Initial suction drainage decreases severe postoperative complications after pancreatic trauma: A cohort study
2023-10-21KaiWeiLiKaiWangYuePengHuChaoYangYunXuanDengXinYuWangYuXiuLiuWeiQinLiWeiWeiDing
Kai-Wei Li, Kai Wang, Yue-Peng Hu, Chao Yang, Yun-Xuan Deng, Xin-Yu Wang, Yu-Xiu Liu, Wei-Qin Li, Wei-Wei Ding
Abstract
Key Words: Pancreatic trauma; Drainage; Postoperative complications; Clavien-Dindo; Propensity score matching
INTRODUCTION
Pancreatic trauma (PT) is relatively rare; however, injury to the pancreas can be challenging for even the most experienced trauma surgeon[1-3]. Significant morbidity and mortality are usually related to the cumulative effect of all injured organs[4]. Surgical management is nearly always adopted for PT in the emergency setting of abdominal trauma[5,6].
Consensus regarding the need for drainage has been formulated in many management strategies for PT[7-9]. The rationale is to evacuate intra-abdominal exudate, pancreatic juice or blood that can accumulate after surgery and serve as an early warning sign of possible pancreatic fistula, anastomotic fistula and associated hemorrhage[8-10]. Moreover,peripancreatic drainage alone is an important therapeutic measure[11,12]. The following two drain types are mainly placed for pancreatic surgery: Closed passive gravity (PG) drainage and sustained low negative pressure irrigation (NPI)suction drainage. PG drainage applies no pressure, evacuating fluid by gravity alone with intra-abdominal pressure[13].NPI suction drainage actively flushes the abdominal cavity with normal saline under low negative pressure[14,15]. In fact, high-level evidence has not yet been provided to support the choice of drain type for PT[16].
Several issues related to drainage are considered counterproductive, leading to constant evaluation of the roles of these methods[16,17]. First, the drains can serve as portals of entry for bacteria[18]. Second, fistula, hemorrhage, or holloworgan perforation can be caused by mechanical pressure, suction or erosion around the anastomosis and fragile tissue[19]. It is of paramount importance to understand the extent to which drains influence the development and severity of complications. Therefore, based on one of the largest PT populations in our high-volume center, we performed a retrospective study to investigate whether NPI is superior to PG drainage.
MATERIALS AND METHODS
We performed a retrospective cohort study of consecutive patients who underwent pancreatic surgery at a tertiary trauma referral center between January 2009 and October 2021 in our PT database. The study was approved by the Institutional Review Board (IRB) of Jinling Hospital (Approval No. 2021DZGZR-YBB-009). Informed consent was waived by the IRB because of the retrospective nature of the study. This study was conducted in accordance with the principles of the Declaration of Helsinki. The exclusion criteria were as follows: Early death (< 48 h) after admission; Glasgow Coma Scale score ≤ 8; Abbreviated Injury Scale score = 6 for any area of the body; nonoperative treatment; pregnancy status;and previous history of malignancy, immune system or hematological diseases.
Operative and drainage management
Pancreatic injuries are classified into 5 grades (Ⅰ-Ⅴ) according to the Organ Injury Scale, proposed by the American Association for the Surgery of Trauma in 1990. For low-grade PT (Ⅰ-Ⅱ), drainage alone was performed after complete exposure of the pancreas. For high-grade PT (Ⅲ-Ⅴ), distal pancreatectomy with or without splenectomy was usually adopted for grade III injury; debridement/resection of the area of injury, closure of the proximal stump and distal Rouxen-Y pancreaticojejunostomy or drainage alone was implemented for grade IV injury; and one-stage damage control drainage and subsequent definitive operative or pancreaticoduodenectomy was utilized for grade Ⅴ injury.
After distal pancreatectomy, a drain was insertedviathe left flank and was placed near the pancreatic remnant; the other drain was placed in the left subphrenic area, but only when splenectomy was performed. Similarly, a drain was insertedviathe left flank and was placed between the pancreaticojejunostomy and pancreatic remnant after middle pancreatectomy. After pancreatoduodenectomy, a drain was insertedviathe right flank and placed posterior to the biliary anastomosis, extending to the proximal margin of the pancreatic remnant. The other drain was insertedviathe left flank and was placed posterior to the stomach, extending to the posterior surface of the pancreatic anastomosis in proximity to the contralateral drain. In addition, individualized operative management was performed, and drains were placed as appropriate after careful assessment of the other intra-abdominal organs.
The two drain types adopted are shown in Figure 1. The decision regarding which drain type to place was made on a case-by-case basis and according to the surgeon's preference. Drains were routinely kept in situ for at least postoperative days (POD) 7 to 10. Computed tomography (CT) scans were performed every other week postoperatively. Once pancreatic fistula grade B/C or gastrointestinal fistula was confirmed by fistulography, the duration of drain placement was prolonged. For these patients, PG drainage was replaced by NPI suction drainage through the sinus tract for irrigation to minimize erosion of the surrounding tissue by the digestive juice. A controlled pancreaticocutaneous fistula or enterocutaneous fistula was created by retaining the catheter in situ until the fistula healed spontaneously. When necessary, a CT-guided percutaneous drainage procedure was performed in patients with local pancreatic complications after failed initial drainage and/or new-onset gastrointestinal fistula and localized intra-abdominal abscess requiring source control, and the PG drain was then replaced with NPI suction drainage following the guidewire.
We regularly replaced the catheter to maximize the effect of sustained irrigation drainage and reduce the size of the tube by degrees as appropriate. Two replacement strategies are employed for the management of NPI suction drainage in clinical practice: (1) Planned replacement for prophylactic drainage; and (2) On-demand replacement for therapeutic drainage. If patients do not develop pancreatic fistula grade B/C or gastrointestinal fistula and the volume of drainage fluid is decreasing, prophylactic NPI suction drainage is planned to be replaced every 3 d. For patients with pancreatic fistula grade B/C or gastrointestinal fistula, on-demand replacement is adopted because the role of NPI has been converted to therapeutic drainage. The catheter was retained in situ to create a controlled pancreaticocutaneous fistula or enterocutaneous fistula when there was a large volume of drainage fluid. In addition, the nature of the drainage fluid and the irrigation and drainage fluid in and out volume per unit of time were used to judge whether catheter blockage occurred. If blockage occurred, it was replaced promptly. Moreover, in the presence of a decreasing volumes of drainage fluid and no evidence of intra-abdominal infection, we switched the NPI suction drainage from on demand to planned replacement.
We adhered to the following drain removal policy: Lack of infection-induced systemic inflammatory response syndrome; pancreatic fistula defined by the International Study Group of Pancreatic Fistula was absent or grade A; the evidence provided by CT excluded intra-abdominal abscess or undrained fluid collections; drained fluid was less than 20 mL per day and turned clear; and lack of any gastrointestinal fistula. Additional management methods included the administration of antibiotics, supplemental parenteral or enteral nutrition, reinterventions (reoperation, endoscopic or interventional radiological procedures), and organ function support.
Study variables and outcomes
Data analyzed included demographics, vital signs, injury parameters, operative procedures, types and locations of drains,complications, reinterventions, bacterial culture information about drainage fluid samples, mortality and length of stay(LOS). The primary outcome was the occurrence of severe complications defined as Clavien-Dindo grade Ⅲb-Ⅴ during hospitalization. Further details on the definitions of outcome variables are provided in Supplementary Table 1.
Statistical analysis
Student’sttest and Wilcoxon’s rank sum test were used to compare normal or nonnormal continuous variables,respectively. The chi-square test and Fisher’s exact test were used to compare categorical variables. A multivariate logistic regression model was applied to evaluate the associations between the primary outcome and different drain types.Variables withP< 0.2 in the univariate test were included in the multivariate analysis.
To study effect modification by different drainage methods and to adjust for confounding factors, we performed sensitivity analysis based on propensity score matching (PSM). The PG group was matched 1:1 with the NPI group using their propensity scores with the nearest neighbor matching algorithm without replacement (the caliper was set at 0.2). A standardized mean difference (SMD) of less than 10% indicates appropriate balance. A univariable logistic regression model was adopted to estimate the odds ratio (OR) and corresponding 95% confidence interval (CI) for the primary outcome. Prespecified subgroup analyses were performed in the matched cohort to determine whether the effect of drainage varied across stratification factors of covariates. R software, version 4.0.3, was used for statistical analysis.
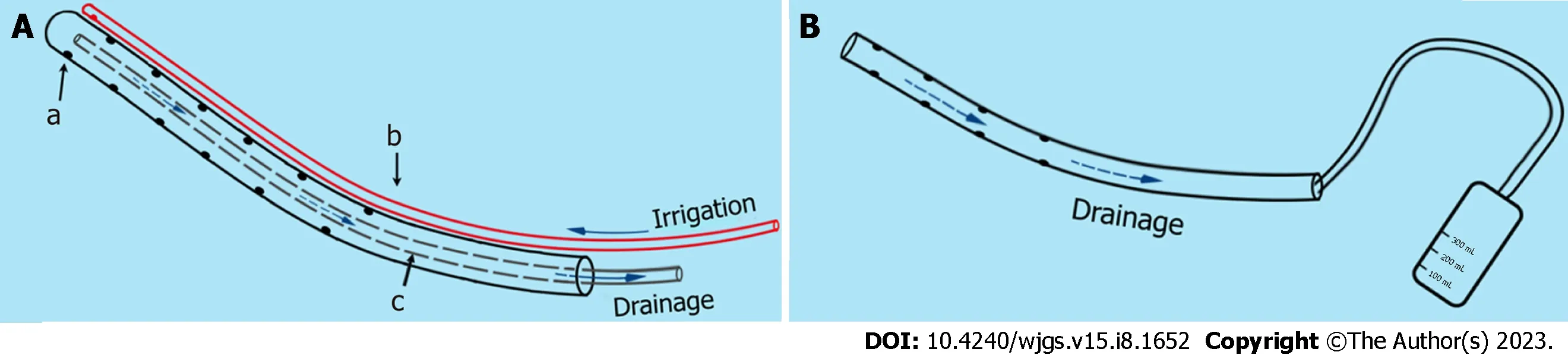
Figure 1 Sketch map of the negative pressure irrigation suction drainage and passive gravity drainage systems. A: Negative pressure irrigation suction drainage. A cranial margin closed the outer silicone cannula with a diameter between 24 French and 30 French, and multiple side apertures with diameters of 3-5 mm were arranged along the cannula (part a). A 12 French urinary catheter and the cranial margin are connected to part a with silk thread for continuous irrigation with sterile normal saline at a rate of 100 to 125 mL/h after surgery (part b). An inner silicone cannula without side aperture was placed into part a, with approximately half the diameter of part a, for connection to a low negative pressure (-10 kPa to -20 kPa) system[28] (part c); B: Passive gravity (PG) drainage.PG drainage is defined as a latex catheter drain that maintains a pathway for fluid to follow from the surgical site by gravity, connected to a liquid storage bag maintained at atmospheric pressure.
RESULTS
Patient characteristics
Two hundred thirteen PT patients were managed by operative management with drain placement during the study period. Of these patients, 196 met the inclusion criteria: 146 (74.5%) in the PG groupvs50 (25.5%) in the NPI group. The screening process is shown in Figure 2. The patients’ preoperative demographics, clinical characteristics and injury parameters are summarized in Table 1. In the entire cohort, the NPI group had less duodenum injury and more concomitant vascular injury (P< 0.05). Regarding the time from trauma to operation, delayed operative treatment (24 h)occurred more frequently in the NPI group (46.0%vs20.5%,P= 0.001).
PSM with a 1:1 ratio resulted in 88 patients (PG 44, NPI 44). Before PSM, 13 of 15 baseline characteristics were unequally distributed between the two groups; following PSM, all of the variables reached an SMD < 0.10 (Supplementary Figure 1), suggesting that the two matched cohorts were well balanced. In the matched cohort, the pancreatic injury grades and the extent of injury to intra-abdominal organs exhibited approximately proportional distributions (P>0.05) (Table 1). Moreover, the proportion of each operative procedure performed for pancreatic injury-related and other intra-abdominal organ injury-related cases was comparable in the matched cohort (Table 2).
Primary outcome
In the entire cohort, the incidence of severe complications in the NPI group was significantly lower than that in the PG group [14/50 (28.0%)vs66/146 (45.2%),P= 0.033] (Table 3). In univariate logistic regression analysis, injury severity score, abdominal abbreviated injury scale, isolated pancreatic injury, and different drain types were associated with severe complications (P< 0.05) (Supplementary Table 2). Notably, the NPI group was significantly less likely to develop severe complications (OR: 0.471; 95%CI: 0.235-0.947;P= 0.035). In multivariate analysis, the adjusted risk for severe complications was decreased in the NPI group (OR: 0.437; 95%CI: 0.203-0.940;P= 0.034) (Figure 3). After PSM, the results of the sensitivity analysis were consistent with those of the multivariate analysis (OR: 0.365; 95%CI: 0.148-0.901;P= 0.029)(Figure 3).
Secondary outcomes
Among the matched cohort, no significant difference in in-hospital mortality was observed between the two groups. The drainage period in the NPI group was shorter than that in the PG group [median (inter-quartile range), 35.0 (20.0-54.75)vs47.0 (30.0-68.0) d;P= 0.009]. The proportion of patients who underwent CT drainage in the NPI group was still significantly lower (15.9%vs34.1%,P= 0.042). Moreover, the NPI group was associated with a lower incidence of pancreatic fistula grade B/C, a lower incidence of gastrointestinal fistulas, a lower reoperation rate, and a shorter LOS (P< 0.05) (Table 3). The POD 7 infection rate of drainage fluid in the NPI group was significantly lower [11/36 (30.6%)vs27/43 (62.8%),P= 0.004] (Supplementary Table 3). With regard to the qualitative microbiological analysis, the incidence of G+ bacterial infection was higher in the NPI group [7/11 (63.6%)vs5/27 (18.5%),P= 0.017] (Supplementary Table 4).In this prespecified subgroup analysis, the difference in the rate of the primary outcome between the PG and the NPI group was greater among patients without concomitant vascular injury (Figure 4). We detected no significant interactions of treatment with the other baseline factorsP> 0.10 for all comparisons.
DISCUSSION
Few comparative studies have focused on the potential differences in the postoperative outcomes related to drain types for PT patients. Most western countries recommend closed suction drainage, but conclusive evidence is lacking[7-9,20].The Memphis group found that closed suction drainage reduced septic complications, while sump drainage causedretrograde infectionsviacatheters[21]. However, it is difficult to derive robust results from this study due to the heterogeneity of study participants, injury parameters, and operative procedures. In this study, we evaluated the severity of complications for different drain types after PT and found that NPI suction drainage is superior to PG drainage.

Table 1 Baseline characteristics of patients before and after matching
The reduced Clavien-Dindo severity for NPI suction drainage can be attributed to several factors. First, NPI suction drainage can effectively remove residual infection within intra-abdominal or between intestinal loops through continuous and active irrigation with sterile normal saline, thereby reducing the incidence of abscess, systemic inflammation orsepsis[22]. Second, NPI suction drainage can rapidly drain collected pancreatic juice by a low negative pressure system to reduce accumulation and diffusion, and it can dilute the accumulated fluid collection by irrigating sterile normal saline to minimize erosion and impairment to other tissues, thus preventing mild pancreatic leakage from developing into a serious pancreatic fistula and avoiding hemorrhage and the formation of gastrointestinal fistulas. Jianget al[15] verified that pancreatic fistula grade C in patients with NPI suction drainage was significantly less common than in patients with passive drainage after pancreaticoduodenectomy. Under dual effects, NPI suction drainage could achieve significant clinical benefits for patients. PG drainage generally relies on the pressure difference and gravity, which might not obtain adequate drainage and predispose patients to catheter blockage. In this study, the incidence of catheter blockage was 9.6% (14/146) in the PG group, whereas it did not occur in the NPI group.
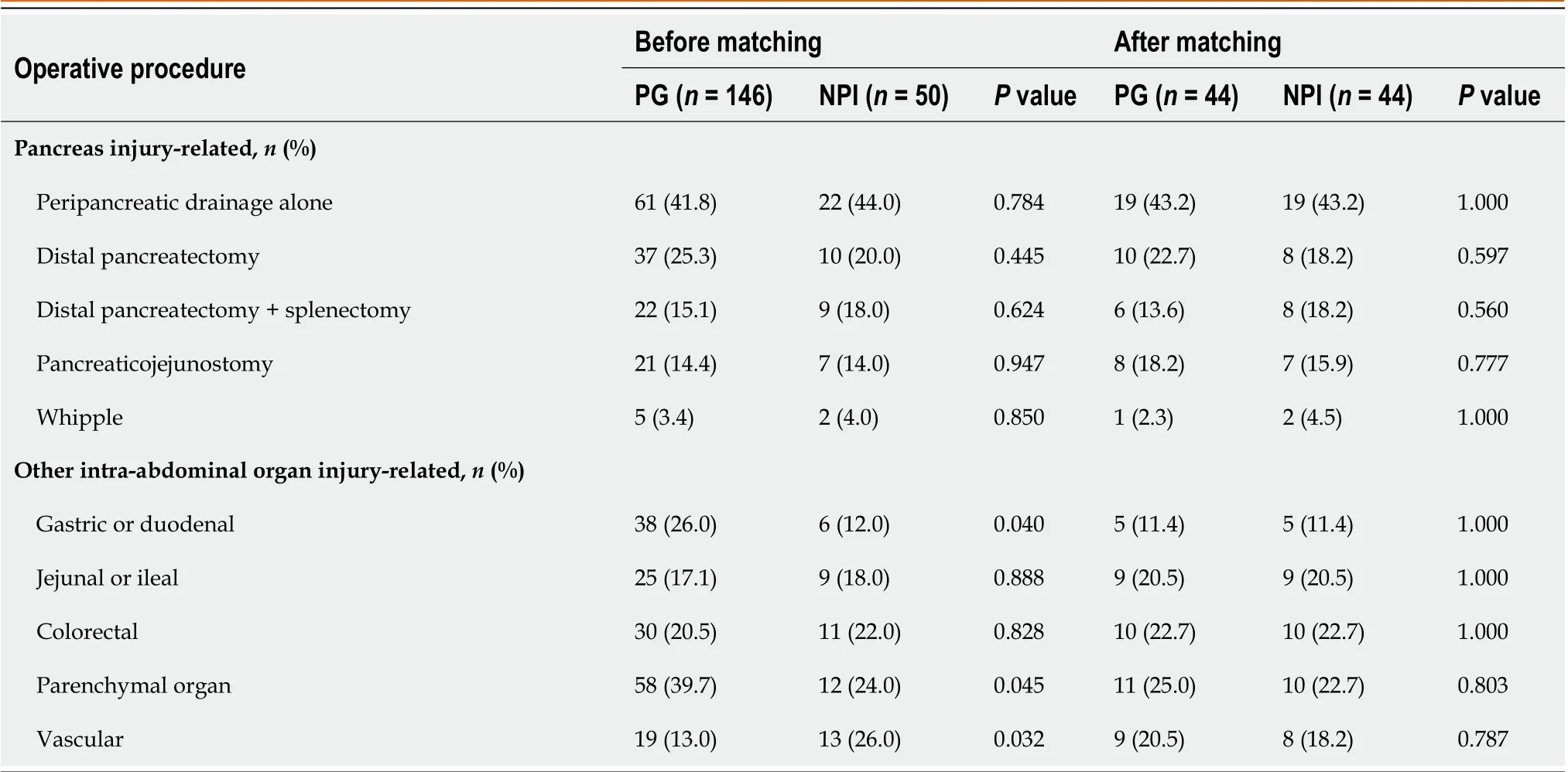
Table 2 Operative procedures between two drain types before and after matching cohorts
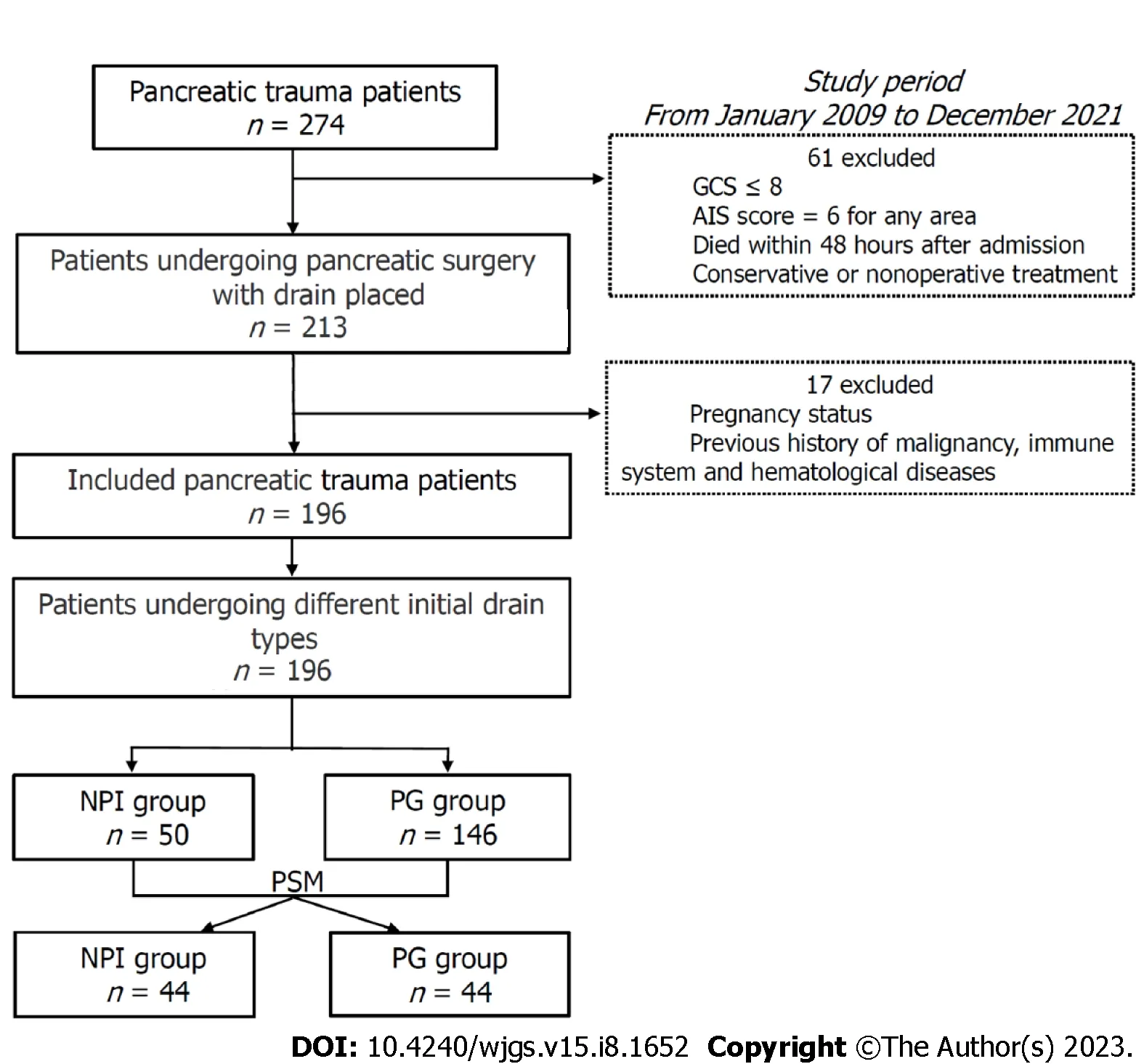
Figure 2 Flow chart of the patient selection process. GCS: Glasgow coma scale; AIS: Abbreviated injury scale; PG: Passive gravity; NPI: Negative pressure irrigation; PSM: Propensity score matching.
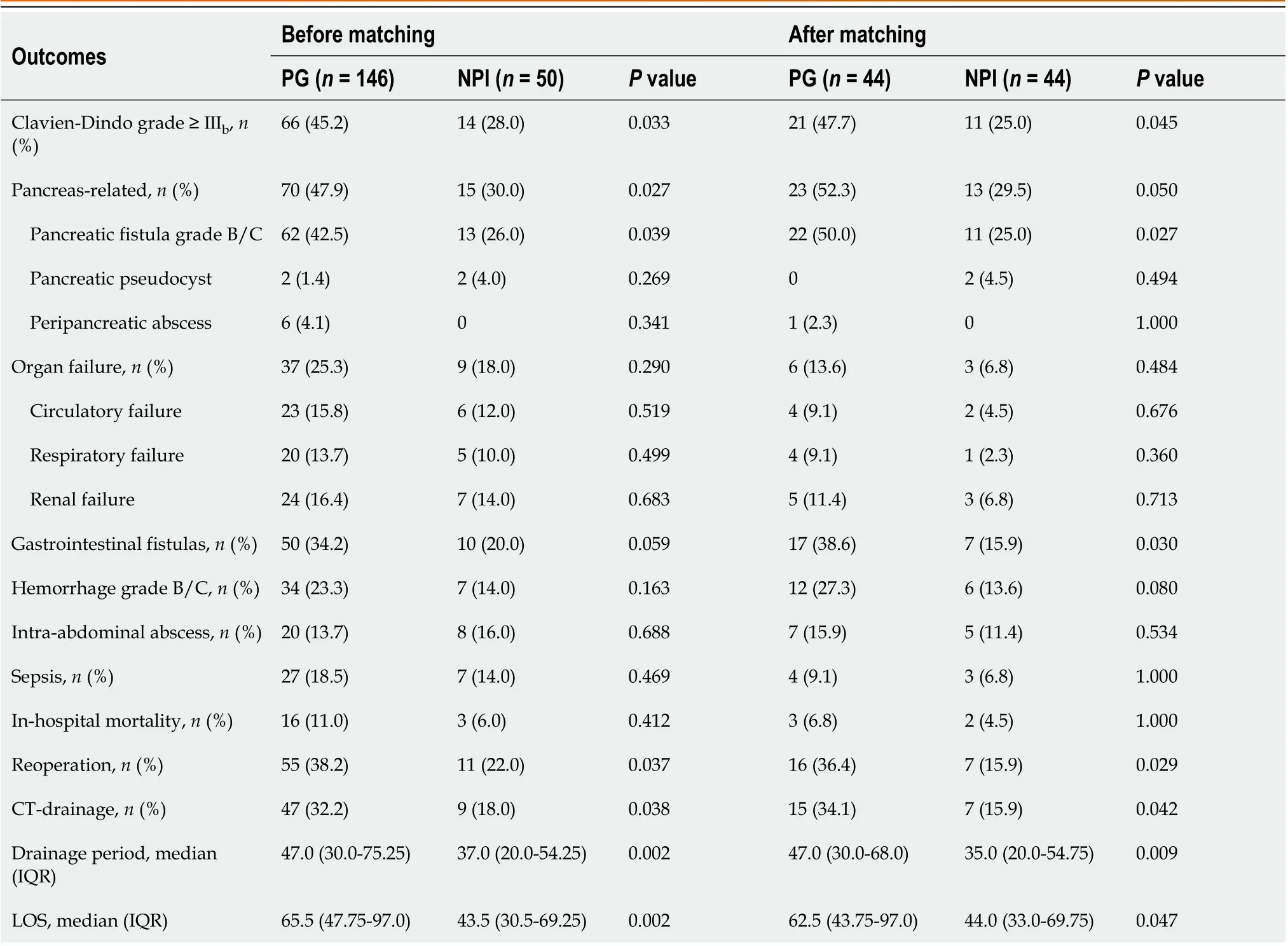
Table 3 Postoperative outcomes of passive gravity vs negative pressure irrigation group before and after matching cohorts
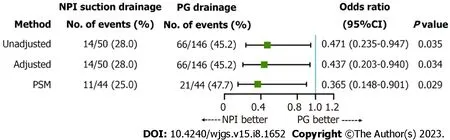
Figure 3 Events of severe complications for passive gravity vs negative pressure irrigation and sensitivity analysis results. Events of severe complications associated with different drain types are measured as those with a Clavien-Dindo grade ≥ IIIb. PG: Passive gravity; NPI: Negative pressure irrigation;Unadjusted: Univariate logistic regression model; Adjusted: Multivariate logistic regression model; PSM: Propensity score matching; CI: Confidence interval.
More importantly, postoperative digestive tract fistulas often contribute to various other complications, such as hemorrhage, sepsis, multisystem organ failure, and even death. These complications require reinterventions, such as percutaneous drainage or reoperation[23]. Nevertheless, resection and anastomoses should not be considered suitable procedures due to the edematous and friable nature of and adhesions adjacent to the fistula site. Fistulography is performed to evaluate the possibility of conservative treatment. For patients able to be treated conservatively, we uniformly adopted NPI suction drainage. The outer cannula can prevent both aspiration damage to surrounding tissues and blockage of the inner suction cannula. The patency provided by NPI suction drainage is a fundamental principle in the formation of a stable and controlled pancreaticocutaneous or enterocutaneous fistula, which is beneficial for facilitating the formation of the fistula tract[24].

Figure 4 Relative risk for the primary outcomes in prespecified subgroups. The forest plot presents, for each subgroup, the relative risk of severe complications between different drain types by a square and its 95% confidence interval (CI) by a horizontal line. On the left side of the figure, the subgroup sample size by drain type is presented with the corresponding severe complication rate. The right side of the figure lists the relative risk and its 95%CI; the x-axis of the plot is the risk estimate of severe complications. The last column shows the P values for relative risk interactions between subgroups. Subgroup-specific relative risk was derived from modified Poisson regression. PG: Passive gravity; NPI: Negative pressure irrigation; BMI: Body mass index; ISS: Injury severity score; CI: Confidence interval.
In the matched cohort, the incidence of gastrointestinal fistulas and the reoperation rate were higher in the PG group.Sixteen patients required reoperation for one or more intra-abdominal complications: Intra-abdominal hemorrhage grade B/C in 10 patients, small intestinal fistulas in 3, colonic fistulas in 5, pancreatic fistula grade C in 2, and infectious pancreatic necrosis in 2. Correspondingly, 7 patients required reoperation in the NPI group, due to intra-abdominal hemorrhage grade B/C in 1 patient, gastric fistula in 1, colonic fistulas in 3, and pancreatic fistula grade C in 3. For patients who underwent CT-guided percutaneous drainage, the proportion in the NPI group was significantly smaller than that in the PG group. From the above, it can be determined that patients in the NPI group could undergo fewer invasive reinterventions. Our previous study also found that 74 of 88 gastric and small intestinal fistulas (84.1%) and 21 of 72 colonic fistulas (29.2%) caused by acute pancreatitis could be cured by NPI suction drainage[25]. Some studies have shown that negative pressure contributes by causing local tissue and vascular damage in the area near the drain[26].However, Čečkaet al[17] found that the rates of pancreatic fistula, hemorrhage and overall morbidity were not different between closed suction and PG drainage after pancreatic resection. According to the results of our study, low negative pressure did not raise the above concerns.
The overall mortality rate was 9.6% (19/196): 18 patients died of sepsis and related multiple organ failure. Similarly,the Western Trauma Association Multicenter Trials Group on Pancreatic Injuries found that the mortality was 9.1% (79/872) in PT patients who underwent surgery[11,12]. In our matched cohort, no significant differences in mortality were observed. These patients might benefit from good control of the infected source, and most digestive tract fistulas usually heal spontaneously over time[27]. In addition, the improvement of care capacity for severe trauma, parenteral and enteral nutritional support, and effective anti-infection treatment also played important roles.
The POD 7 infection rate of drainage fluid in the NPI suction drainage group was significantly lower; however, the incidence of infectious complications (abscess and sepsis) was not significantly different between the two drain types.This finding could be attributed to antibiotic administration and the application of percutaneous drainage. We speculate that the higher incidence of G+ bacterial infection with NPI suction drainage might be related to the open nature of the drain or retrograde migration of bacteria. Although subgroup analyses were prespecified, this study was not adequately powered to assess the benefit of treatment. Patients without concomitant vascular injury appeared to benefit more from NPI suction drainage than those with vascular injury. Nevertheless, with the limitations of a relatively small sample size and retrospective nature, caution should be exercised in the interpretation of these results.
Our study has several limitations. First, as an observational study, the analyses are subject to selection bias, and residual unmeasured confounding might persist despite adjustment for a variety of known patient variables using PSM to approximate randomization. Second, conducting the study at a single high-volume center limits its generalizability.Third, the volume, microbiology, amylase concentrations of drainage fluid, trends over time and drainage catheter removal time were not included in our data; however, they might also reflect the potential differences between the two drain types.
CONCLUSION
In conclusion, we compared the incidence of severe postoperative complications between the PG and NPI groups and found that NPI suction drainage was associated with decreased Clavien-Dindo severity. These findings suggest that initial NPI suction drainage could be recommended as a safe and effective alternative for managing complex PT patients.Further randomized, controlled trials are warranted to validate these results.
ARTICLE HIGHLIGHTS
Research background
Consensus regarding the necessity for drainage has been formulated in the many management strategies for pancreatic trauma (PT).
Research motivation
Few studies have addressed the question of which drain types are more beneficial for PT patients.
Research objectives
To investigate whether sustained low negative pressure irrigation (NPI) suction drainage is superior to closed passive gravity (PG) drainage in PT patients.
Research methods
We performed a retrospective cohort study of consecutive patients who underwent pancreatic surgery at a tertiary trauma referral center between January 2009 and October 2021 in our PT database. The primary outcome was defined as the occurrence of severe complications (Clavien-Dindo grade ≥ Ⅲb). Multivariable logistic regression was used to model the primary outcome, and propensity score matching (PSM) was included in the regression-based sensitivity analysis.
Research results
In this study, 146 patients underwent initial PG drainage, and 50 underwent initial NPI suction drainage. In the entire cohort, a multivariable logistic regression model showed that the adjusted risk for severe complications was decreased with NPI suction drainage [14/50 (28.0%) vs 66/146 (45.2%); odds ratio (OR), 0.437; 95% confidence interval (CI): 0.203-0.940]. After 1:1 PSM, 44 matched pairs were identified. The proportion of each operative procedure performed for pancreatic injury-related and other intra-abdominal organ injury-related cases was comparable in the matched cohort.NPI suction drainage still showed a lower risk for severe complications [11/44 (25.0%) vs 21/44 (47.7%); OR: 0.365;95%CI: 0.148-0.901].
Research conclusions
Initial NPI suction drainage could be recommended as a safe and effective alternative for managing complex PT patients.
Research perspectives
Further randomized, controlled trials are warranted to validate these results.
FOOTNOTES
Author contributions:Li KW designed and performed the research and drafted the manuscript; Wang K, Yang C, Deng YX and Wang XY were involved in the literature search and data extraction; Li KW and Hu YP analyzed and interpreted the data; Ding WW, Liu YX and Li WQ supervised and reviewed the report.
Supported bythe Jinling Hospital Scientific Research Project, No. YYZD2021011 and No. 22JCYYZD1.
Institutional review board statement:This study protocol was approved by the Institutional Review Board of Jinling Hospital, No.2021DZGZR-YBB-009.
Informed consent statement:This is a retrospective study, and patients were not required to give informed consent for the study because the analysis used anonymous clinical data that were obtained after each patient agreed to treatment by written consent.
Conflict-of-interest statement:All authors read and approved the final manuscript and declared no conflicts of interest.
Data sharing statement:The original anonymous dataset is available upon request from the corresponding author at dingwei_nju@hotmail.com.
STROBE statement:The authors have read the STROBE Statement—checklist of items, and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution Non-Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Wei-Wei Ding 0000-0002-5026-689X.
S-Editor:Lin C
L-Editor:A
P-Editor:Zhang YL
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Is endoscopic mucosal resection-precutting superior to conventional methods for removing sessile colorectal polyps?
- Knowledge, attitude, and practice of monitoring early gastric cancer after endoscopic submucosal dissection
- Changing trends in gastric and colorectal cancer among surgical patients over 85 years old: A multicenter retrospective study, 2001-2021
- Enhanced recovery nursing and mental health education on postoperative recovery and mental health of laparoscopic liver resection
- Effects of ultrasound monitoring of gastric residual volume on feeding complications, caloric intake and prognosis of patients with severe mechanical ventilation
- Risk factors and their interactive effects on severe acute pancreatitis complicated with acute gastrointestinal injury