Calcitriol induced hypercalcemia -a rare phenomenon in lung cancer: A case report
2023-12-18AmulyaPrakashFarhanKhalidAhmadAlalwanHusamBaderDoantrangDuTrishalaMeghal
Amulya Prakash,Farhan Khalid,Ahmad Alalwan,Husam Bader,Doantrang Du,Trishala Meghal
Abstract BACKGROUND Calcitriol-induced hypercalcemia has been rarely reported in cases of lung cancer;however,it is frequently reported in cases of lymphoid malignancy and granulomatous disease.We present a rare case of hypercalcemia associated with squamous cell cancer of the lung with elevated calcitriol level.CASE SUMMARY A 61-year-old Caucasian female with severe hypercalcemia of 15 mg/dL,which led to a new diagnosis of metastatic lung cancer.Since the parathyroid hormonerelated peptide (PTHrP) level was minimally elevated at 2.1 pmol/L,we believe excessive calcitriol production by tumor cells was the underlying mechanism for hypercalcemia.Calcitriol was significantly elevated at 130 pg/mL with a low 25-hydroxyvitamin D level of 25.9 ng/mL and suppressed PTH level of 8 pg/mL.Corticosteroids are generally used to treat calcitriol-induced hypercalcemia,but we successfully treated our patient with bisphosphonate,highlighting the further utility of bisphosphonates in hypercalcemia treatment.CONCLUSION We believe that the underlying cause of hypercalcemia,in this case of metastatic squamous cell lung carcinoma,was elevated calcitriol,which was likely produced by the tumor cells.In addition to PTHrP,calcitriol levels should be included in the workup for hypercalcemia in cases of lung cancer.However,the pathophysiology and prognostic significance of dysregulated calcitriol production in solid tumors remain unclear and warrant further research.Bisphosphonate may be used as a steroid-sparing therapy even in cases of calcitriol-induced hypercalcemia and warrants further investigation.
Key Words: Hypercalcemia associated malignancy; Lung cancer; Denosumab; Calcitriol; Vitamin D; Case report
INTRODUCTION
Hypercalcemia associated with malignancy (HAM) is a common clinical finding and may even present as an oncologic emergency.It has been found in up to 30% of cases of malignancy[1].The estimated yearly prevalence of hypercalcemia for all cancers is 1.46% to 2.74%[2].Calcitriol overproduction is a rare etiology of HAM and accounts for merely 1% of cases of HAM[3].It has been frequently reported in cases of Hodgkin and non-Hodgkin lymphoma and also in some cases of ovarian dysgerminoma,pancreatic neuroendocrine tumors,seminomas,and renal cell carcinoma[4-6].In our extensive literature search,we came across just one case report of squamous cell lung cancer by Akaiet al[7],where calcitriol overproduction was exclusively responsible for hypercalcemia and treated with tumor resection.We present a rare case of squamous cell lung carcinoma with hypercalcemia and elevated calcitriol levels,which was treated successfully with bisphosphonate.To the best of our knowledge,bisphosphonates have never been reported for the treatment of calcitriol-induced hypercalcemia in the case of squamous cell lung carcinoma.
CASE PRESENTATION
Chief complaints
Hypercalcemia on routine blood work investigation.
History of present illness
The patient didn’t complain of any significant symptoms at the time of presentation.However,during detailed history taking,she reported vague complaints of nausea,fatigue,and generalized weakness but denied any other symptoms like constipation,palpitation,confusion,etc.
History of past illness
She has a past medical history of diabetes,hyperlipidemia,and depression.
Personal and family history
The patient has a remote history of tobacco smoking more than 15 years ago.She denies any supplementation with vitamin A,vitamin D,or calcium,frequent use of antacids,or excessive consumption of dairy products.Her current medications include atorvastatin and sertraline.Patient denies any significant family history.
Physical examination
Her vital signs and physical exam were within normal limits.
Laboratory examinations
Three months prior to the presentation,her calcium level was noted to be within the normal range of 10.1 (range: 8.6-10.3 mg/dL).In a routine lab work performed one week before the presentation,her corrected serum calcium was noted to be elevated first time at 13 mg/dL.She was asymptomatic at that point so decision was made to monitor with serial labs.
Our patient presented for repeat lab draw a week later and now her corrected serum calcium was 14.3 mg/dL,so she was instructed to visit the emergency department for further evaluation.She was admitted 12 h later on the same day and her corrected serum calcium further worsened to 15 mg/dL with an ionized calcium value of 7.5 mg/dL (range: 4.5-5.6).Her albumin was 3.4 mg/dL,creatinine 0.5 mg/dL,estimated glomerular filtration rate >60 mL/min/1.73 m2,magnesium 1.9 mg/dL (range: 1.8-2.4),phosphorus 2.4 mg/dL (range: 2.5-4.9).25-hydroxyvitamin D was noted to be low: 25.9 ng/mL(30-100 ng/mL),with elevated calcitriol level: 130 pg/mL (24.8-81.5 pg/mL) and suppressed intact parathyroid hormone(PTH) level: 8 pg/mL (15-65 pg/mL) and minimally elevated PTH-related peptide (PTHrP) 2.1 pmol/L (normal <2.0 pmol/L).Complete blood count and urinalysis were within normal limits.
Imaging examinations
Chest X-ray reveals a left hilar opacity,which was concerning for lung neoplasm.Upon further investigation with contrasted pan-computed tomography,the patient was noted to have a left lower lobe mass with an epicenter in the left lower lobe bronchus with invasion into the mediastinum and multiple hepatic metastases.No metastasis to bones,brain or spleen was noted.A core biopsy was performed on one of the liver metastases.Histopathology findings were consistent with metastatic squamous cell carcinoma,moderately differentiated.Immunohistochemistry of biopsied tissue sample was positive for markers p63,cytokeratin 5/6 heterogeneously positive;negative for thyroid transcription factor,cytokeratins 7,caudal-related homeobox transcription factor 2 and GATA binding protein 3.Thus,immunohistochemistry findings were also consistent with squamous cell carcinoma of lung.The tissue sample shows high programmed cell death ligand 1 expression (Figure 1).
FINAL DIAGNOSIS
Calcitriol induced hypercalcemia.
TREATMENT
Our patient was paucisymptomatic but had rapid rise in serum calcium level so we decided to treat her hypercalcemia.The patient was managed with intravenous normal saline,subcutaneous calcitonin administered twice,and a single infusion of zoledronic acid 4 mg during the course of the hospital stay.Her calcium level improved rapidly to 9.8 mg/dL within 48 h and she was discharged from the hospital.Her calcium level 2-wk later was noted to be elevated again at 13 mg/dL and was given another dose of zolendronic acid.Four weeks after discharge,her calcium level was noted to be within the normal range at 9.9 mg/dL.
OUTCOME AND FOLLOW-UP
The patient is scheduled to receive infusion of zolendronic acid once every month to manage hypercalcemia.She is planned to undergo chemotherapy with carboplatin,paclitaxel and pembrolizumab.
DISCUSSION
Hypercalcemia results from dysregulation between normal bone formation and the degradation cycle.The pathophysiology of HAM can be broadly classified into: (1) Local osteolytic hypercalcemia;(2) Humoral hypercalcemia mediated through PTHrP;and (3) Excess production of 1,25-dihydroxy vitamin D (calcitriol).
In the current case,calcitriol level was noted to be significantly elevated with suppressed PTH level and minimal elevation of PTHrP.The question is about what’s causing the calcitriol elevation in this case.Squamous cell cancer of the lung is usually associated with hypercalcemia driven by PTHrP elevation.In granulomatous disease such as sacrcoidosis,there is extrarenal production of calcitriolviaautonomous 1-α-hydroxylase activity in tissue macrophages.PTHrP can also upregulate 1-alpha hydroxylase activity and calcitriol production in mice models,but it does not increase calcitriol production in humans[8,9].In this patient,we tend to believe that hypercalcemia was due to a PTHrP-independent mechanism since PTHrP was minimally elevated.Additionally,extrarenal synthesis of calcitriol is dependent on its substrate 25-hydroxyvitamin D,which was low in this case,thus excluding extrarenal calcitriol production as an underlying mechanism.It’s very possible that it was being ectopically produced by tumor cells in an autonomous fashion[10].Although staining of the biopsy sample for 1,25-dihydroxy vitamin D and 1-alpha-hydroxylase was not done to confirm calcitriol’s ectopic production,the treatment response further solidifies our hypothesis.Increased calcitriol level in cases of granulomatous disease is believed to be due to the upregulation of 1-alpha hydroxylase activity,and its autocrine regulation is sensitive to corticosteroid therapy.Hence,corticosteroid is indicated in the treatment of hypercalcemia in such cases[11,12].However,in our case,hypercalcemia responded remarkably to treatment with bispho-sphonate and didn’t require any steroid treatment,making us doubtful of any increased 1-alpha-hydroxylase activity.
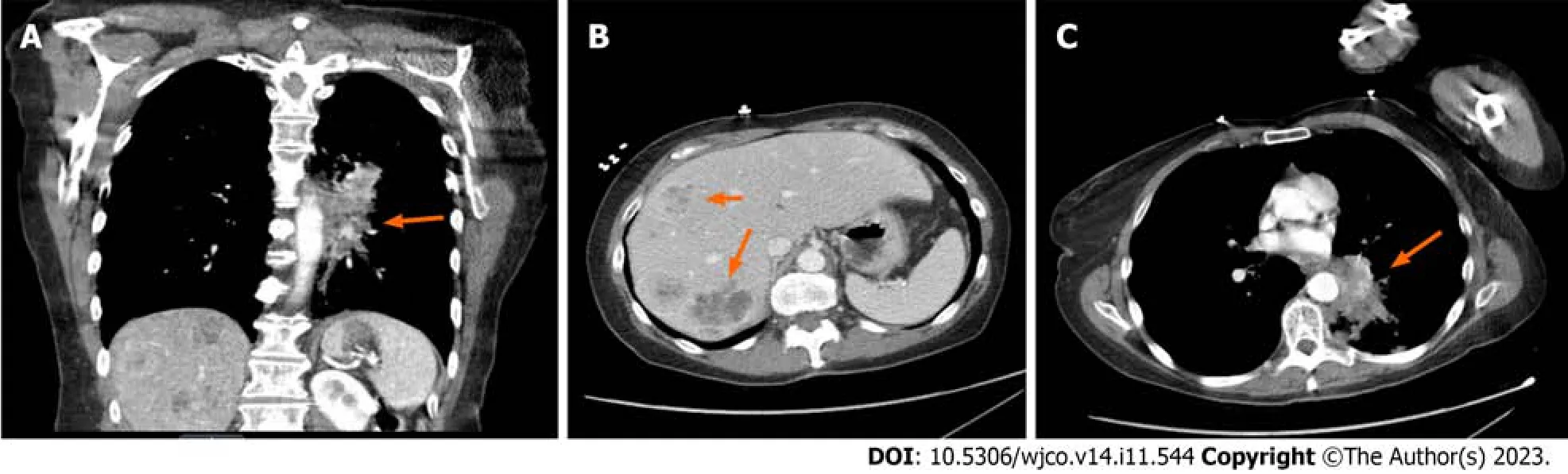
Figure 1 Computed tomography images. A: Computed tomography (CT) showing left lower lobe mass involving left bronchus;B: CT abdomen with contrast showing liver metastases;C: CT chest showing left lower lobe mass invasion into mediastinum.
The standard treatment approach for HAM is aimed at: (1) Promoting renal calcium excretion through intravenous normal saline administration and even loop diuretics,sometimes;and (2) Reducing bone absorption through the use of bisphosphonates and denosumab in refractory cases.Calcitonin can also be used as an adjunctive therapy with bisphosphonates,but tachyphylaxis develops within 48 h.Corticosteroids are the first-line agents for the treatment of calcitriolmediated hypercalcemia by inhibiting the transcription of 25-hydroxyvitamin D-1-hydroxylase;however,it was not required in our case.That being said,bisphosphonates may have more of a role in the treatment of HAM.Bisphosphonate may inhibit the adhesion of osteoclast precursors to stromal osteoblasts through the increased expression of intercellular adhesion molecule-1,which is promoted by calcitriol[13,14].In a case series reported by Rizzoliet al[15],bisphosphonate was more effective than steroids in the treatment of hypercalcemia,probably due to its bone anti-resorptive effect.Bisphosphonates may have additional effects,including induction of apoptosis,inhibition of invasion,and antiangiogenic properties,as seen in some preclinical studies[16].It would be worthwhile to conduct further research to investigate the cellular effects of calcitriol and bisphosphonate in patients with lung cancer.
CONCLUSION
We believe that the underlying cause of hypercalcemia,in this case of metastatic squamous cell lung carcinoma,was elevated calcitriol,which was likely produced by the tumor cells.In addition to PTHrP,calcitriol levels should be included in the workup for hypercalcemia in cases of lung cancer.However,the pathophysiology and prognostic significance of dysregulated calcitriol production in solid tumors remain unclear and warrant further research.Bisphosphonate may be used as a steroid-sparing therapy even in cases of calcitriol-induced hypercalcemia and warrants further investigation.
FOOTNOTES
Author contributions:Alalwan A conceived the idea,did the literature search,managed the case on medical floor,contributed to case presenrtation and the introduction;Khalid F and Bader H contributed the discussion;Du D and Meghal T edited and revised the manuscript.
Informed consent statement:Informed consent was obtained by the patient.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016),and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:United States
ORCID number:Farhan Khalid 0000-0002-8456-5118.
S-Editor:Wang JJ
L-Editor:A
P-Editor:Wang JJ
杂志排行

World Journal of Clinical Oncology的其它文章
- Analysis of clinicopathological features and prognostic factors of breast cancer brain metastasis
- Clinical study of standard residual liver volume and transient elastography in predicting poor prognosis of patients after hemihepatectomy
- System describing surgical field extension associated with flap reconstruction after resection of a superficial malignant soft tissue tumor
- Computational exploration of the significance of COPS6 in cancer:Functional and clinical relevance across tumor types
- Circulating tumor cells as potential prognostic biomarkers for earlystage pancreatic cancer: A systematic review and meta-analysis
- Bibliometric analysis of the global research status and trends of mechanotransduction in cancer