System describing surgical field extension associated with flap reconstruction after resection of a superficial malignant soft tissue tumor
2023-12-18AkioSakamotoTakashiNoguchiShuichiMatsuda
Akio Sakamoto,Takashi Noguchi,Shuichi Matsuda
Abstract BACKGROUND Flap reconstruction after resection of a superficial malignant soft tissue tumor extends the surgical field and is an indicator for potential recurrence sites.AIM To describe a grading system for surgical field extension of soft tissue sarcomas.METHODS Grading system: CD-grading is a description system consisting of C and D values in the surgical field extension,which are related to the compartmental position of the flap beyond the nearby large joint and deeper extension for the pedicle,respectively.C1/D1 are positive values and C0/D0 are negative.With a known location,1/0 values can be "p" (proximal),"d" (distal),and "b" (in the tumor bed),and the description method is as follows: flap type,CxDx [x=0,1,p,d or b].RESULTS Four representative patients with subcutaneous sarcomas who underwent reconstruction using fasciocutaneous flaps are presented.The cases involved a distal upper arm (elbow) synovial sarcoma reconstructed using a pedicled latissimus dorsi (pedicled flap: CpDp);a distal upper arm (elbow) pleomorphic rhabdomyosarcoma reconstructed using a transpositional flap from the forearm(transpositional flap: CdD0);an undifferentiated pleomorphic sarcoma in the buttocks reconstructed using a transpositional flap (transpositional flap: C0D0);and a myxofibrosarcoma in the buttocks reconstructed using a propeller flap from the thigh (pedicled flap: CdDd).CONCLUSION The reconstruction method is chosen by the surgeon based on size,location,and other tumor characteristics;however,the final surgical field cannot be determined based on preoperative images alone.CD-grading is a description system consisting of C and D values in the surgical field extension that are related to the compartmental position of the flap beyond the nearby large joint and deeper extension for the pedicle,respectively.The CD-grading system gives a new perspective to the flap reconstruction classification.The CD-grading system also provides important information for follow-up imaging of a possible recurrence.
Key Words: Soft tissue; Sarcoma; Surgery; Sarcoma; Grading system; Surgical flap
INTRODUCTION
Soft tissue sarcomas comprise a group of rare heterogeneous neoplasms that account for <1% of all cancers[1].Soft tissue sarcomas can occur in any soft tissue,but are most common in the extremities.Wide resection of the sarcoma and the surrounding normal tissue is necessary to reduce the recurrence rate[2].Flap reconstruction is used to repair soft tissue defects after resection of a soft tissue sarcoma,especially a superficial soft tissue sarcoma[3,4].
The term “tumor bed” refers to the area of tissue remaining after a malignant tumor is removed.The tumor bed includes the tumor and surrounding healthy tissues where cancer cells may exist[5].Use of a reconstruction flap following soft tissue sarcoma resection can extend the surgical field or tumor bed because of flap elevation or dissection of recipient vessels.
The current Cancer Staging Manual of the American Joint Committee on Cancer (AJCC) of soft tissue sarcoma is widely used based upon tumor size,histologic grade,and the presence of metastasis[6].AJCC supports theR classification,which categorizes surgical margins as negative (R0),microscopically positive (R1),or grossly positive (R2)[7,8].Flaps can be classified based on several factors (pedicled,free,or the tissue type from which the flap is made).Classification of flaps according to clinical complications has also been reported[9];however,there is no system describing surgical field extension related to flap reconstruction.
In the current report we propose a grading classification,the CD-grading system,to describe extension of the surgical field related to flap reconstruction after superficial soft tissue sarcoma resection.Representative cases are also presented.
MATERIALS AND METHODS
Classification: CD-grading system for a superficial sarcoma in the extremities
The new grading system (CD-grading system) was used herein for superficial soft tissue sarcomas with extremity resection reconstructed by fascio-(musculo)-cutaneous flaps.Upper extremity tumors are defined as lesions arising distal to the acromioclavicular joint and include tumors of the shoulder girdle and axilla.Lower extremity tumors are defined as lesions arising distal to the iliac crest,including tumors of the gluteal region[9].Additional skin grafting does not affect the grade;the skin grafting cases were not excluded.
The CD-grading system consists of C-and D-values.The C-value indicates the "compartmental position of the flap beyond the nearby large joint " and when the flap crosses a nearby large joint,the C-value is positive (C1).When the flap is within the compartment,the C-value is negative (C0).Large joints include the shoulders,elbows,wrists,hips,knees,and ankles.If the location of a flap crossing the joint location is proximal,the C-value is Cp (p=proximal) and when crossing a distal large joint the C-value is Cd (d=distal).
D-value means “deeper extension for the pedicle.” The pedicle is already exposed,and the negative D-value is D0.If dissection of the pedicle is necessary,the positive D-value is D1.When the dissected pedicle is located proximal to the surgical field,the D-value is Dp (p=proximal),when the dissected pedicle is located distally,the D-value is Dd (d=distal),and when the pedicle dissection is within the surgical bed,the D-value is Db (b=surgical bed;Tables 1 and 2).

Table 1 C-value for flap location beyond the nearby large joint

Table 2 D-value for surgical field extension for the pedicle dissection
The flap type is described before the CD-values as “flap type,CxDx,” in which x can be 0,1,p,d,or b.There is no strict rule in the description of the flap type;however,an easy and understandable description,such as distinguishing between a local or free flap,would be required.
Transpositional fascial flap/propeller flap
In cases involving transpositional fasciocutaneous or propeller flaps[10],the flap is located within the compartment,the C-value is C0,the D-value is D0,and the CD-grade is C0D0.When the flap is from the extra compartment across the large joint,the C-value is C1,the D-value is D0,and the CD-grade is C1D0.When the flap is obtained proximally and crosses a large joint,the CD-grade is CpD0,and when the flap is derived distally and crosses a large joint,the CD-grade is CdD0(Tables 3 and 4).
Pedicled flap
The C-value in the pedicle flap is the same as the transpositional flap.The flap is located within the compartment and the C-value is C0.When the flap comes from the extra compartment across the joint,the C-value is C1.C1 can be Cp or Cd depending on the flap location (proximal or distal).The D-value reflects the location of the pedicle.The pedicle flap needs extension of the surgical field to deeper tissues,therefore the D-value is always D1.When the pedicle is located proximal to the surgical field,D1 can be Dp (p=proximal),and when the pedicle is located distal to the surgical field,the D1 can be Dd (d=distal;Tables 3 and 5).
Free flap
The donated area of the flap does not affect the surgical field in terms of tumor contamination,and the C-value in the free flap is always C0.When the pedicle is already exposed at the surgical field,the D-value is D0.When the pedicle is not exposed,and the pedicle needs to be exposed,then the D-value is D1.When the pedicle is located proximal to the surgical field,D1 can be Dp (p=proximal),and when the pedicle is located distal to the surgical field,the D1 can be Dd (d=distal).When the pedicle is exposed at the deeper tissues within the surgical field,the D-value is Db (Tables 3 and 6).
RESULTS
Herein we present four cases of superficial soft tissue sarcomas.Two elbow soft tissue sarcomas and two buttock softtissue sarcomas are presented.One elbow soft tissue sarcoma patient was a 47-year-old female with a synovial sarcoma at the elbow (distal upper arm) reconstructed with a pedicled latissimus dorsi;the CD-grade was CpDp (pedicled flap,CpDp;Figure 1).The second elbow soft tissue sarcoma patient was an 85-year-old male with a pleomorphic rhabdomyosarcoma at the elbow (distal upper arm) reconstructed using a transpositional flap from the forearm;the CD-grade was CdD0 (transpositional flap,CdD0;Figure 2).The first patient with a buttock soft tissue sarcoma was a 65-year-old female with an undifferentiated pleomorphic sarcoma at the buttock reconstructed using a transpositional flap;the CD-grade was C0D0 (transpositional flap,C0D0[11];Figure 3).The second patient with a buttock sarcoma was a 46-year-old male with a myxofibrosarcoma that was reconstructed using a propeller flap from the thigh;the CD-grade was CdDd (pedicled flap,CdDd;Figure 4).

Table 3 Possible classification of flap reconstruction

Table 4 Transpositional fasciocutaneous flap/propeller flap

Table 5 Pedicled flap
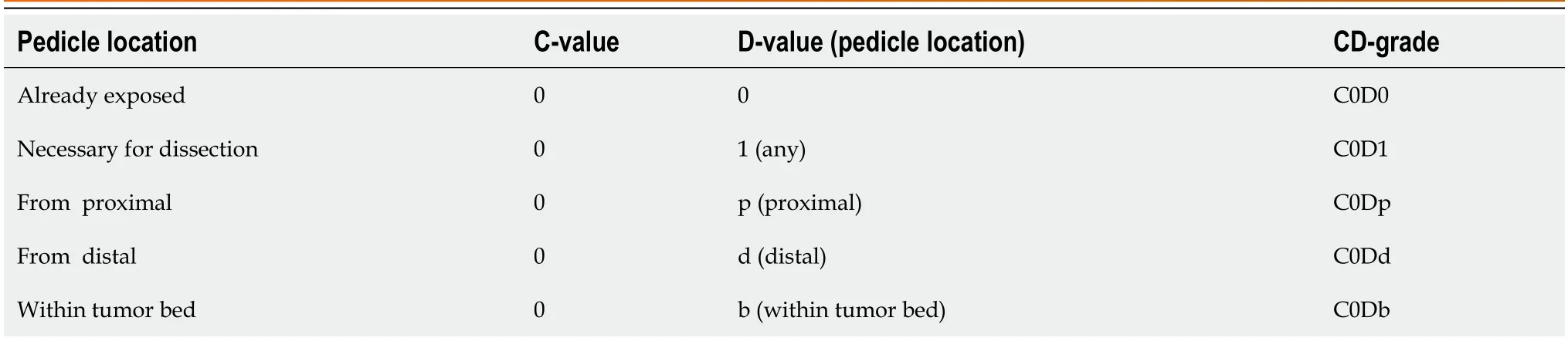
Table 6 Free flap
DISCUSSION
Soft tissue sarcomas require wide resection with healthy tissue margins[12,13].Thus,the surgical field is wider than the tumor size.The extension of the tumor bed has the possibility of tumor contamination.Therefore,recognition of tumor bed extension is necessary.Discrepancies between the preoperative tumor burden and postoperative tumor bed contour have been identified after tumor burden replacement with a latissimus dorsi flap[14].Flap reconstruction increases the surgical field during superficial soft tissue sarcoma resection[15].
A flap is applied to the defect after resection of a soft tissue sarcoma,especially a superficial soft tissue sarcoma.The choice of flap is often determined by the surgeon's preference,as well as the location of the tumor.The tumor bed after resection of soft tissue sarcomas cannot be predicted solely based on preoperative imaging.If amputation is necessary in the case of a re-occurrence,the level of amputation is important.Extension of the tumor bed due to flap reconstruction carries the risk of tumor contamination and may require more proximal amputation.The C-value gives information that indicates the likelihood of tumor contamination across the greater joint.

Figure 1 Synovial sarcoma at the distal upper arm (elbow) reconstructed by a pedicled latissimus dorsi (pedicled flap,CpDp). A: A 47-yearold female with a synovial sarcoma at the elbow (distal upper arm).Magnetic resonance imaging showed a tumor with heterogenous low-to-high signal intensity on the T2-weighted image.Before (A-I) and after (A-II) chemotherapy of doxorubicin and ifosfamide,the tumor size was reduced.B-D: A wide surgical resection was performed with a pedicled latissimus dorsi.The CD-grade was CpDp (pedicled flap,CpDp).

Figure 2 Pleomorphic rhabdomyosarcoma at the distal upper arm (elbow) reconstructed by transpositional flap (transpositional flap,CdD0). A: An 85-year-old male with a pleomorphic rhabdomyosarcoma at the elbow (distal upper arm);B: Magnetic resonance imaging showed a tumor with homogenous high-signal intensity on T2-weighted images (B-I) and low-signal intensity on T1-weighted images (B-II).A wide surgical resection was performed.The transpositional flap was obtained from the upper arm and forearm;C-G: Skin grafting was performed at the forearm.The CD-grade was CdD0 (transpositional flap,CdD0).
There is a risk of tumor contamination if deep tissues are created in the surgical field.The D-value represents the location of the pedicle.Dissection of the pedicle and recipient vessels requires dissection to the deeper layers,resulting in extension of the surgical field,with a D-value of D1.Transposition flaps in the compartment do not require exposure of the donor vessels,therefore less deep tissue exposure is advantageous in terms of reducing the potential for tumor recurrence,with a D-value of D0.Similarly,even in cases of a free flap requiring microsurgery,if the recipient vessels are already exposed,the D-value is D0 because deeper tissue dissection is not necessary.
The AJCC Staging of Soft Tissue Sarcomas (eighth edition) is based upon the tumor size,histologic grade,and the presence of metastasis.Tumor size is classified into four categories with border values of 5,10,and 15 cm.The notation regarding tumor depth (superficial or deep from the superficial fascia) has been eliminated from the seventh edition of the AJCC Staging of Soft Tissue Sarcomas[6].The surgical staging of musculoskeletal sarcomas has 4 types of surgical margins [intralesional,marginal,wide,and radical (compartmental)],as proposed by Ennekinget al[16].A 2-3 cm surgical margin provides reasonable local control of soft tissue sarcomas[17].The AJCC supports theR classification,which categorizes margins as negative (R0),microscopically positive (R1),or grossly positive (R2)[7,8].Furthermore,the Union Against Cancer (UICC) proposed aR+1 mm classificationthat requires 1 mm of healthy tissue between the tumor and margin to define a negative margin (R0)[18,19],thus resulting in more resections being considered microscopically positive (R1).Radiation therapy can be performed as adjuvant therapy,especially if cancer cells remain after the resection.Radiation has a role in reducing the risk of recurrence in soft tissue sarcoma resection[5].The term,tumor bed,refers to the area of tissue remaining after a malignant tumor is removed.The tumor bed may have cancer cells[5].Recognition of tumor bed extension is necessary for postoperative radiation.Without flap reconstruction following soft tissue sarcoma resection,the tumor bed can largely be predicted with the preoperative staging based upon the images and the histologic findings.With flap reconstruction,tumor bed prediction is difficult without the surgical method information.Indeed,the new grading system can give information of surgical field extension associated with flap reconstruction.

Figure 3 Undifferentiated pleomorphic sarcoma at the buttock reconstructed by a transpositional flap (transpositional flap,C0D0). A: A 65-year-old female with an undifferentiated pleomorphic sarcoma at the buttock.Magnetic resonance imaging revealed a subcutaneous tumor.The tumor had a cystic appearance and contained liquid with slightly high signal intensity on the T2-weighted image.The periphery of the cystic wall was thick with a solid neoplastic lesion and intermediate signal intensity on T2-weighted images (A-I).Computed tomography showed that the lesion is located at the buttock (A-II);B: A resection of the tumor was designed;C and D: The tumor was resected and the defect was reconstructed with a transpositional flap donated from the lateral abdomen.The CD-grade was C0D0 (transpositional flap,C0D0).
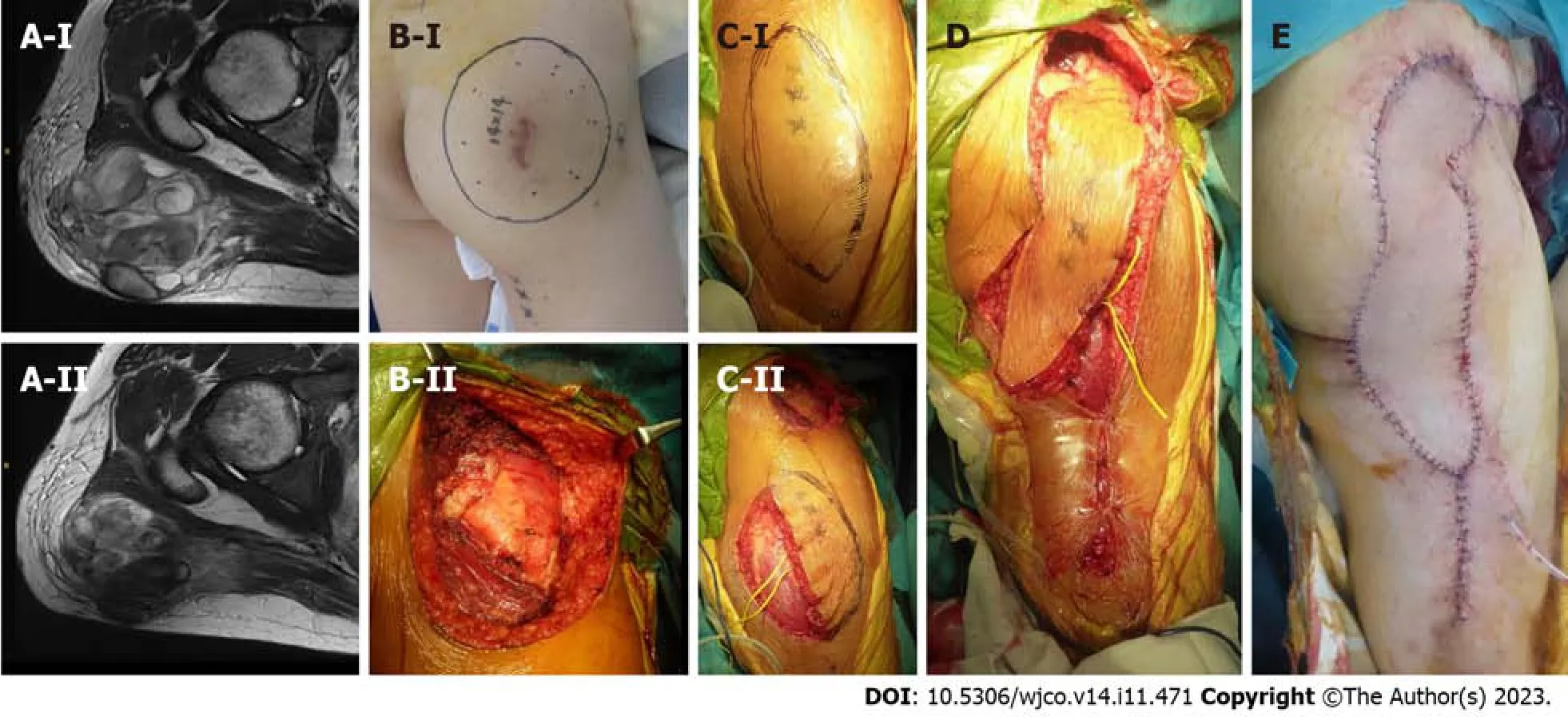
Figure 4 Myxofibrosarcoma at the buttock reconstructed by a propeller flap (pedicled flap,CdDd). A: A 46-year-old male with a myxofibrosarcoma at the buttock.Magnetic resonance imaging revealed that the tumor showed heterogenous low-to-high signal intensity on the T2-weighted image.Before (A-I) and after (A-II) chemotherapy of doxorubicin and ifosfamide,the tumor size was reduced;B: The resection of the tumor was designed (B-I) and performed (B-II);C and E:A propeller flap from the thigh was designed (C-I) and the pedicle was preserved (C-II) and performed.The CD-grade was CdDd (pedicled flap,CdDd).
There are several limitations in the new grading system.First,this classification is completely new and still theoretical.Clinical use of the assembled clinical data would be necessary,and some modification may be required for improvement.Second,the new grading system was used for superficial soft tissue sarcomas resected in the extremities and fascio-(musculo)-cutaneous flaps,in which hands and feet were not included.The new grading system might be modified for any part of bones and soft tissue sarcomas.Third,flap type description is not strictly defined in the new grading system,which may result in ambiguity;however,according to the flap technique improvement,description of the flap would be diverse.Therefore,no flap description restrictions were used in the new grading system.Finally,the new grading system cannot describe the length or area required for postoperative radiation.Excessive information in the grading system,however,would make the new grading system difficult for clinical use.
CONCLUSION
We have proposed a method to describe extension of the surgical field in reconstruction after superficial soft tissue sarcoma resection.The method described can give values for tumor bed extension after flap reconstruction.The description of whether or not the operative field has been extended due to reconstruction is considered to be important information for image evaluation of recurrence.
ARTICLE HIGHLIGHTS
Research background
Flap reconstruction can extend the surgical field or tumor bed because of flap elevation or dissection of recipient vessels during resection of superficial soft tissue sarcomas.There is currently no method describing extension of the surgical field.
Research motivation
Extension of the surgical field cannot be predicted based on preoperative images for flap reconstruction after superficial soft tissue sarcoma resection.Knowledge of the surgical field extension is important information for evaluation of recurrence images or possible postoperative radiation.
Research objectives
A theoretical CD-grading system was developed consisting of C and D values in the surgical field extension.The C-value represents the flap beyond the nearby large joint and the D-value pertains to a deeper extension.
Research methods
C1/D1 and C0/D0 are positive and negative values,respectively.With a known location,C values are "p" (proximal),"d"(distal),and "b" (in the tumor bed).The description method is as follows: flap type,CxDx [x=0,1,p,d or b].
Research results
Classification and possible values are shown in the tables (transpositional fascial flap/propeller,pedicled,and free flaps).Four representative patients with subcutaneous sarcomas who underwent reconstruction using fasciocutaneous flaps are presented.
Research conclusions
The new grading system can give values for tumor bed extension after flap reconstruction following superficial soft tissue sarcoma resection.The description of whether or not the operative field has been extended due to reconstruction is thought to be important information for evaluation of recurrence images.
Research perspectives
Clinical use of assembled clinical data would be necessary and some modification may be required for improvement,especially if the new grading system is modified for any part of bone and soft tissue sarcomas.
FOOTNOTES
Author contributions:Sakamoto A developed the classification and drafted the manuscript;Noguchi T and Matsuda S participated in the study design;All authors read and approved the final manuscript.
Institutional review board statement:Analysis of clinical data accumulation in patients with bone and soft tissue tumors.Retrospective study.
Informed consent statement:The patients represented in this study were informed that the data from the case would be de-identified and used in a journal publication.There is a specific signed document because the analysis used anonymous clinical data that were obtained after each patient had been notified at the Kyoto University home page that the data could be used for a clinical study.
Conflict-of-interest statement:We,the authors,declare no conflicts of interest regarding our manuscript entitled “A system describing surgical field extension associated with flap reconstruction after resection of a malignant soft tissue tumor.”
Data sharing statement:No additional data are available.
STROBE statement:The authors have read the STROBE Statement—checklist of items,and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Japan
ORCID number:Akio Sakamoto 0000-0002-7518-1606; Takashi Noguchi 0000-0003-2965-4772; Shuichi Matsuda 0000-0003-0802-1255.
S-Editor:Liu JH
L-Editor:A
P-Editor:Liu JH
杂志排行

World Journal of Clinical Oncology的其它文章
- Analysis of clinicopathological features and prognostic factors of breast cancer brain metastasis
- Clinical study of standard residual liver volume and transient elastography in predicting poor prognosis of patients after hemihepatectomy
- Computational exploration of the significance of COPS6 in cancer:Functional and clinical relevance across tumor types
- Circulating tumor cells as potential prognostic biomarkers for earlystage pancreatic cancer: A systematic review and meta-analysis
- Bibliometric analysis of the global research status and trends of mechanotransduction in cancer
- Autoimmune diabetes from pembrolizumab: A case report and review of literature