Transcatheter aortic valve implantation in a patient with anomalous right coronary artery originating from the left aortic sinus with interarterial course
2023-09-24LuChenWANGYanXiangLIUXiaoGangSUNWeiWANG
Lu-Chen WANG ,Yan-Xiang LIU ,Xiao-Gang SUN,Wei WANG
Department of Cardiovascular Surgery,Fuwai Hospital,National Center for Cardiovascular Diseases,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing,China
Recently,the utilization of transcatheter aortic valve implantation (TAVI) has gained increasing prevalence due to its expanding range of applications in managing symptomatic severe aortic stenosis (AS).Coronary obstruction,a life-threatening complication,has been reported to occur during and after TAVI at an incidence rate of 0.5%-1%.[1]In addition to shallow sinus of Valsalva (less than 30 mm),low coronary take-off (below 12 mm from annulus plane),and calcification of native valve leaflets over the coronary ostium,anomalous origins of coronary arteries and compression from expanded transcatheter heart valve have been shown to cause TAVI-associated coronary occlusion.[2,3]To successfully perform this procedure,careful consideration of the anatomical characteristics of the coronary arteries is crucial,particularly the coronary height and sinus depth,as well as the spatial relationship between the coronary artery and the implanted valve.Despite the increasing number of TAVI procedures being performed,scarcity of reports exists on TAVI procedures performed in patients with anomalous coronary arteries.This report describes a case study of an AS patient with an anomalous right coronary artery originating from the left coronary sinus with an interarterial course,who underwent a successful TAVI procedure.
An 80-year-old woman presented to our Cardiovascular Surgery Department with atypical chest pain and exertional dyspnea.Physical examination revealed a loud 4/6 systolic murmur related to the aortic valve.Transthoracic echocardiography showed a thickened and calcified aortic valve with severe AS (mean aortic valve gradient of 68 mmHg,aortic orifice area of 0.50 cm2,and left ventricular ejection fraction of 66.0%).The coronary computed tomography angiography (CCTA) revealed that the anomalous right coronary artery arose from the left aortic sinus and coursed between the two main arterial trunks (pulmonary artery and aorta) (Figure 1A).Specifically,the proximal right coronary artery exhibited a segment of 10.1 mm in length with a slit-like morphology,showing a 50% to 70% narrowing without an intramural course.The coronary distribution type observed was right coronary dominance.Additionally,measurements on CCTA revealed the dimensions of the sinus of Valsalva as 24.1 mm × 24.7 mm × 24.4 mm,while the mean diameter of the sinotubular junction was 22.2 mm.The mean diameters of the aortic annulus and left ventricular outflow tract were 21.4 mm and 21.6 mm,respectively.The take-off angle of the right coronary artery measured 21°.The distance from the left coronary ostia to the aortic annulus plane was measured to be 8.2 mm (Figure 1B).
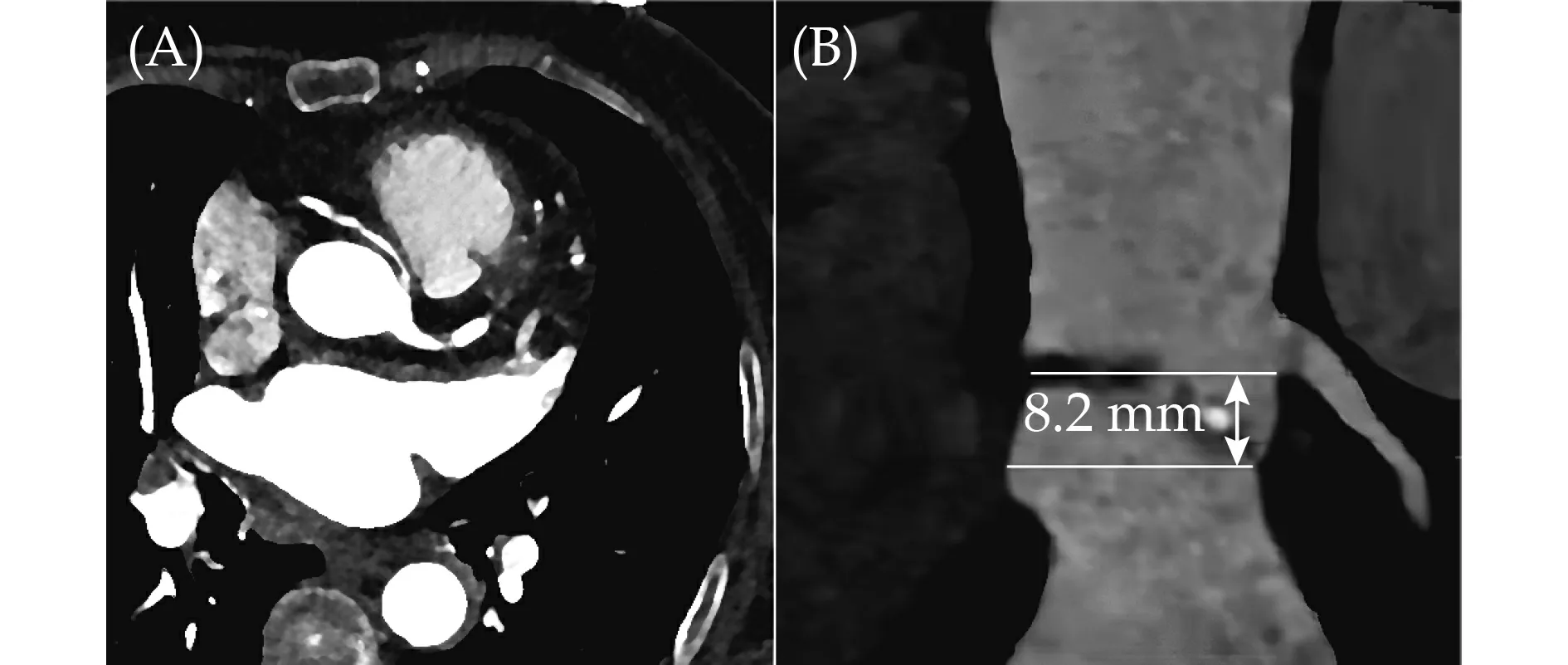
Figure 1 Preoperative evaluation of the patient. (A): The anomalous right coronary artery arised from the left aortic sinus with interarterial course;and (B): the height of the left coronary ostia was 8.2 mm.
The logistic EuroSCORE II was calculated to be 5.1%.In view of her wishes and the surgical risks,the heart team decided to perform a transfemoral TAVI procedure.After carefully evaluating preoperative imaging data and drawing from the team’s clinical experience,the surgeons opted to implant a 23 mm Venus-A valve (Venus MedTech,Hangzhou,China) via femoral access under general anesthesia.During the operation,a 20 mm balloon was employed for predilation.No significant alterations were observed in the coronary angiogram when compared to the root angiography phase (Figure 2A &2B).Finally,the position of the valve was confirmed by aortography,and the patency of the coronary arteries was also confirmed (Figure 2C).During the procedure,she was hemodynamically stable without ST-segment changes on electrocardiogram and ventricular wall motion abnormalities on transesophageal echocardiography.

Figure 2 Intraoperative assessment of the patient. (A): The coronary angiogram during the root angiography;(B): the annulus predilation by a balloon;and (C): the aortography after valve implantation.
Transthoracic echocardiography after TAVI also showed that the implanted aortic valve had a good function,without perivalvular leakage and local wall motion abnormality.
Anomalous right coronary artery arising from the left aortic sinus is reported to be more common than its leftsided counterpart,with an estimated incidence of 0.1% to 0.9%.[4]Angina,syncope,sudden cardiac death,and major adverse cardiovascular events have been significantly associated with anomalous right coronary arteries,especially those with interarterial courses.[5]One theory suggests that during exercise,when the aorta expands due to increased flow,the coronary artery between the aorta and the pulmonary artery may be compressed,resulting in blood flow blockage.
With the increasing utilization of TAVI,an augmented number of TAVI procedures will be performed on patients with anomalous origin of coronary arteries.Previous literature reports have documented coronary obstruction after TAVI.[3,6,7]However,the underlying mechanism of obstruction in anomalous origin of coronary arteries differs from that of a typical ostium obstruction,which usually results from a low coronary height and a shallow sinus of Valsalva.Instead,the obstruction in anomalous origin of coronary arteries is due to extrinsic compression resulting from expanding force,which causes narrowing of the coronary.This compression commonly occurs at the level of the aortic annulus.In this regard,the success of our case was mainly attributed to the anomalous right coronary artery being situated away from the annulus.Therefore,accurate analysis of the aortic root anatomy using CCTA to clarify the positional and spatial relationship of the coronary arteries and aortic annulus may predict the risk of coronary occlusion among patients with anomalous coronary arteries undergoing TAVI.Furthermore,comprehensive preoperative evaluation of the anomalous coronary arteries in proximal vessel morphology,the presence and length of the intramural course,the take-off type,angle,and level,as well as the proximal narrowing area and length,along with intraoperative balloon predilatation,represents vital components.
The present case report describes a TAVI procedure carried out on a patient diagnosed with severe AS and exhibiting an anomalous right coronary origin situated in the left aortic sinus,which ran between the pulmonary artery and aorta.To mitigate the risk of TAVI-related coronary occlusion,which can be caused by extrinsic compression from the expanding force exerted by the transcatheter heart valve,it is imperative to maintain a safe distance between the anomalous coronary ostia and the aortic annulus.This particular case highlights the possibility of performing TAVI in patients with anomalous coronary origins and emphasizes the significance of accurate preoperative assessment of the aortic root anatomy.
ACKNOWLEDGMENTS
All authors had no conflicts of interest to disclose.The authors are grateful to all the surgeons in the Department of Cardiovascular Surgery in Fuwai Hospital,National Center for Cardiovascular Diseases,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing,China.
杂志排行

Journal of Geriatric Cardiology的其它文章
- Prolonging dual antiplatelet therapy improves the long-term prognosis in patients with diabetes mellitus undergoing complex percutaneous coronary intervention
- Development and validation of a score predicting mortality for older patients with mitral regurgitation
- Age-related outcomes in patients with cardiogenic shock stratified by etiology
- Prognostic value of hematological parameters in older adult patients with acute coronary syndrome undergoing coronary intervention: a single centre prospective study
- The first experience of multi-gripper robot assisted percutaneous coronary intervention in complex coronary lesions
- Feasibility of emergent transcatheter aortic valve replacement sequentially followed by cardiac computed tomography angiography: experience from the procedure