Clinical study of standard residual liver volume and transient elastography in predicting poor prognosis of patients after hemihepatectomy
2023-12-18ZhiQiangYuePengZhangShuaiYanLinLingJuHuiXuanWangLiuXiaYuanLinChenJinZhuWuYaLiCao
Zhi-Qiang Yue,Peng Zhang,Shuai Yan,Lin-Ling Ju,Hui-Xuan Wang,Liu-Xia Yuan,Lin Chen,Jin-Zhu Wu,Ya-Li Cao
Abstract BACKGROUND Liver cancer resection,especially in patients with hemihepatectomy or extended hemihepatectomy,often leads to poor prognosis,such as liver insufficiency and even liver failure and death,because the standard residual liver volume (SRLV)cannot be fully compensated after surgery.AIM To explore the risk factors of poor prognosis after hemihepatectomy for hepatocellular carcinoma and evaluate the application value of related prognostic approaches.METHODS The clinical data of 35 patients with primary liver cancer in Nantong Third People's Hospital from February 2016 to July 2020 were retrospectively analyzed.The receiver operating characteristic curve was created using medcac19.0.4 to compare the critical values of the SRLV in different stages of liver fibrosis after hemihepatectomy with those of liver dysfunction after hemihepatectomy.It was constructed by combining the Child-Pugh score to evaluate its application value in predicting liver function compensation.RESULTS The liver stiffness measure (LSM) value and SRLV were associated with liver dysfunction after hemihepatectomy.Logistic regression analysis showed that an LSM value ≥ 25 kPa [odds ratio (OR)=6.254,P <0.05] and SRLV ≤0.290 L/m2 (OR=5.686,P <0.05) were independent risk factors for postoperative liver dysfunction.The accuracy of the new liver reserve evaluation model for predicting postoperative liver function was higher than that of the Child-Pugh score (P <0.05).CONCLUSION SRLV and LSM values can be used to evaluate the safety of hemihepatectomy.The new liver reserve evaluation model has good application potential in the evaluation of liver reserve function after hemihepatectomy.
Key Words: Hepatocellular carcinoma; Hemihepatectomy; Prognosis; Standard residual liver volume; Liver stiffness measure value
INTRODUCTION
Liver cancer is a malignant tumor associated with high mortality worldwide[1-3].Hepatocellular carcinoma (HCC),one of the main types of liver cancer,is often found in advanced stages and cannot be cured[4-6].As a highly heterogeneous disease,HCC mostly develops as a result of hepatitis B cirrhosis[7].China has the largest number of hepatitis B virus infections in the world;therefore,the number of HCC patients accounts for more than half of the total number of HCCs worldwide[8].To date,surgical resection and liver transplantation are still effective treatments for HCC;however,due to the shortage of liver sources,the main treatment for HCC is surgery[9].Liver cancer resection,especially in patients with hemihepatectomy or extended hemihepatectomy,often leads to poor prognosis,such as liver insufficiency and even liver failure and death,because the standard residual liver volume (SRLV) cannot be fully compensated after surgery[10].Research suggests that preoperative liver fibrosis and cirrhosis are the main causes[11].In recent years,an increasing number of studies have shown that the liver stiffness measure (LSM) value is significantly related to the degree of cirrhosis,which can reflect the degree of liver inflammation and fibrosis[12,13].Accordingly,the purpose of this study was to investigate the risk factors and predictive methods of poor prognosis after hemihepatectomy for HCC and verify whether the changes in liver structure can be reflected by the LSM value and SRLV to assess the liver's compensatory capacity.Finally,we established a liver reserve function evaluation model by combining the LSM value and Child-Pugh scores and evaluated its application value.
MATERIALS AND METHODS
Patient characteristics
The clinical case data were obtained from 35 HCC patients undergoing hemihepatectomy in the Nantong Third People’s Hospital between February 2016 and July 2020,and all patients met the inclusion criteria for this study.The study was approved by the Ethics Committee of the Nantong Third People's Hospital Affiliated with Nantong University.Written informed consent was obtained from all patients before being enrolled in the study.The inclusion criteria were as follows:(1) According to the China liver cancer staging for the diagnosis and treatment standard of primary liver cancer (2019 edition),the stage of liver cancer was stage Ia,Ib or IIa,the tumor was located only in the left or right half of the liver,and hemihepatectomy was needed;(2) all patients were positive for HBsAg before the operation,and HCC was confirmed by pathology after surgery;(3) liver enhancement computed tomography (CT) was performed before the operation;(4) the LSM value was detected by transient elastography (Fibro Touch) before the operation;and (5) patients had more complete clinical case data.The exclusion criteria were as follows: (1) The patient did not have a standard hemihepatectomy;(2) the postoperative pathology of the patients was confirmed as cholangiocarcinoma or metastatic carcinoma;(3) the patient had a preoperative intervention,ablation,or chemoradiotherapy;(4) secondary operation;(5) other complications affecting liver function before the operation,such as hepatic encephalopathy,abdominal dropsy,and other conditions;and (6) the presence of other malignant tumors or serious diseases.
Surgical procedure
The patient was placed in a supine position with a soft pad on the high right lumbar back (no pad height was required for left hemihepatectomy),an oblique incision was made at the right abdominal costal margin,approximately 30 cm in length,layer by layer into the abdominal cavity;adhesions were separated,and each connective tissue and ligament of the liver were cut to fully expose the liver.The texture and morphology of the liver and spleen were observed,the completely free left or right lobe of the liver was selected according to the location of the tumor,the lesions that had not been detected before the operation were examined by intraoperative ultrasound,and the abdominal cavity was explored for the presence or absence of tumor implantation and metastasis.Subsequently,the liver hilum was selectively blocked,and the left or right hemiliver was resected,along with the gallbladder removal and extended hemihepatectomy according to the preoperative conditions,with surgical margins generally larger than 1 cm from the tumor margin.The operation area was carefully checked for the presence or absence of bleeding and biliary fistula,an abdominal drainage tube was placed,and each layer of the abdominal wall was closed layer by layer.
Determination of SRLV
Preoperatively,Philips brilliance CT was used to perform a routine double-phase scan of the patient's liver with a thickness of 1.25 mm.Then,portal vein stage tomography was selected,and rapid liver volume measurement software was used to draw the liver boundary layer-by-layer (the inferior vena cava and gallbladder were avoided) and calculate the total liver volume (TLV).The volume of half of the liver was measured by drainage after the liver was isolated.The body surface area (BSA) was calculated according to the literature[14,15].Finally,postoperative remnant liver volume(RLV)=TLV-the volume of half of the liver,and SRLV=RLV/BSA.
Determination of LSM values
According to the measurement requirements of the American Association for the Study of Liver Diseases[16],we measured the LSM value using a liver FibroTouch (FT) device developed by Haskell Medical Technology Company.In detail,the LSM value was measured 10 consecutive times for each patient,the quartile spacing was specified to be less than 30% as the effective measurement,and the median was chosen as the LSM value.All operations were performed by the same physician with extensive experience in the diagnosis of hepatobiliary diseases using ultrasound.A schematic illustration of the measurement results is shown in Figure 1.Then,a new model of liver reserve assessment was constructed according to the combination of the Child-Pugh score and the LSM value (Table 1).
Evaluation of postoperative hepatic fibrosis
By observing the paraffin sections of the liver under the microscope,we phased fibrosis according to the Scheuer scoring system as follows[17]: S0 stage,no liver fibrosis;S1 stage,liver fibrosis limited to the portal region;S2 stage,liver fibrosis extending to the portal region or portal interval,but the vascular relationship was normal;S3 stage,liver fibrosis with structural changes but not obvious cirrhosis;and S4 stage,cirrhosis (Figure 2).
Evaluation of postoperative liver function
According to the definition of liver dysfunction after hepatectomy from the International Study Group of Liver Surgery[18],we defined liver dysfunction as the results of a 5-d laboratory examination after hepatectomy that showed elevated international normalized ratio (INR) and total bilirubin (INR >1.5;total bilirubin >20.5 mmol/L);additionally,the patient was assessed for liver function,kidney function,respiratory function and the need for special assessment and special clinical treatment.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics 25.0,and the measurement data were compared using thettest or single-factor analysis of variance (ANOVA).The Wilcoxon rank-sum test was used when the variance was uneven,and the Chi square test was used for counting data.Analysis of independent risk factors was completed using unconditional logistic regression.We used medcalc19.0.4 to draw the receiver operating characteristic (ROC) curve of the subjects and analyzed the area under the ROC curve under different factors.P<0.05 was considered statistically significant.

Table 1 The new liver reserve assessment model
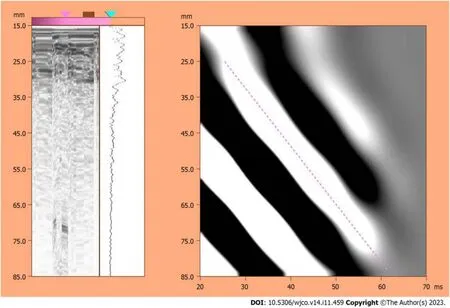
Figure 1 Schematic diagram of transient elastography results of the liver.
RESULTS
Risk factors for liverdysfunction after hemihepatectomy
The 35 patients in this study were grouped according to the presence or absence of liver dysfunction after surgery as follows: 12 patients had postoperative liver dysfunction,and 23 patients had no liver dysfunction.Then,the following 25 factors were analyzed.The results showed that the preoperative LSM value and SRLV were correlated with liver dysfunction after hemihepatectomy in HCC patients (P<0.05,Table 2).
LSM value and SRLV are independent risk factors for liver dysfunction after hemihepatectomy
The preoperative LSM value and SRLV were selected as independent variables,and regardless of whether liver dysfunction was selected as the dependent variable,a logistic regression model was developed for analysis.The results showed that the preoperative LSM value and SRLV were independent risk factors for liver dysfunction after hemihepatectomy (P<0.05,Table 3).
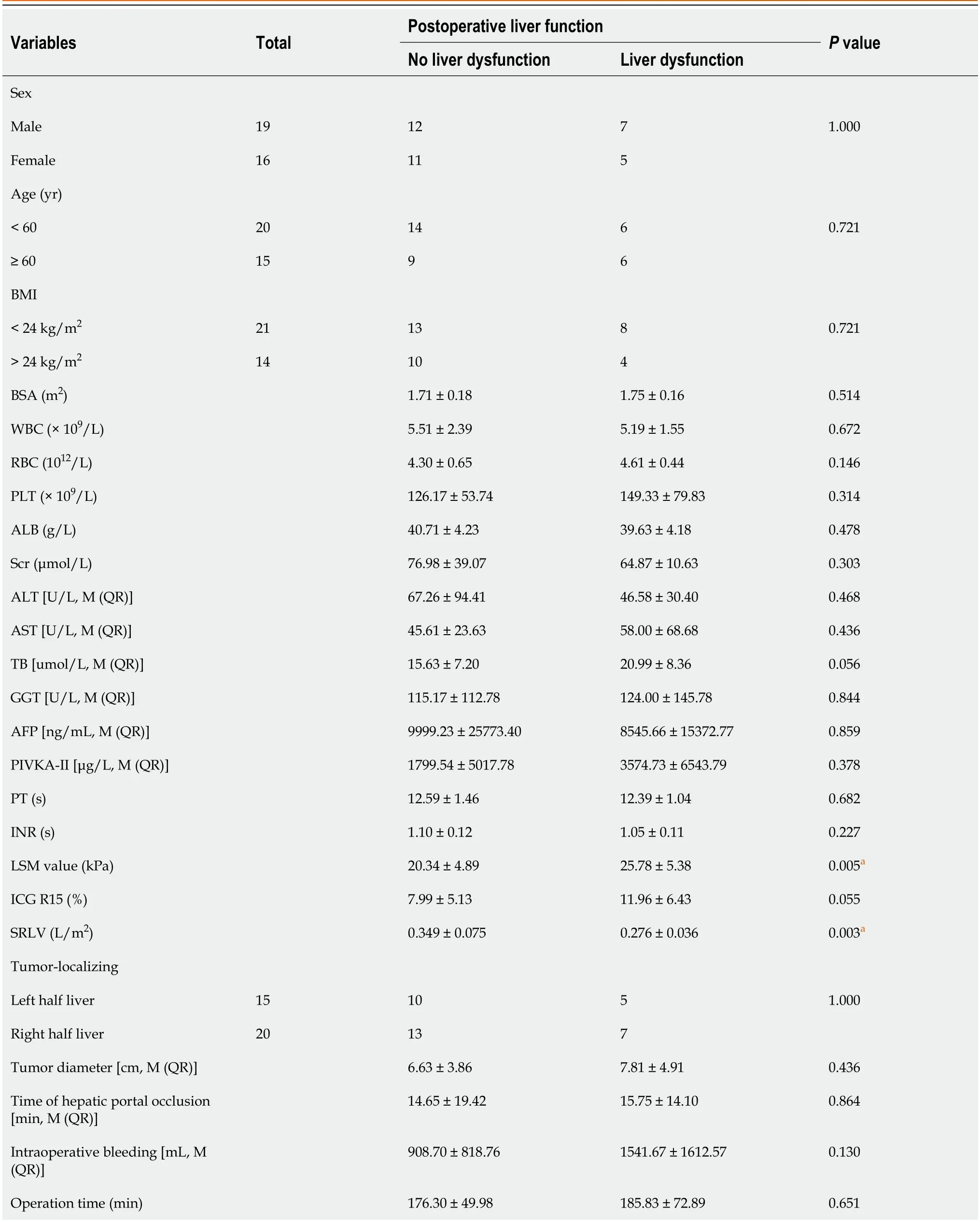
Table 2 Comparison of the clinical features of the surgical safety group and liver dysfunction group (mean ± SD)
The critical value of SRLV for different stages of postoperative fibrosis
The staging results of postoperative liver fibrosis showed 0 cases in the S0 stage,6 cases in the S1 stage,14 cases in the S2-S3 stage,and 15 cases in the S4 stage.Then,we compared and analyzed the critical values of SRLV for different stages,and the results showed that the difference in SRLV among the three phases was statistically significant (P<0.05,Table 4).ROC curve analysis showed that the area under the curve for the S2-S3 stage was 0.743,the sensitivity was 0.467,the specificity was 0.100,and the critical value of SRLV was 0.257 L/m2;the area under the curve for the S4 phase was 0.861,the sensitivity was 0.857,the specificity was 0.762,and the critical value of SRLV was 0.311 L/m2(Figure 3).
The critical value of SRLV for postoperative liver dysfunction
In 12 patients with postoperative liver dysfunction,the staging results of postoperative liver fibrosis showed 0 cases in the S0 stage,1 case in the S1 stage,7 cases in the S2-S3 stage,and 4 cases in the S4 stage.Additionally,the corresponding SRLVs were compared and analyzed,and the results showed that the difference in SRLV among the three phases was statistically significant (P<0.05,Table 5).ROC curve analysis showed that the area under the curve for stage S2-S3 was 0.943,the sensitivity was 0.857,the specificity was 0.100,and the safety-critical value for SRLV was 0.285 L/m2;the area under the curve for stage S4 was 0.938,the sensitivity was 0.100,the specificity was 0.750,and the safety-critical value of SRLV was 0.285 L/m2(Figure 4).
Application of a new assessment model in predicting liver dysfunction after hemihepatectomy
We reviewed and analyzed the clinical data of 35 patients in this study and followed up with the patients.The results showed that there were no postoperative deaths,and all patients were discharged within 3 wk after the operation.Statistical analysis showed that with Child-Pugh score was grade A,the accuracy rate of predicting postoperative liver function compensation was 54.8%;the accuracy rate of grade B was 25.0%.The new model was classified as grade I,and the accuracy rate of predicting postoperative liver function compensation was 100.0%,which was higher than that of the Child-Pugh score (χ2=7.452,P=0.007).Similarly,that of grade II was 91.3%,which was higher than the Child-Pugh score(χ2=9.928,P=0.013).There was a significant difference between the two models in evaluating the prognosis after hemihepatectomy (P<0.05,Table 6).
DISCUSSION
HCC is one of the most common malignant tumors.With the improvement of the technical level of hepatectomy,the mortality rate after HCC resection has decreased significantly[19-21].However,the mortality rate is still 5%-8%,especially in patients with hemihepatectomy[21].The main cause of death after hemihepatectomy is liver failure[22].The surgical resection range is so large such that the postoperative remnant liver cannot meet the needs of the body;more importantly,doctors lack a comprehensive understanding of the liver reserve function of patients before surgery.As a single evaluation indicator,indocyanine green (ICG) is better than many biochemical indicators.When many conventional liver function indicators have not yet become abnormal in value,the ICG retention rate at 15 min (ICG R15) can reflect liver function damage or occult liver disease in a timely manner[23].However,ICG has certain limitations and is easily interfered with by factors such as the patient's cooperation ability,liver cell uptake capacity,liver blood flow,bile duct obstruction,bilirubin,etc[24,25].SRLV is a reliable index of preoperative liver reserve function at home and abroad[26,27].However,considering that HCC patients often have varying degrees of liver fibrosis before the operation,the liver reserve and regeneration function in such patients may vary depending on the extent of liver fibrosis,even if the SRLV is the same;therefore,it is not satisfactory to evaluate liver reserve function only in terms of liver volume.The diagnosis of preoperative liver fibrosis mainly depends on liver histopathological examination;however,because of invasive examination,a low positive rate,difficulty in follow-up,and dynamic detection,the need to consider the wishes of patients and other factors,scholars at home and abroad have explored the use of elastic techniques instead of liver biopsy to assess the extent of liver fibrosis or cirrhosis by measuring the LSM value[17].Therefore,it is very important to evaluate the safety of hemihepatectomy by correctly staging the degree of liver fibrosis before surgery.
First,in this study,the factors that may be related to liver dysfunction in HCC patients after hemihepatectomy were statistically analyzed.The results showed that preoperative LSM and SRLV were associated with liver dysfunction in HCC patients after hemihepatectomy (P<0.05).Multivariate logistic regression analysis showed that preoperative LSM and SRLV were independent risk factors for liver dysfunction in HCC patients after hemihepatectomy.
Then,according to the Scheuer score standard,we observed the degree of liver fibrosis using microscopy and analyzed the SRLV critical value of different stages of liver fibrosis in all patients and the SRLV critical value of different stages of liver fibrosis in postoperative liver insufficiency cases by ROC curve analysis.The results showed that the critical values of SRLV were 0.257 L/m2and 0.310 L/m2in patients with liver fibrosis in stages S2-S3 and S4,respectively,and 0.285 L/m2in patients with postoperative liver dysfunction.SRLV critical values were similar in both cases,suggesting that it is safe and feasible to predict the SRLV threshold of HCC patients undergoing hemihepatectomy by pathological stages of liver fibrosis.It is suggested that the operation is safe if SRLV >0.310 L/m2.
At present,the elastic technique has been used to evaluate the degree of liver fibrosis or cirrhosis.It has been widely accepted because of its simplicity,repeatability,noninvasiveness,low cost,and other factors.At present,studies have reported that the sensitivity and specificity of the LSM value to predict the degree of hepatitis cirrhosis are high,and the LSM value is confirmed to be related to complications after partial hepatectomy in patients[28].However,there is no uniform standard for the patient's disease background,and the operation is limited to only partial or segmental hepatectomy.There is no study on the application of transient elastography to predict the degree of liver fibrosis andcirrhosis in hemihepatectomy,and there is no study on the LSM value in evaluating liver function reserve before hemihepatectomy.In addition,recent studies have shown that transient elastography cannot be used to accurately assess patients with obstructive jaundice.Therefore,more rigorous inclusion and exclusion criteria were adopted in this study.We used Fibro Touch elastic imaging equipment (FT-3.5R50) developed by Haskell Medical Technology Company and a two-dimensional ultrasonic probe to avoid the influence of liver tumors and large blood vessels inside and outside the liver on the measurement results.The measured LSM value was 22.20 ± 5.63 kPa,which is similar to that reported at home and abroad[12].We established a new liver reserve assessment model based on the Child-Pugh score combined with the LSM value and observed its application in the evaluation of liver reserve function in patients with HCC undergoing hemihepatectomy.The results showed that the accuracy of the new evaluation model in predicting postoperative liver function compensation was 100.0% (P<0.05),and the accuracy rate of predicting mildly poor liver function compensation after the operation was 91.3% (P<0.05),which was higher than that of the Child-Pugh score.

Table 3 Logistic regression analysis based on preoperative the liver stiffness measure value and standard residual liver volume

Table 4 The standard residual liver volume of different stages of liver fibrosis in 35 patients after hemihepatectomy (mean ± SD)

Table 5 The standard residual liver volume of different liver fibrosis stages in 12 patients with liver insufficiency after hemihepatectomy
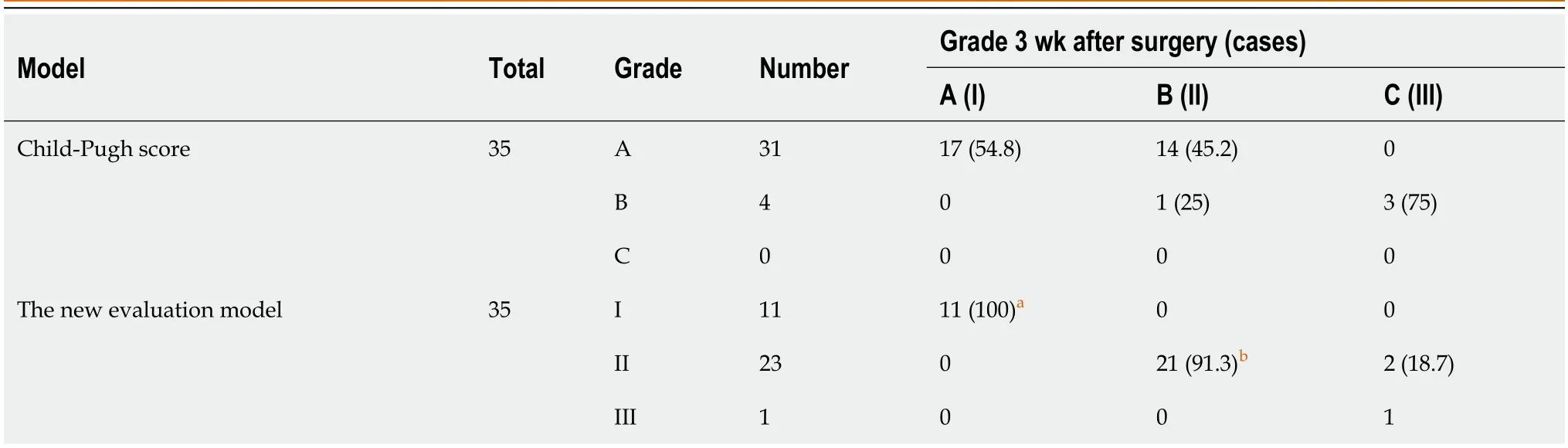
Table 6 The comparison of two assessment methods,n (%)

Figure 2 The different stages of liver fibrosis in 35 cases of hemihepatectomy (hepatic encephalopathy × 200). A: Stage S1;B: Stage S2;C:Stage S3;D: Stage S4.
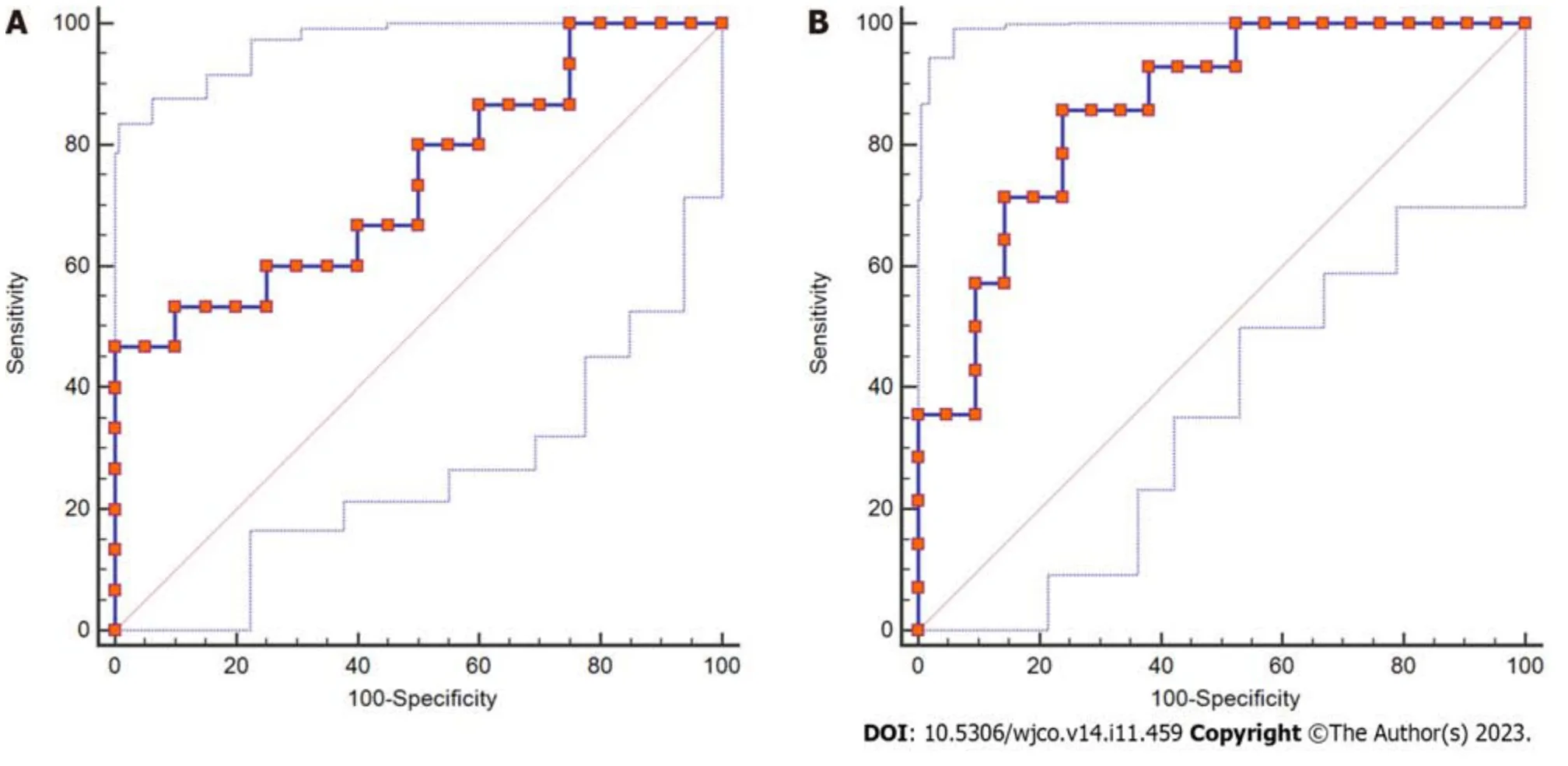
Figure 3 The receiver operating characteristic curve of the standard residual liver volume in different stages of liver fibrosis. A: Stages S2-S3;B: Stage S4.
Therefore,we believe that the new liver reserve assessment model can provide a reference for preoperative safety assessment of patients with liver cancer undergoing hemihepatectomy,which can increase patient safety during the perioperative period and reduce the incidence of liver failure after the operation.Additionally,it can provide a reference for patients with liver cancer who are expected to receive hemihepatectomy or extended hemihepatectomy.
CONCLUSION
In summary,through this study,we found that for patients with moderate or severe liver fibrosis,when the predicted SRLV is greater than 0.310 L/m2,the new evaluation model of liver function reserve predicts that the postoperative liver function compensation is good before the operation,and hemihepatectomy is safe;when the predicted SRLV is less than 0.285 L/m2,the new liver reserve assessment model predicts poor liver function compensation after hepatectomy,and the probability of liver dysfunction after hemihepatectomy is higher.A blind operation should be avoided,and the operation should be evaluated after full liver protection.Patients in whom severe liver dysfunction is expected after surgery need to undergo antiviral treatment and undergo portal vein embolization or associated life partition and portal vein ligation for staged hepatectomy,and the values of SRLV and LSM should be reevaluated after liver regeneration.After contralateral liver regeneration,the SRLV and LSM values are reevaluated.It is expected that hemihepatectomy is still feasible for patients with well-compensated liver function.The LSM value combined with SRLV is safe and reliable.
However,the sample size involved in this study is too small and has no statistical significance in theory;nevertheless,the author believes that the LSM value and SRLV are useful safety indices for the evaluation of HCC hemihepatectomy.The new liver reserve evaluation model based on the Child-Pugh score combined with the LSM value can improve on the Child-Pugh score;it has important clinical guiding importance for the evaluation of liver reserve function in HCC patients with hemihepatectomy and provides a theoretical basis for further investigations conducted by our research group.
ARTICLE HIGHLIGHTS
Research background
Liver cancer resection often leads to poor prognosis,because the standard residual liver volume (SRLV) cannot be fully compensated after surgery.
Research motivation
Hemihepatectomy or extended hemihepatectomy often leads to liver insufficiency and even liver failure.
Research objectives
This study aimed to explore the risk factors of poor prognosis after hemihepatectomy for hepatocellular carcinoma and evaluate the application value of related prognostic approaches.
Research methods
The clinical data of 35 patients with primary liver cancer were retrospectively analyzed.The critical values of SRLV in different stages of liver fibrosis after hemihepatectomy were compared with those of liver dysfunction after hemihepatectomy.
Research results
Logistic regression analysis showed that the liver stiffness measure (LSM) value ≥ 25 kPa [odds ratio (OR)=6.254,P<0.05)] and SRLV ≤ 0.290 L/m2(OR=5.686,P<0.05) were independent risk factors for postoperative liver dysfunction.The accuracy of the new liver reserve evaluation model for predicting postoperative liver function was higher than that of the Child-Pugh score (P<0.05).
Research conclusions
LSM values and SRLV can be used to evaluate the safety of hemihepatectomy.
Research perspectives
The new liver reserve evaluation model has good application potential in the evaluation of liver reserve function after hemihepatectomy.
ACKNOWLEDGEMENTS
We appreciate teachers and classmates support and guidance through this process.Express respect and gratitude to patients who provide medical records.
FOOTNOTES
Co-first authors:Zhi-Qiang Yue and Peng Zhang.
Co-corresponding authors:Jin-Zhu Wu and Ya-Li Cao.
Author contributions:Yue ZQ,Zhang P,Yan S,Yuan LX,Ju LL,Wang HX,Chen L,Cao YL and Wu JZ contributed equally to this work;Yue ZQ,Zhang P,Yan S,Yuan LX and Wu JZ were hepatobiliary surgeons;Ju LL,Wang HX,Yuan LX,Chen L and Cao YL were researchers in Nantong Institute of Liver Disease;Wu JZ,Chen L,Cao YL designed the research study;Yue ZQ,Zhang P,Yan S,Yuan LX,Ju LL and Wang HX performed the primary literature and data extraction;Yue ZQ,Zhang P analyzed the data and wrote the manuscript;Chen L,Cao YL and Wu JZ were responsible for revising the manuscript for important intellectual content;and all authors read and approved the final version.Yue ZQ and Zhang P have made equally significant contributions to this thesis.In accordance with the principles of rigorous and objective research and respect for the contributions of all team members,Zhang P is co-designated as the first author.Wu JZ (corresponding author) and Cao YL (co-corresponding author) provided financial support for this research.Wu JZ(corresponding author),as the research advisor of Yue ZQ (first author),was primarily responsible for the design and guidance of the paper.Meanwhile,Cao YL (co-corresponding author),as an authoritative expert,significantly contributed to the advancement of this study.Therefore,Cao YL is co-designated as the co-corresponding author.
Supported byNantong Municipal Health Commission,No.MSZ2022036 and No.QN2 022041;Nantong Science and Technology Bureau,No.JCZ2022036.
Institutional review board statement:This study was reviewed and approved by the Ethics Committee of the Nantong Third People’s Hospital (approval NO.EK201628).
Informed consent statement:All study participants or their legal guardian provided informed written consent about personal and medical data collection prior to study enrolment.
Conflict-of-interest statement:We have no financial relationships to disclose.
Data sharing statement:Technical appendix,statistical code,and dataset available from the corresponding author at 39235978@qq.com.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Zhi-Qiang Yue 0009-0001-0837-7414; Lin-Ling Ju 0000-0002-9541-0533; Lin Chen 0000-0002-1108-4735; Jin-Zhu Wu 0000-0002-7295-2030.
S-Editor:Qu XL
L-Editor:A
P-Editor:Zhang XD
杂志排行

World Journal of Clinical Oncology的其它文章
- Analysis of clinicopathological features and prognostic factors of breast cancer brain metastasis
- System describing surgical field extension associated with flap reconstruction after resection of a superficial malignant soft tissue tumor
- Computational exploration of the significance of COPS6 in cancer:Functional and clinical relevance across tumor types
- Circulating tumor cells as potential prognostic biomarkers for earlystage pancreatic cancer: A systematic review and meta-analysis
- Bibliometric analysis of the global research status and trends of mechanotransduction in cancer
- Autoimmune diabetes from pembrolizumab: A case report and review of literature