Post-transplant biliary complications using liver grafts from deceased donors older than 70 years:Retrospective case-control study
2023-10-21CarlosJimenezRomeroIagoJustoAlonsoPilardelPozoElsoAlbertoMarcacuzcoQuintoCristinaMartArriscadoArrobaAlejandroManriqueMunicioJorgeCalvoPulidoAlvaroGarcSesmaRicardoSanRomOscarCasoMaestro
Carlos Jimenez-Romero, Iago Justo-Alonso, Pilar del Pozo-Elso, Alberto Marcacuzco-Quinto, Cristina Martín-Arriscado-Arroba, Alejandro Manrique-Municio, Jorge Calvo-Pulido, Alvaro García-Sesma, Ricardo San Román, Oscar Caso-Maestro
Abstract
Key Words: Older liver; Liver transplant; Biliary complications; Biliary strictures; Septuagenarian donors; Octogenarian donors
INTRODUCTION
Excellent outcomes obtained with liver transplantation (LT) have led to an increasing number of candidates on the waiting list. However, the number of liver grafts remains stable. The historical liver shortage and subsequent waiting list mortality (5.2% in 2019)[1] led us to expand the donor pool using livers from extended-criteria donors, such as those with split-liver, living-related, and donor after circulatory death (DCD)[2]. However, our group principally increased the progressive utilization of livers from older donors, without an age limit, a practice already initiated in 1996[3].
There is controversial because some series have reported a significantly worse patient and graft survival[4,5] using older livers from deceased donorsvsother reports defending the use of septuagenarian[6-11] and octogenarian liver grafts for non-hepatitis C virus (HCV) diseases[6,8,9,12-15]. A recent study from the Scientific Registry of Transplant Recipients has demonstrated that the use of liver grafts ≥ 70 years provide substantial long-term survival benefits,compared to waiting for a better organ offer[16]. In contrast, several series using older livers from donors after brain death (DBD) have demonstrated significantly higher incidence of post-LT biliary complications (BC) than the use of younger livers[11,17-21], considering BC is a major source of morbi-mortality and costs[21-23]. There are no studies analyzing the incidence and outcomes of BC in patients older and younger than 70 years. There is only a recent metaanalysis that did not find significant differences in BC between recipients of liver grafts ≥ 70 years and those of grafts < 70 years[24].
Thus, the aim of the present study is to analyze specifically the incidence, outcomes, and risk factors of BC in patients who underwent LT using liver grafts from donors older than 70 years.
MATERIALS AND METHODS
Study population and design
Between April 1986 and December 2019, 2057 LTs were performed at our hospital. Between January 1994 and December 31, 2019, 297 LTs were performed using livers older than 70 years. In order to achieve a more homogeneous study population, and avoid confounder factors we excluded 47 LTs because of the following reasons: re-transplantation (11 patients), acute liver failure (9 patients), donation after circulatory death (3 patients), simultaneous liver kidney (1 patient), primary non-function (7 patients), and hepatic artery thrombosis (HAT) (16 patients). Thus, our sample comprised 250 LTs divided into two groups as follows: patients who developed post-LT BC (n= 21) and those without BC(n= 229) (Figure 1).
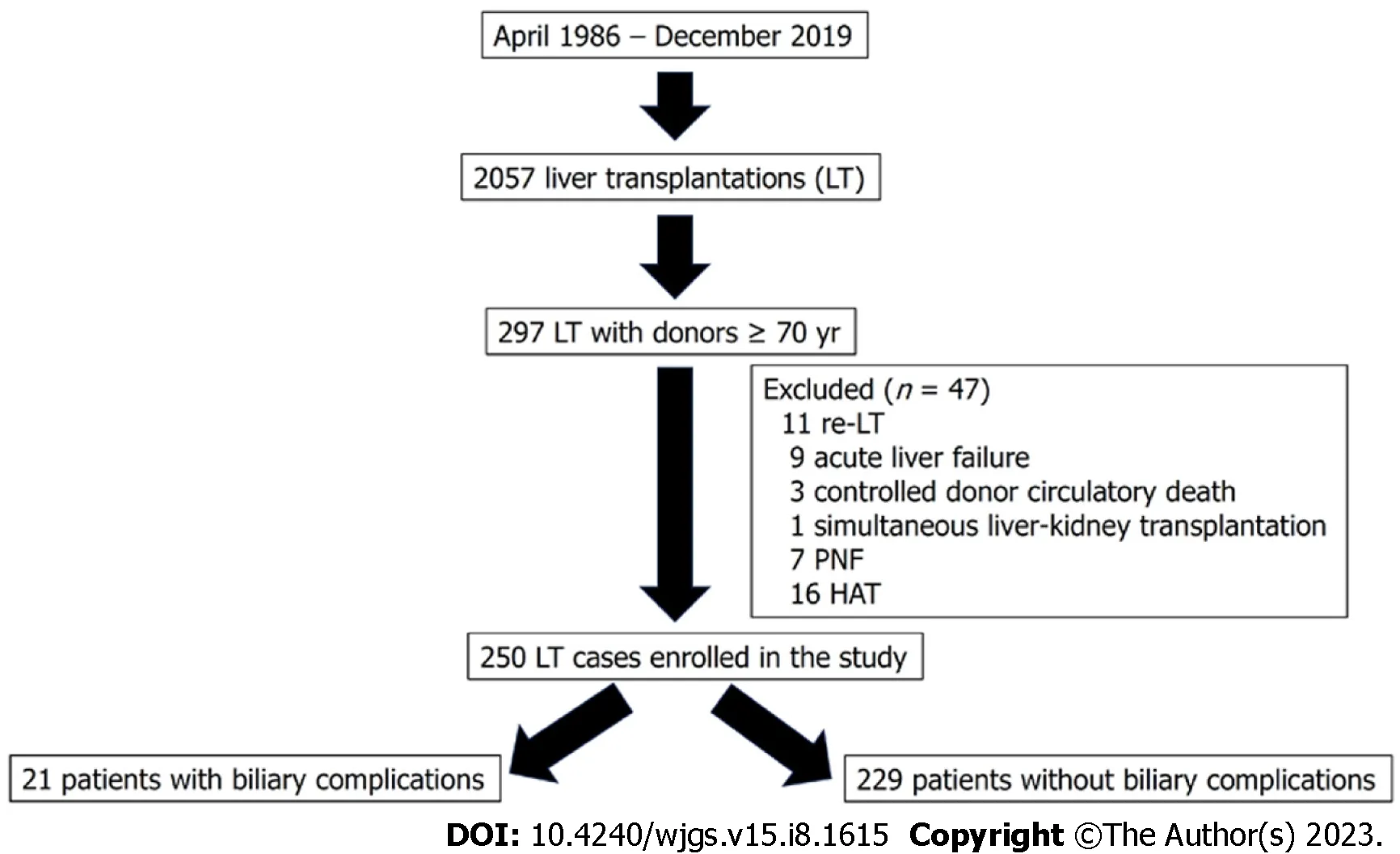
Figure 1 Flowchart for patient selection. HAT: Hepatic artery thrombosis; PNF: Primary non- function; LT: Liver transplantation.
A retrospective case-control study was carried out comparing both groups and following the STROBE guidelines for reporting observational studies[25].
This study was terminated on June 31, 2021, with a minimal follow-up period of 18 mo after LT. Patients were not required to give informed consent to the study because the analysis used anonymous data that was collected after each patient agreed to treatment by written consent. This study was approved by our Institutional Review Board, and it was conducted and reported according to the declaration of Helsinki. All data generated or analyzed during this study are available upon request.
Donor evaluation and transplant technique
General criteria for the acceptance of liver grafts older than 70 years for LT at our department were the following: good pre-procurement hemodynamic stability avoiding severe hypotension episodes or the use of high doses of vasopressors,bilirubin < 2.5 mg/dL, transaminases < 150 IU/L, intensive care unit (ICU) stay < 4 d, soft graft consistency, liver biopsy displaying the absence of hepatitis or fibrosis or macro-steatosis up to 25%, and cold ischemia time (CIT) usually not exceeding 9 h. The presence of atheroma at the bifurcation of the common hepatic artery or gastroduodenal artery was a contraindication for the use of older livers. All liver grafts were biopsied at the beginning of the procurement. Dual aortic and portal vein flush was performed using Belzer or Celsior (since 2008 to present) preservation solutions. Donor procurement was performed according to standard techniques, except for donors displaying hemodynamic instability. A rapid procurement technique was carried out in such cases. The gallbladder and biliary tract were flushed with cold saline solution at the beginning of procurement.
Recipient hepatectomy was performed using the vena cava-sparing technique (piggy-back). Portal reperfusion was performed initially, followed by arterial anastomosis and subsequent arterial reperfusion. The vascularization of the donor and recipient choledochus was carefully preserved. Biliary reconstruction was usually performed by an end-to-end choledocho-choledochostomy, without a T-tube, using interrupted sutures of polyglyconate 5-6/0. A T-tube was only placed in cases of extremely small bile ducts, diameter discrepancy between both the donor and recipient bile ducts, or intraoperative difficulties. A cholangiography through a T-tube was usually performed on postoperative day 7, closing the tube at 5-8 d thereafter. Three months after LT, a second cholangiography through the T-tube was repeated, being then removed if there were not abnormal radiological findings. Similarly, Roux-en-Y hepaticojejunostomy (RYHJ) was only indicated inpatients with a diameter extreme discrepancy between both donor and recipient bile ducts or in case of recipients with biliary disease or prior RYHJ.
Donor and recipient characteristics
The following donor variables were evaluated: Demographics, ICU stay, the cause of death, medical history, cardiac arrest, hemodynamic instability, norepinephrine use, laboratory values (serum glucose, creatinine and sodium, liver function, and coagulation parameters), the presence of micro- and/or macro-steatosis, CIT, warm ischemia time (WIT),and preservation solutions. Moreover, the following pre-LT recipient data were assessed: demographics, LT indication,the presence of hepatocellular carcinoma (HCC), pre-LT transarterial chemoembolization (TACE), model for end-stage liver disease (MELD), MELD- Na, D-MELD scores, United Network for Organ Sharing (UNOS) status, medical history,major abdominal operations, and laboratory values (serum glucose, creatinine, albumin, liver function, and hematological parameters).
Perioperative variables, morbi/mortality, and patient and graft survival
The following perioperative variables were analyzed: Biliary reconstruction techniques, intraoperative transfusion, and base immunosuppression. Post-LT complications, such as early allograft dysfunction (EAD), acute renal failure, nonsurgical related infections, acute rejection, HCV and HCC recurrence, non-biliary related reoperations, re-transplantation,ICU and hospital stay, patientfollow-up, overall mortality rate and causes, and patient and graft survival were also analyzed.
Definitions
Non-anastomotic biliary stricture (NABS) or ischemic-type biliary lesion was defined as any stricture, dilation, or irregularity of the intra- or extra-hepatic bile ducts, with a patent hepatic artery. In contrast, anastomotic biliary stricture (ABS)was defined as a lesion localized within the biliary anastomosis[19]. Anastomotic biliary leakage (ABL) was defined as the presence of bile leak through abdominal drainage oran intra-abdominal biliary collection requiring radiological or surgical drainage.
Biliary strictures were diagnosed based on the clinical symptoms and cholestasis laboratory pattern, confirmed at the first era by ultrasound, CT scan and percutaneous transhepatic cholangiography (PTC). From 2005, a magnetic resonance imaging cholangiography (MRIC) was used for stricture confirmation. PTC was used for biliary stricture delineation and subsequent balloon dilation therapy. RYHJ was performed only after an interventional radiology failure.
EAD was defined according to Olthoffet al[26]. Post-LT acute renal failure was defined as a > 0.5% increase in the serum creatinine level or > 50% over the baseline value[27]. Acute and chronic rejection and HCV recurrence were confirmed by biopsy.
Immunosuppression
The immunosuppressive regimen consisted of cyclosporine or tacrolimus and prednisone. Mycophenolate mofetil or mammalian target of rapamycin inhibitors were introduced when appropriate, and tacrolimus was reduced. Steroids were usually discontinued between 3-6 mo.
Statistical analysis
The statistical review of the study was performed by a biomedical statistician. Continuous variables were expressed as mean ± SD and as median and interquartile range, according to the Kolmogorov-Smirnov test results. Qualitative variables were expressed as absolute frequencies (n) and relative frequencies (%). The chi-square test and Fisher's exact test were performed to compare the qualitative variables. In contrast, the continuous variables were compared using thet-test. Non-parametrictests were conducted when appropriate. The graft and patient survival rates were estimated using the Kaplan-Meier method. Donor and recipient variables (P< 0.10) from the univariate analysis were subsequently investigated in a multivariate analysis to assess their eventual effect on the development of BC. The results were expressed as odds ratios (ORs) and 95% confidence intervals (CIs). AP-value < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS Statistics, version 27 (SPSS Inc., Chicago, IL, United States).
RESULTS
Donor and recipient characteristics
A total of 250 patients underwent LT using liver grafts from donors aged ≥ 70 years (175 and 75 patients were septuagenarians and older than 80 years, respectively). The overall incidence of BC in this series was 8.4%. If we divide the patients who underwent LT into two eras, donor age was similar (76.1 years in the first eravs77.6 years in the second era;P=0.073), and no significant differences were found (P= 0.551) regarding the rate of BC: 6.6% (4 cases) in the first era (61 LT performed between January 1994 and December 2004), and 9% (17 cases) in the second era (189 LT performed between January 2005 and December 2019).
The mean donor age was similar between the groups (BC and non-BC), and women were significantly less frequent in the BC group (P= 0.017). Moreover, we did not find differences in obesity, body mass index, ICU stay, and causes of donor death, and cerebrovascular disease was the most frequent cause of death. There were also no differences in hypertension, diabetes, hemodynamic instability, and norepinephrine use. The incidence of cardiac arrest was significantly higher in the BC group than that in the non-BC group (19%vs5.7%;P= 0.043). Donor laboratory values were similar, except for a lower platelet count in the BC group (P= 0.016).
There were no significant differences in the rates of micro-steatosis and macro-steatosis, and the mean CIT and WIT values were similar too (Table 1).
The median recipient age was equal in both groups, and there were no significant differences in LT indications. Pre-LT TACE as a bridging therapy in patients with HCC, MELD scores, and UNOS status demonstrated similar frequencies.Medical history, such as hypertension, diabetes, and pre-LT major abdominal operations were more frequent in the BC group, but the difference was statistically in significant. While the median values of total bilirubin were significantly lower (P= 0.036) in the BC group, the prothrombin rate was significantly higher (P= 0.030) (Table 2).
Perioperative characteristics and morbi/mortality
We observed a statistically significant difference in biliary tract reconstruction techniques between the groups (P= 0.013).Choledocho-choledochostomy without a T-tube was the most frequent technique (76.2% cases in the BC groupvs86.9%cases in the non-BC group), but the frequency of choledocho-choledochostomy with a T-tube and RYHJ was higher in the BC group.
Post-LT complications, such as EAD, acute renal failure, acute rejection, and non-biliary related reoperations, were similar between the groups. The rate of non-surgical related infections was higher, but statistically insignificant in the BCgroup (28.6%vs13.1%;P= 0.062). Other complications, such as HCV and HCC recurrence rates, did not differ significantly. None of the patients who developed BC underwentre-transplantation. The median follow-up period of the BC group was lower than that of the non-BC group, but differences were not statistically significant (46 ± 56 movs72 ± 95 mo;P= 0.099). Overall mortality was lower but no significant in the BC group (28.6%vs38.9%;P= 0.352). Infections were the main cause of the death in the BC group and cardiovascular disease and malignancies were the main cause of death in the non-BV group (P= 0.041) (Table 3).
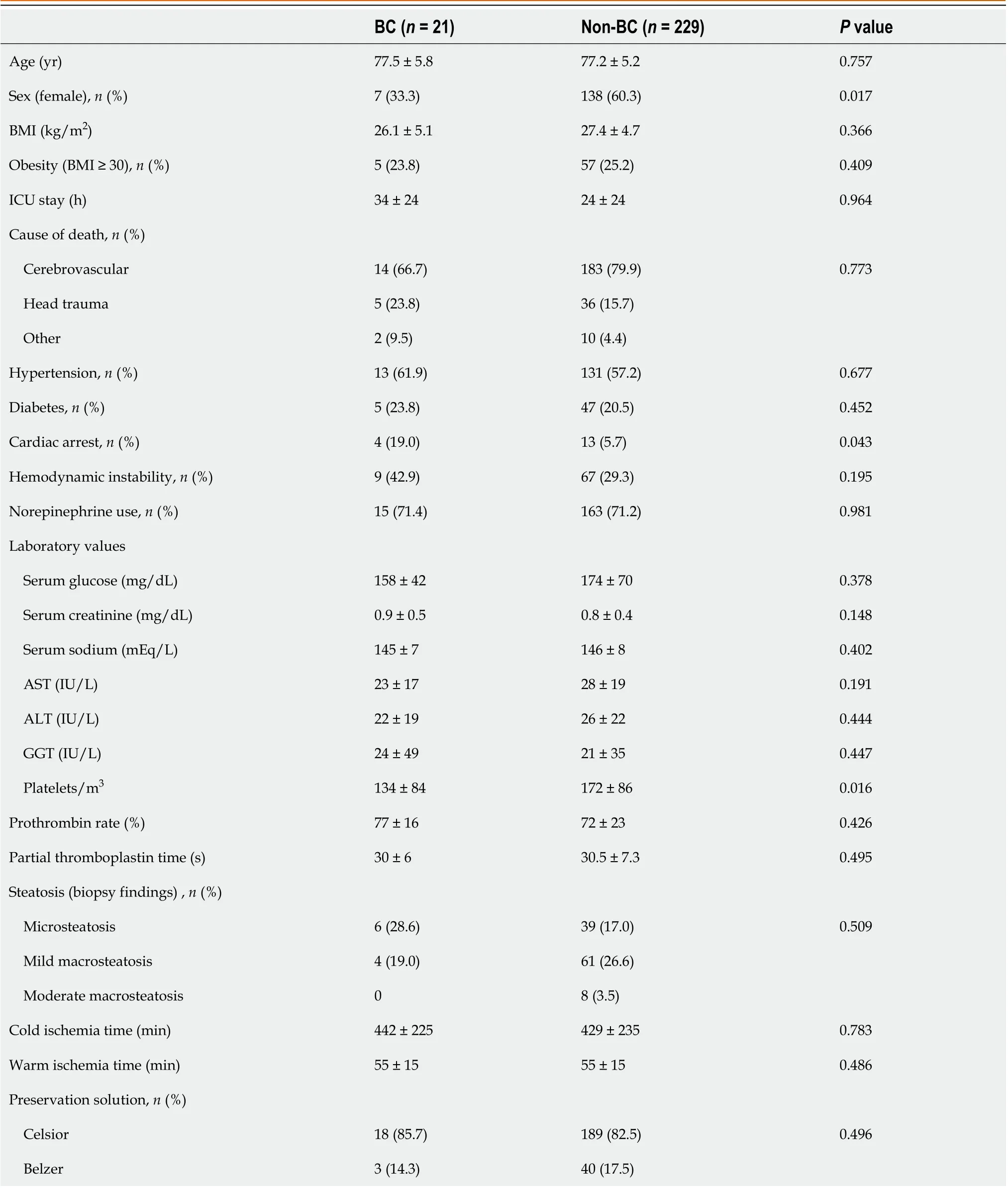
Table 1 Donor characteristics

Table 2 Pre-liver transplantation recipient characteristics
Patient and graft survival
There were no significant differences in the patient and graft survival between the recipients of donors aged ≥ 70 years who developed BCvsnon-BC recipients. The 1-, 3-, and 5-year patient survival rates in the BC group were 81.0%, 81.0%,and 67.5%, respectively,vs86.9%, 80.2%, and 72.5%, respectively, in the non-BC group (P= 0.954; Figure 2A). The 1-, 3-,and 5-year graft survival rates in the BC group were 81.0%, 81.0%, and 67.5%, respectively,vs86.0%, 78.8%, and 71.1%,respectively, in the non-BC group (P= 0.909; Figure 2B).
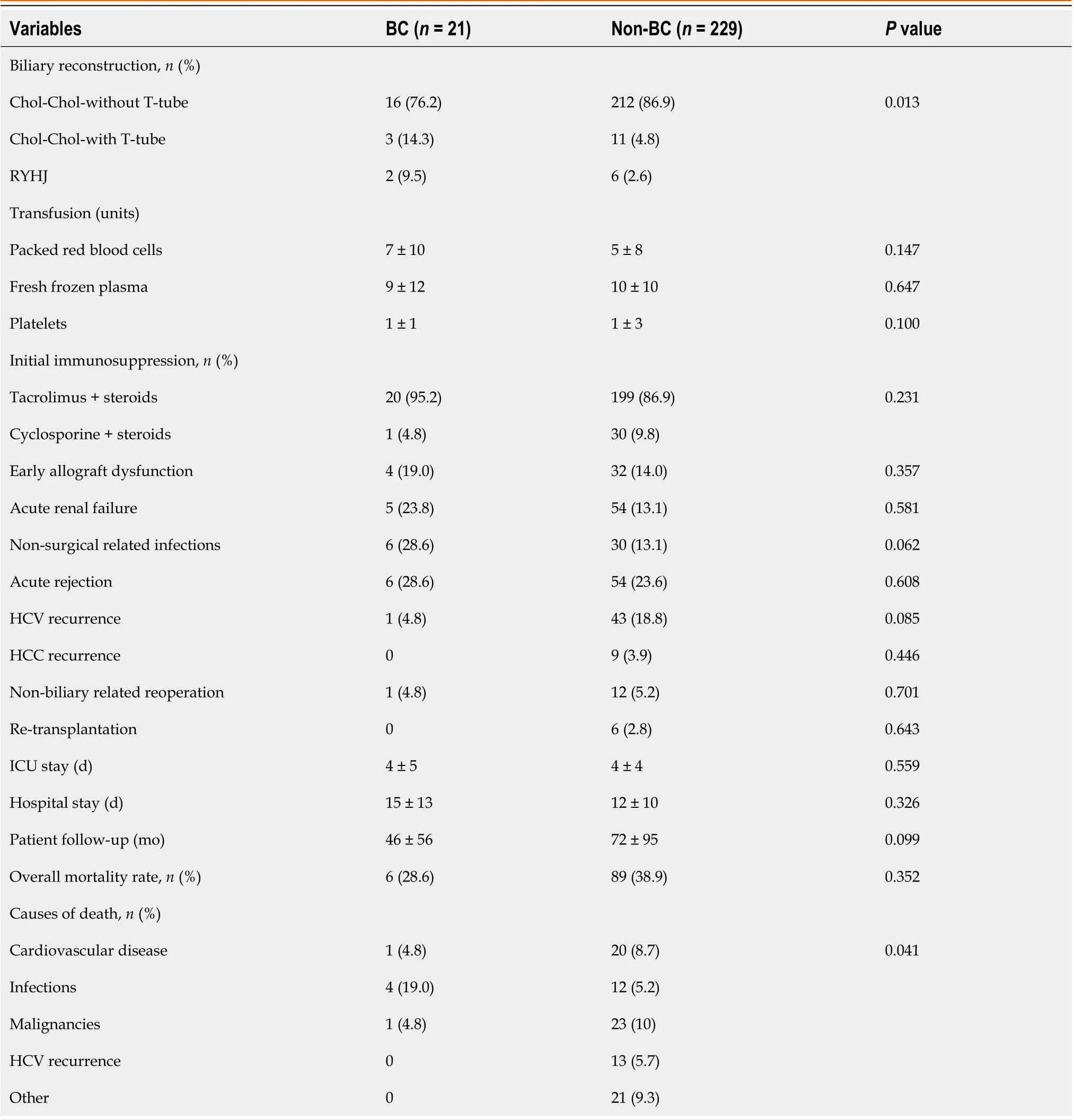
Table 3 Perioperative variables and morbidity/mortality
Univariate and multivariate analysis of predictors of BC
In the univariate analysis, donor variables, such as female donors (OR: 0.33; 95%CI: 0.13-0.85,P= 0.021), cardiac arrest(OR: 3.91; 95%CI: 1.14-13.30,P= 0.029), and platelet count (OR: 1.00; 95%CI: 1.00-1.00,P= 0.031) displayed statistically significant differences. In the multivariate analysis, while female donors (OR: 0.27; 95%CI: 0.08-0.90,P= 0.033) was a protective factor for BC, donor cardiac arrest (OR: 7.66; 95%CI: 1.52-38.61,P= 0.013) was a risk factor (Table 4).
Diagnosis, management, and outcomes of patients with BC
The incidence of BC in 175 recipients of septuagenarian liver grafts and 75 recipients of octogenarian liver grafts was 7.4%and 10.7%, respectively (P= 0.398). The initial techniques of biliary reconstruction were choledocho-choledochostomy without a T-tube, with a T-tube, and RYHJ in 16 patients, 3 patients, and 2 patients, respectively. MRIC was used in nine patients to confirm ABS following an ultrasound. While 15 (71.4%) patients were diagnosed with BC within the first year of LT (eight ABS and seven ABL), 6 (28.6%) patients were diagnosed after the first year (five ABS and one mild NABSwithout any therapeutic requirement).
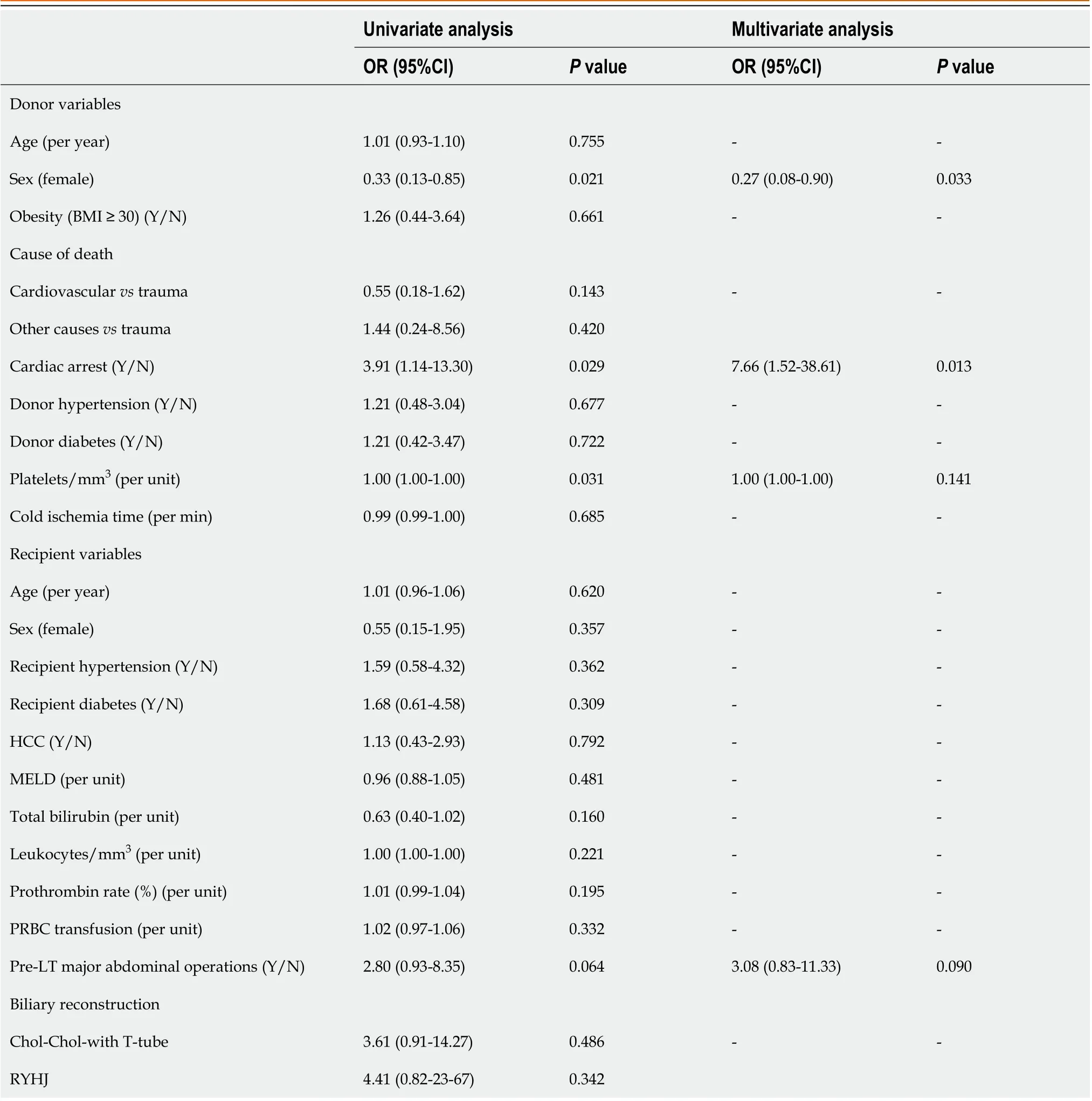
Table 4 Univariate and multivariate analysis of predictors of biliary complications
Of the 7 patients with ABL, 3 (42.8%) patients closed spontaneously, and 4 (57.2%) patients required reoperation (two were treated by a leakage repair, one underwent RYHJ, and the remaining patient with a prior RYHJ underwent several surgeries because of multiple biliary complications). Nine (69.2%) of the 13 patients with ABS underwent PTC balloon dilation (range: 1-6 times), and 4 patients underwent RYHJ. In addition, 4 patients also required a RYHJ procedure due to failure of prior PTC balloon dilation. During follow-up, 6 patients died among those who developed BC (5 among the recipients of septuagenarian donors, and 1 among recipients of octogenarian donors). However, only three (14.3%)ofthese deaths were related to BC (two in recipients of septuagenarian donors, and one in a recipient of an octogenarian donor) (Table 5).
DISCUSSION
Before the introduction of direct-acting antivirals (DAAs), the use of older livers in patients with HCV was associated with a significantly lower patient and graft survival owing to HCV recurrence[28]. However, on excluding recipients withHCV cirrhosis, the patient and graft survival did not differ between the recipients of octogenarian and septuagenarian donors[29]. Currently, the scenario has dramatically changed, and well-selected liver grafts without an age limit can be used, without the fear of HCV recurrence on treating the patients with DAA[30]. The liver is the most permissive organ,in relation to the donor age because of its regenerative property[31]. However, older livers are more susceptible to prolonged cold ischemia times[32]. Biological and chronological aging of the old liver donors is not always the same because the general status and physiologic reserve vary markedly by lifestyle factors[33] and comorbidities. To obtain good results using older livers, the donors and recipients should be selected carefully to avoid theiruse in sick patients[29].

Table 5 Diagnosis, management, and outcomes of patients with biliary complications post-liver transplantation with grafts older than 70 years
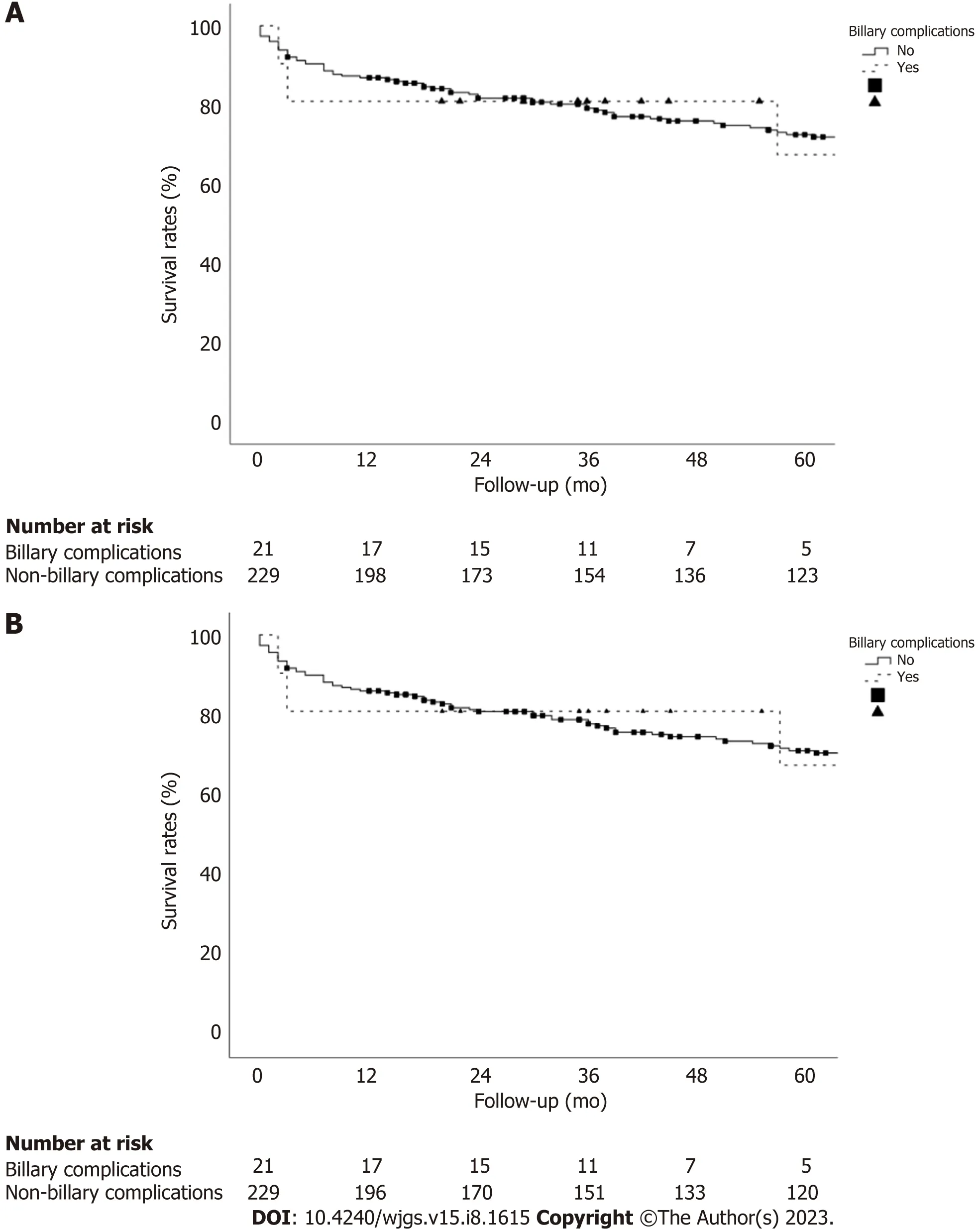
Figure 2 Comparison of patient and graft survival between the recipients of donors older than 70 years who developed biliary complications vs those without biliary complications. A: The 1-, 3-, and 5-year patient survival rates in the biliary complications (BC) group are 81.0%,81.0%, and 67.5%, respectively, vs 86.9%, 80.2%, and 72.5%, respectively, in the without BC (non-BC) group (P = 0.954); B: The 1-, 3-, and 5-year graft survival rates in the BC group are 81.0%, 81.0%, and 67.5%, respectively, vs 86.0%, 78.8%, and 71.1% in the non-BC group (P = 0.909).
Most BC are diagnosed within 1-year post-LT, and the overall incidence among the recipients of livers from DBD younger than 80 years reportedly ranges between 12%-44%[8,11,21,23,34-36]. In contrast, the overall incidence of BC using livers older than 80 years ranges between 6.7%-23.9%[6,13-15,29,37-39]. One of these series using only octogenarian livers reported on an overall incidence of 23.9%, corresponding17% of these patients to type NABS[38]. In other study, the same authors found the donor age ≥ 80 years as a risk factor for the development of NABS when performing a single aorticvsdual perfusion (aortic and portal) during donor procurement[39]. Three other studies compared post-LT BC for liver grafts younger and older than 70 years, and the incidence ranged between 9%-19% and 12%-15.1% in recipients of septuagenarian and octogenarian livers, respectively, without significant differences between thegroups[8,40,41]. In other comparative study, the incidence of NABS was 13% for liver grafts ≥ 65 yearsvs19% for grafts < 65 years[35].
The overall rate of BC among our recipients of donors ≥ 70 years was 8.4%, without significant differences between the two groups (7.4% in recipients of septuagenarian donorsvs10.7% in recipients of donors ≥ 80 years;P= 0.398). We divided the patients into two groups according to the era of LT (beforeor after December 2004) to investigate an eventual influence of the period of LT over the incidence of BC. The age of the donor was higher in the second era, nevertheless the difference was statistically insignificant. Of note, overall rate of BC (8.4%) in our study was lower than overall rate of 12.1% previously reported in a systematic review analysis of five series of LT using livers older than 70 years[24].
Researchers have described several donor risk factors for BC, such as the use of older liver grafts, donors with extended criteria, DCD livers, macro-steatosis > 25%, atherosclerosis, the use of high viscosity preservation solution, CIT> 10 h, severe hypotension of the donor or recipient, ABO incompatibility, smallbile ducts, bile duct ischemia,anastomotic technique failure, HAT, prior bile leak, autoimmune hepatitis, primary sclerosing cholangitis, or acute or chronic rejection[17,20,22,23,38,42-45]. The policy at our department on the use of donors ≥ 70 years was framed to prevent the aforementioned risk factors for BC, by performing a mandatory liver biopsy in all cases to discard livers with relevant histological alterations[29]. The use of hepatic artery pressure perfusion with low viscosity histidine-tryptophanketoglutarate preservation solution to improve peribiliary vascularization has been associated with lower rates of ischemic cholangiopathy[20]. This practice has been routinely performed in 207 of our LT, using Celsior solution as an alternative low viscosity solution. The use of older donors with a CIT longer than 13 h increases the risk of NABS[20], and it reduces the graft survival[5]. In our study, the median values of CIT were under 13 h in both groups and differences were not statistically significant (442 min in BCvs429 min in non-BC;P= 0.783).
A careful preservation of arterial vascularization of donor and recipient bile ducts is an important measure to avoid BC[44]. Small bile duct diameter constitutes a risk factor for ABS[23]. A sonographic study revealed that the upper normal limit size of the bile duct in the elderly population should be set at 8.5 mm[46]. In a LT series using liver grafts of a mean age of 55 years, the common bile duct diameter ranged between 6.8 mm and 7.1 mm[47]. The use of old liver grafts could facilitate the performance of the biliary anastomosis because of aging-associated progressive duct dilation.
The technique of biliary reconstruction using a T- tube has demonstrated a higher risk of BC, which has been attributed to a higher ABL rate[23,48]. In the same way, in our series the rate of BC was significantly higher among few patients who underwent choledocho-choledochostomy with a T-tube (two cases of ABS and one of ABL).
Patients with BC were diagnosed based on the clinical features and ultrasound/doppler and were confirmed by CT scan and PTC in the first era, and more recently by MRIC. Patients with ABL were diagnosed during the first 10 d post-LT, with an evolution to spontaneous closure in three patients and the remaining four requiring reoperation. In contrast,13 patients with ABS were diagnosed at a mean time of 12.2 mo post-LT (range: 1-38). While nine patients underwent an interventional therapy by PTC balloon dilation (1-6 times), eight underwent RYHJ. Alternatively, other authors prefer to use endoscopic retrograde cholangiopancreatography for ABS dilation[49]. Only three (14.3%) of our patients died because of BC (two recipients of septuagenarian livers and one recipient of an octogenarian liver).
We observed no significant differences in the patient and graft survival between the groups. In contrast, other authors have reported on the association between BC and significantly lower patient and graft survival[21,23,49]. Another series demonstrated an association between significantly lower patient and graft survival and more frequent incidence of NABS in recipients of octogenarian livers[38]. A different series using liver grafts younger and older than 75 years showed similar patient and graft survival between the groups, but a higher BC rate between the older group (29.6%vs13%)[11].
The most frequent causes of mortality in octogenarian liver recipients are cardiovascular disease, HCV or HCC recurrence, infection, and the development of de novo tumors[6,12,15,37], similar to our findings, and NABS[38]. As previously reported[30], the multivariate analysis identified female donors as a protective factor of BC owing to better pre-transplant liver function. However, donor cardiac arrest was a risk factor, as demonstrated in recipients of DCD livers suffering cardiac arrest[42,50].
This study had several limitations. We collected data retrospectively for a long duration and, subjected them to some biases typical for such studies.
CONCLUSION
In conclusion, the incidence of BC in our series was lower than others previously reported, and most cases could be managed by multidisciplinary approaches (percutaneous dilation or Roux-en-Y hepaticojejunostomy), which kept patient and graft survival unchanged. None of the patients with BC required re-transplantation. Female donor sex was a protective factor for BC, while donor cardiac arrest was a risk factor. The careful management of older liver grafts and meticulous anastomotic techniques can be associated with a low incidence of BC, confirming that livers older than 70 years are fine to use in LT.
ARTICLE HIGHLIGHTS
Research background
The shortage of liver grafts and subsequent waitlist mortality led us to expand the donor pool using liver grafts from older donors.
Research motivation
There are no studies analyzing the incidence and outcomes of biliary complications (BC) in patients older and younger than 70 years.
Research objectives
The aim of this study was to determine the incidence, outcomes, and risk factors for BC in liver transplantation (LT) using liver grafts from donors aged > 70 years.
Research methods
A retrospective case-control study was performed comparing patients who developed biliary complications with patients who did not after liver transplantation with donors ≥ 70 years.
Research results
Twenty-one patients (8.4%) developed biliary complications (13 anastomotic strictures, 7 biliary leakages, and 1 nonanastomotic biliary stricture). There were no significant differences in the patient and graft survival between the groups.Only three deaths were related to biliary complications. Female donors were protective factors for biliary complications and donor cardiac arrest was a risk factor.
Research conclusions
The incidence of biliary complications was relatively low on using liver grafts > 70 years.
Research perspectives
Prospective studies are necessary to confirm these results. It would be interesting to analyze the diameter of the bile duct and technical aspects when we perform the anastomosis.
FOOTNOTES
Author contributions:Jimenez-Romero C and Caso-Maestro O designed the research and wrote the paper; Jimenez-Romero C, Justo-Alonso I, san Román R and Caso-Maestro O analyzed data; Justo-Alonso I, del Pozo-Elso P, Marcacuzco-Quinto A, Manrique-Municio A,Calvo-Pulido J and García-Sesma A collected data; Martín-Arriscado-Arroba C peformed the statistical analysis.
Institutional review board statement:The study was reviewed and approved by the `12 de Octubre´ University Hospital Institution Review Board.
Informed consent statement:Patients were not required to give informed consent to the study because the analysis used anonymous data that were collected after each patient agreed to treatment by written consent.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:Technical appendix, statistical code, and dataset is available from the corresponding author if required.
STROBE statement:The authors have read the STROBE Statement—checklist of items, and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Spain
ORCID number:Carlos Jimenez-Romero 0000-0002-1965-0666; Iago Justo-Alonso 0000-0002-0553-5835; Pilar del Pozo-Elso 0000-0003-1793-1226; Alberto Marcacuzco-Quinto 0000-0001-6266-8792; Cristina Martín-Arriscado-Arroba 0000-0002-2147-2811; Alejandro Manrique-Municio 0000-0003-4758-9927; Jorge Calvo-Pulido 0000-0003-3144-4555; Alvaro García-Sesma 0000-0002-4377-7501; Ricardo San Román 0000-0001-8516-1978; Oscar Caso-Maestro 0000-0002-8953-269X.
Corresponding Author's Membership in Professional Societies:Asociacion Española de Cirujanos; Sociedad Española de Trasplante; Sociedad Española de Trasplante Hepático; and The Transplantation Society.
S-Editor:Gong ZM
L-Editor:A
P-Editor:Zhang YL
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Initial suction drainage decreases severe postoperative complications after pancreatic trauma: A cohort study
- Vascular complications of chronic pancreatitis and its management
- Historical changes in surgical strategy and complication management for hepatic cystic echinococcosis
- Goldilocks principle of minimally invasive surgery for gastric subepithelial tumors
- Prognosis after splenectomy plus pericardial devascularization vs transjugular intrahepatic portosystemic shunt for esophagogastric variceal bleeding
- Prognostic scores in primary biliary cholangitis patients with advanced disease