Feasibility of emergent transcatheter aortic valve replacement sequentially followed by cardiac computed tomography angiography: experience from the procedure
2023-09-24DongKaiSHANBoJIANGZeYuSUNJingWANGYunDaiCHENChangFuLIU
Dong-Kai SHAN ,Bo JIANG ,Ze-Yu SUN,Jing WANG,Yun-Dai CHEN ,Chang-Fu LIU
Senior Department of Cardiology,the Sixth Medical Centre,Chinese PLA General Hospital,Beijing,China
Transcatheter aortic valve replacement (TAVR)has emerged as an effective alternative to surgical aortic valve replacement in symptomatic aortic stenosis (AS).[1,2]Approximately one in five cases of AS are emergent with acute decompensation of cardiac function;[3]therefore,emergent TAVR is an essential approach for severe AS patients with acute condition.[4,5]According to the Transcatheter Valve Therapy registry,an emergent state is defined as a situation that requires immediate aortic valve intervention due to continuous,intractable cardiac damage,with or without hemodynamic instability,and no response to any form of medication therapy except for cardiac intervention.[4]To date,although there are still some disputes about the indication of emergent TAVR,in clinical practice,it is an effective mean to save patients’ lives.
Conventionally,in emergent TAVR,the type of balloon predilation should be selected according to transesophageal echocardiography (TEE) assessment.Continuous balloon dilation can be performed to avoid circulatory instability caused by massive regurgitation if necessary;meanwhile,the type of artificial valve size is selected according to TEE and intraoperative aortic root angiography.However,there are still several limitations to this process,such as imprecise evaluation by TEE,which can cause a decrease in the device success rate.The acquisition and analysis program of cardiac computed tomography (CT) angiography (CTA) images has been standardized in selective TAVR,[6]because it is a possible way to acquire relatively accurate aortic root measurement data.However,thus far,there is no precedent for the application of cardiac CTA before emergency TAVR.In view of this,we have attempted to innovatively integrate cardiac CTA evaluation into the emergent TAVR workflow instead of TEE.Here,we show the preliminary experience of emergent TAVR and discuss the feasibility of emergent TAVR sequentially followed by cardiac CTA.Notably,this TAVR procedure was named emergent sequential CT-TAVR here.
From January 2019 to June 2022,there were 98 TAVR cases in Chinese PLA General Hospital,Beijing,China,of which three cases were introduced into the emergent sequential CT-TAVR procedure:
Case 1 A 77-year-old female with a history of diabetes mellitus and chronic obstructive pulmonary disease(COPD) was sent to the Emergency Department because of “chest tightness and shortness of breath after activity for more than three years and aggravation for more than half a month”,who was diagnosed with severe AS,and severe mitral regurgitation by emergent echocardiography.Her aortic effective orifice area was 0.4 cm2,and the mean pressure gradient was 89 mmHg.Because of recurrent refractory angina,emergent TAVR was planned after immediate cardiac CTA evaluation (Figure 1).Case 2 A 66-year-old male with a previous COPD history was delivered to the Emergency Department due to “intermittent chest tightness and shortness of breath for six years,aggravating for one year”.Echocardiography showed that his aortic valve had severe stenosis,while its effective orifice area was 0.5 cm2,and the mean pressure gradient was 61 mmHg.In addition,he had severe aortic valve regurgitation,severe mitral regurgitation,and severe tricuspid regurgitation.What made the condition worse,his left ventricular ejection fraction was 29% and suffered from symptoms of acute heart failure.After thoroughly evaluated,extracorporeal membrane oxygenation assisted circulatory support was introduced in emergency situations before emergent sequential CT-TAVR (Figure 2).
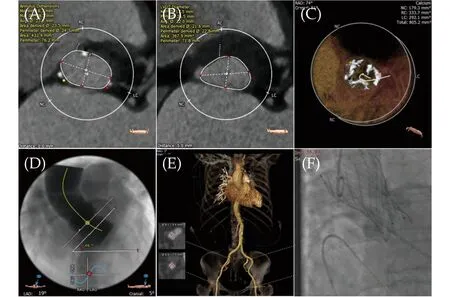
Figure 1 Preoperative computed tomography angiography annulus measurement,approach evaluation and final implantation presentation of emergent transcatheter aortic valve replacement of case 1. (A &B): Measurement of annulus and left ventricular outflow tract;(C): evaluation of calcification;(D): simulated angiographic angle of aortic valve implantation;(E): peripheral approach evaluation;and (F): final implantation presentation in angiography.

Figure 2 Preoperative computed tomography angiography annulus measurement,approach evaluation and final implantation presentation of emergent transcatheter aortic valve replacement of case 2. (A &B): Measurement of annulus and left ventricular outflow tract;(C): evaluation of calcification;(D): simulated angiographic angle of aortic valve implantation;(E): peripheral approach evaluation;and (F): final implantation presentation in angiography.
Case 3 An 84-year-old female with a history of hypertension for thirty years and a history of myocardial infarction and COPD,mainly due to “intermittent chest tightness and shortness of breath for more than five years,aggravating for one month”,was delivered to the Emergency Department.Echocardiographic examination showed that the aortic valve had extremely severe stenosis with an effective orifice area of 0.8 cm2,and the mean aortic valve pressure gradient was 42 mmHg.She had complex valvular diseases,including severe AS,slight aortic regurgitation,moderate to severe mitral regurgitation and slight tricuspid regurgitation.Because of her aggravated condition and persistent dyspnea,she was recommended to undergo emergent sequential CT-TAVR(Figure 3).

Figure 3 Preoperative computed tomography angiography annulus measurement,approach evaluation and final implantation presentation of emergent transcatheter aortic valve replacement of case 3. (A &B): Measurement of annulus and left ventricular outflow tract;(C): evaluation of calcification;(D): simulated angiographic angle of aortic valve implantation;(E): peripheral approach evaluation;and (F): final implantation presentation in angiography.
After urgent discussion and determination by a cardiac expert team,emergent sequential CT-TAVR was performed on the above three patients.With monitoring heart function and hemodynamic conditions,patients were transported to a CT-hybridized catheter room for cardiac CTA scanning.Interventional strategy planning by analysis of aortic root structure and peripheral vascular condition was implemented simultaneously.After evaluation of the anatomic structure,patients were referred for TAVR.
The protocol of cardiac enhanced CTA scanning for three patients was basically the same: the patient underwent CTA scanning using a second generation dualsource CT scanner.For the aortic root data,a retrospective electrocardiography-gated spiral scan protocol was used for data acquisition after the intravenous administration of a 50 mL contrast bolus.Moreover,an additional non-electrocardiography-gated large pitch enhanced scanning protocol acquisition of the entire aorta and iliac arteries was subsequently performed.Cardiac CTA imaging analysis was performed to determine the appropriate prosthesis type and intervention strategy.A prototype of now commercially available,automated analysis software 3mensio (Pie Medical Imaging,Maastricht,Netherlands) was used as previously reported.[7]Measurements of key parameters of aortic root structure were performed in a standardized fashion by experienced investigators.
After scanning and decision-making according to CTA analysis,TAVR was immediately carried out.All cases of TAVR were completed in a specially equipped hybrid interventional suite.After general anesthesia,arterial sheaths were passed through the transfemoral route,and a Lunderquist guidewire was used to establish the orbit.Aortic root angiography was used to precisely locate the expected implantation position,and the valve prosthesis was released under rapid ventricular pacing (160-200 beats/min) with a temporary pacemaker.The release system was withdrawn,and postimplantation angiography and TEE were used to assess valve position,function and paravalvular regurgitation.
After the operation,the symptoms of the patients were relieved to varying degrees,and the indicators basically normalized at the ninety-day visit.The key details of the TAVR intervention and the short-term prognosis of the three patients are listed in Table 1.

Table 1 Emergent sequential CT-TAVR information of three cases.
Acute decompensated heart failure or cardiogenic shock caused by severe AS usually indicates poor prognosis,and these patients are also at high risk of surgery.[8,9]Transcatheter intervention,such as emergent TAVR,provides an alternative treatment option for these high-risk patients.[10]For patients with cardiogenic shock or the acute stage of AS,emergent TAVR is a feasible strategy with an acceptable mortality.[4,11]Bongiovanni,et al.[5]reported that the success rate of emergent TAVR was 93.5% in a single center,the death rate was 3.3%,and the survival probabilities for thirty days and one year were 87% and 61%,respectively.To date,the results from the largest study,STS/ACC TVT registration,showed that in 64 emergent TAVR patients,the thirty-day and oneyear mortality rates were 8.7% and 29.1%,respectively.[4]
At present,clinical experience has proposed the following suggestions on the emergent TAVR process: for patients with unstable hemodynamics,mechanical circulatory assistance is recommended to avoid adverse events.The optimal approach is extracorporeal membrane oxygenation,while an intra-aortic balloon pump could be selected for secondary consideration.The femoral artery approach was the first choice for emergent TAVR.The aortic root structure should be evaluated by TEE in the emergent environment.[12]However,certain problems still exist in relying on TEE alone to guide this procedure.Firstly,interventional procedures guided by echocardiography may lead to imprecise measurement of the valve parameter,resulting in undersized valve selection,especially for oval annuli,[12]such as case 2 (annular diameter by echocardiography was 22 mm,but by cardiac CTA it was 29.4 mm).Secondly,echocardiography is not sensitive enough to assess the leaflets or annuls calcification,which may lead to inaccurate implantation position and postoperative conduction disturbances and leakage complications.Moreover,it is generally insufficient to assess coronary artery ostium heights by echocardiography,which may result in an increased risk of coronary artery ostium occlusion.Last but not least,the peripheral arteries cannot be evaluated accurately without CTA,which may cause increasing perioperative vascular complications,such as difficulty in prosthesis delivery,dissection and hematoma.
After preoperative cardiac CTA evaluation,more accurate analysis can be made according to the structure of the valve annulus and leaflet calcification,while the annulus size and prosthesis release position can be identified more precisely than TEE,so intervention can obtain a better hemodynamic effect and avoid complications.[6]For instance,in case 1,a small supravalvular structure and obvious calcification were evaluated by cardiac CTA,which indicates that downsizing the prosthesis to 23 mm(annular diameter) may be suitable.In case 2,although the valve annulus was large enough to contain a 29 mm prosthesis,the patient’s aortic valve was a type 0 bicuspid valve with extremely severe calcification on both the annulus and leaflets.Therefore,downsizing to a 27 mm prosthesis valve was acceptable.As a result,an ideal immediate effect after the intervention was observed.Meanwhile,this procedure did not increase the patient’s creatinine value,but it is still worth noting that for patients with severe renal insufficiency,adequate hydration after surgery is necessary.
However,it should be mentioned that increased preoperative and procedure time,as well,contrast agent and radiation exposure were inevitable when using CTA.Therefore,it is necessary for the cardiac expert team to cooperate tightly to reduce unnecessary preoperative time.In our center,the preliminary experience was that 20-30 min was appropriate for transporting patients from the CT department to the catheterization room.In fact,the shorter the transport time is,the better the operation effect.Admittedly,the distribution of CT and catheter departments in each medical center is different,and the collaboration process may need to be explored individually.If there is no CT-hybridized catheter room,or the distance between the CT room and interventional catheter room is too far,or the transport time is over more than 30 min,it should be carefully assessed whether to initiate the procedure.What is expected is that with the development of artificial intelligence imaging technology,the application of intelligent evaluation systems will lead to a greater reduction in the time of CTA image analysis because of the reduction in manual plotting and adjustment,making cardiac CTA analysis easier.Furthermore,based on the fact that patients undergoing emergent TAVR had higher rates of acute kidney injury and new dialysis,[4]it is essential to estimate the potential risk of contrast agent before starting this procedure.According to our imaging acquisition experience,the dosage of contrast agent in pre-TAVR CTA was 60-80 mL according to the patient’s weight.The flowchart of emergent sequential CT-TAVR is illustrated in Figure 4.

Figure 4 Flowchart of emergent sequential CT-TAVR.CT: computed tomography;TAVR: transcatheter aortic valve replacement.
It should be noted that emergent TAVR under echocardiogram guidance is still an effective approach to save the lives of patients who are undergoing cardiopulmonary resuscitation or life-threatening situations,and it is still the first choice currently for medical centers that have difficulty implementing preoperative cardiac CTA scanning.
Based on preliminary exploration,cardiac CTA evaluation could be conducted for patients for emergent TAVR in CT-hybridized catheter rooms.Cardiac CTA can quickly and safely acquire image data and can be transmitted to the background for analysis,and its measured accuracy is higher than that of echocardiography,which is beneficial for the expert team to quickly implement operative planning and valve prosthesis implantation.This is the first report of this sequential imaging procedure for emergent TAVR,and the interventional attempt for this emergent situation may be feasible and effective.However,this emergent sequential CT-TAVR procedure needs to be further verified with a larger sample size.
For patients with decompensated and unstable hemodynamic severe AS,emergent TAVR may be a feasible option.If patients’ conditions are allowed and cardiac CTA is available,it is safe and effective to choose the initial emergent sequential CT-TAVR procedure.
ACKNOWLEDGMENTS
This study was supported by the National Key Research and Development Program of China (2016YFC1 300304),the Logistic Health Care Program (21BJZ33),and the Youth Independent Innovation Science Fund of Chinese PLA General Hospital (22QNCZ024).All authors had no conflicts of interest to disclose.
杂志排行
Journal of Geriatric Cardiology的其它文章
- Prolonging dual antiplatelet therapy improves the long-term prognosis in patients with diabetes mellitus undergoing complex percutaneous coronary intervention
- Development and validation of a score predicting mortality for older patients with mitral regurgitation
- Age-related outcomes in patients with cardiogenic shock stratified by etiology
- Prognostic value of hematological parameters in older adult patients with acute coronary syndrome undergoing coronary intervention: a single centre prospective study
- Transcatheter aortic valve implantation in a patient with anomalous right coronary artery originating from the left aortic sinus with interarterial course
- The first experience of multi-gripper robot assisted percutaneous coronary intervention in complex coronary lesions