitory effect of water soluble propolis on oxidative damage in rats with ulcerative colitis