Economic Evaluation of Gastroscopy for Detecting Gastric Cancer in Chinese Natural Population
2022-12-30LiuYuhanSunLihua
Liu Yuhan,Sun Lihua
(School of Business Administration,Shenyang Pharmaceutical University,Shenyang 110016,China)
Abstract Objective To evaluate the economy of detecting gastric cancer by electronic gastroscope in Chinese natural population of different ages and genders.Methods A Markov model was constructed for the population,including both men and women of different ages.The model cycle was one year and the simulation time was 60 years.The cost-effectiveness of electronic gastroscopy in detecting gastric cancer of general population in China was analyzed from the perspective of the whole society,and the stability of the results was verified by sensitivity analysis.Results and Conclusion For the general population,the incremental cost-effectiveness ratio (ICER)of gastric cancer screening from the age of 50 is 50 143 yuan/QALY (quality-adjusted life-year),which is less than two times of per capita gross domestic product (GDP) compared with the screening from the age of 55.For men who start gastric cancer screening at the age of 50,the ICER is 38 525 yuan/QALY,which is less than two times of per capita GDP,and it is economical.For women who start the screening from the age of 55,the ICER is 47 814 yuan/QALY,which is less than two times of per capita GDP,so it is economical.The results of sensitivity analysis are consistent with the conclusions of basic analysis,and the results of basic analysis are stable.For the general population,it is more economical to start gastric cancer screening from the age of 50,while for men and women,it is more economical to start gastric cancer screening from the age of 50 and 55,respectively.
Keywords: gastroscope;gastric cancer;screening;cost-utility;health economic evaluation
Gastric cancer is the fifth most common malignant tumor and the third leading cause of cancer death in the world.Its advanced prognosis is relatively poor,which seriously threatens human health[1].Regarding the incidence rate,Asia is a region with a high incidence of gastric cancer.Among Asian countries,the incidence of gastric cancer in China,Japan,and South Korea is greater than 30/100 000,which is much higher than other Asian countries[2].In terms of survival rate,the 5-year survival rate is the standard for the clinical cure rate of gastric cancer,which means that within five years after treatment,if no visible metastasis or recurrence is found,it is regarded as clinically cured.After that,the probability of tumor recurrence and metastasis drops below 10%,and the patient can basically achieve long-term survival[3].The five-year survival rate of gastric cancer is closely related to the timing of diagnosis and treatment.After receiving treatment for early gastric cancer,the 5-year survival rate can reach 80%.While even if advanced gastric cancer undergoes surgical treatment,the 5-year survival rate is still less than 30%[4].Japan and South Korea,which are also countries with a high incidence of gastric cancer,have a government-funded gastric cancer screening program.By 2009,the early gastric cancer detection rate in Japan and South Korea had increased to 50%[5].Therefore,the 5-year survival rate for gastric cancer in Japan and South Korea is 64.6%and 71.5%,respectively.However,the 5-year survival rate for gastric cancer in China in the same year is only 35.9%,and the early detection rate is less than 10%[6,7].Combined with the high incidence of gastric cancer and the large population base in China,gastric cancer has become one of the leading tumors that seriously endanger people’s lives and health[8].It is estimated that in 2015,about 498 000 Chinese died of gastric cancer,about 1 364 people died every day.The morbidity and mortality of gastric cancer are both the second highest among malignant tumors in China.42.6% of gastric cancer cases and 45.0% of gastric cancer deaths worldwide occurred in China[9].The “Healthy China Action-Cancer Prevention and Control Implementation Plan (2019-2022)” proposes that the government should promote early cancer screening,early diagnosis,and early treatment strategies with wider coverage so that we can achieve 55% of early diagnosis rate of malignant tumors.Therefore,the implementation of early gastric cancer screening in the public is a feasible and efficient way to change the severe situation of gastric cancer diagnosis and treatment in China.However,large-scale cancer screening projects often bring a large economic burden to national medical insurance funds.Currently,China has no relevant research on the economics of gastric cancer screening for its populations,which cannot effectively support the government’s decisionmaking on technology choices.From the perspective of the whole population,this study analyzed the cost and utility of gastric cancer screening strategies through electronic gastroscopy by establishing a Markov model,and provided recommendations for the selection of gastric cancer screening programs in China.
1 Materials and methods
1.1 Markov model
As the incidence and mortality of gastric cancer in Chinese population has gradually increased from around 40 years old,the later the initial age of screening,the higher the incidence rate,and the lower the cost of each gastric cancer patient screened.However,the increase in the starting age of screening has also led to a decrease in the number of target populations.Considering that different initial screening ages have a greater impact on the economics of screening,this study analyzed the different initial screening ages from 40 to 80 years old.Therefore,the target population of this study is the different age groups in China without history and symptoms of gastric cancer.
The Markov model was established based on published literature[10].In this study,based on the possible results of screening and the natural history of gastric cancer,the Markov model divided the target population into seven groups: False positive,false negative,gastric cancer stage I,and gastric cancer stage II,Gastric cancer stage III,gastric cancer stage IV,and death (Fig.1).After the target population is screened by electronic gastroscope,according to the sensitivity and specificity of electronic gastroscope,it will be transferred to false negative and false positive probability with different probability.Although the population in the false positive group does not suffer from gastric cancer,they have spent the inspection fees for subsequent diagnosis and can return to the target population group in the next round of screening.People in the false negative group have already suffered from gastric cancer,but they have not been diagnosed.Therefore,in the next round of examination,they cannot return to the target population group.Due to the delay of the disease,and considering the rapid progress of gastric cancer,this study assumes that the population in this group will be screened out according to the proportion of people who are not screened[11].The total number of gastric cancer patients in the entire cohort is calculated from the incidence rate of corresponding age groups.Gastric cancer patients diagnosed in false positive and target population status will be transferred to each stage of gastric cancer status according to the planned screening population ratio.
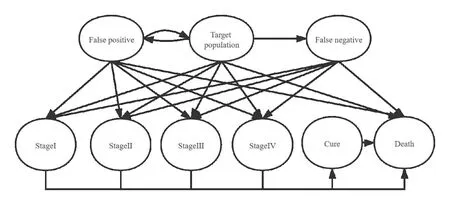
Fig.1 Markov model structure
The proportion of people planning to be examined in this study comes from the annual gastric cancer screening program in Japan.Therefore,this study sets the cycle length of the model to 1 year.Meanwhile,considering that the incidence of gastric cancer in men is twice as much as women,and then men and women are simulated separately[12].Since the incidence of gastric cancer increases with age,reaching a peak at 80 years old,if the average age of 77 is used as the study cut-off age,the difference between the two programs cannot be fully reflected.Therefore,the time limit of this study is set to 60 years,and it is simulated that 99% of the population enters a state of death.
1.2 Data sources
All-cause mortality and gastric cancer mortality of the target population in this study are from the“2019 China Health Statistics Yearbook”,and the incidence of gastric cancer is from the 2014 China Cancer Registry[13].The five years survival rate of gastric cancer patients in each stage and the proportion of non-screened populations in each phase are from the research conclusions of 1 503 patients in the Cancer Center of Sun Yat-sen University[14],and the probability of metastasis in each phase is obtained from the survival curve through the Getdate software.The data on the detection ratio of the planned population comes from the results of two Japanese gastric cancer screening projects in 1996 and 2000,and the final detection ratio is calculated by weighting[15,16](Table 1).The costs of gastroscopy detection,pathological biopsy and treatment for patients with gastric cancer in each stage come from five tertiary hospitals in Xuzhou,Jiangsu Province in 2015.All costs are converted to 2020 values by using China’s health care consumer price index (CPI)[17].Among them,patients with stage I-III gastric cancer are mostly treated with surgery,while patients with stage IV gastric cancer are mostly treated with palliative therapies,so the treatment cost of patients with stage IV gastric cancer is lower than that of stage I-III.The utility data comes from a multi-center clinical study for gastric cancer screening conducted in China in 2015,which measured the health utility value of 140 000 people with stage I to IV gastric cancer through the EQ-5D questionnaire[18].This study is a long-term simulation,so a 5% discount rate is used (Table 2).
2 Results and analysis
2.1 Cost-utility analysis
No matter from the perspective of the general population or the male or female population,the cost and utility of gastroscopy screening are increasing as the initial screening age continues to advance.Compared with women,men have a higher incidence of gastric cancer.Therefore,at the same initial screening age,the ICER of men’s gastroscopy screening is lower than that of women.The World Health Organization recommends that the threshold of willingness to pay should be 1 to 3 times of the gross domestic product (GDP) per capita[19].Based on this,the model results are analyzed (Table 3).
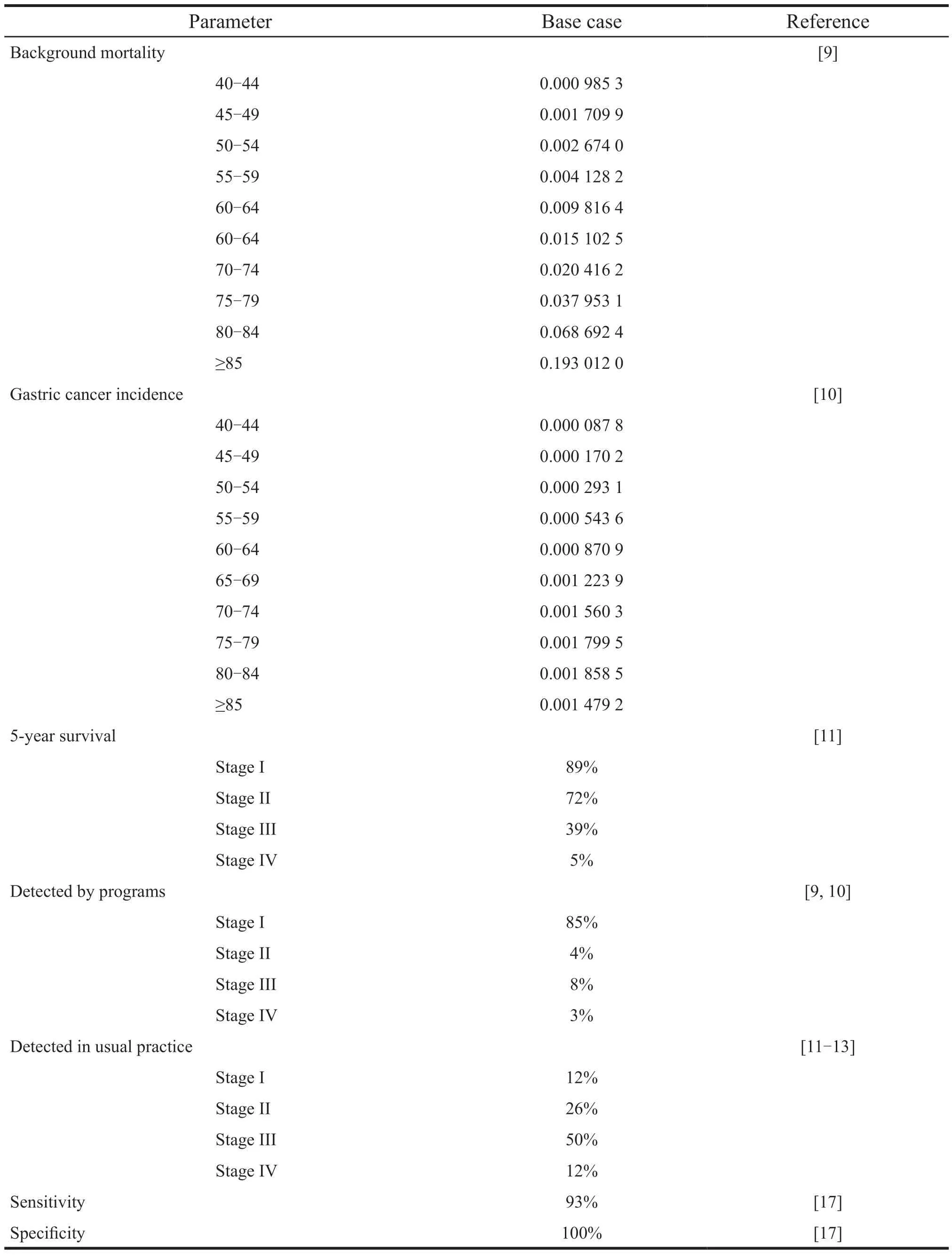
Table 1 Epidemiologic data
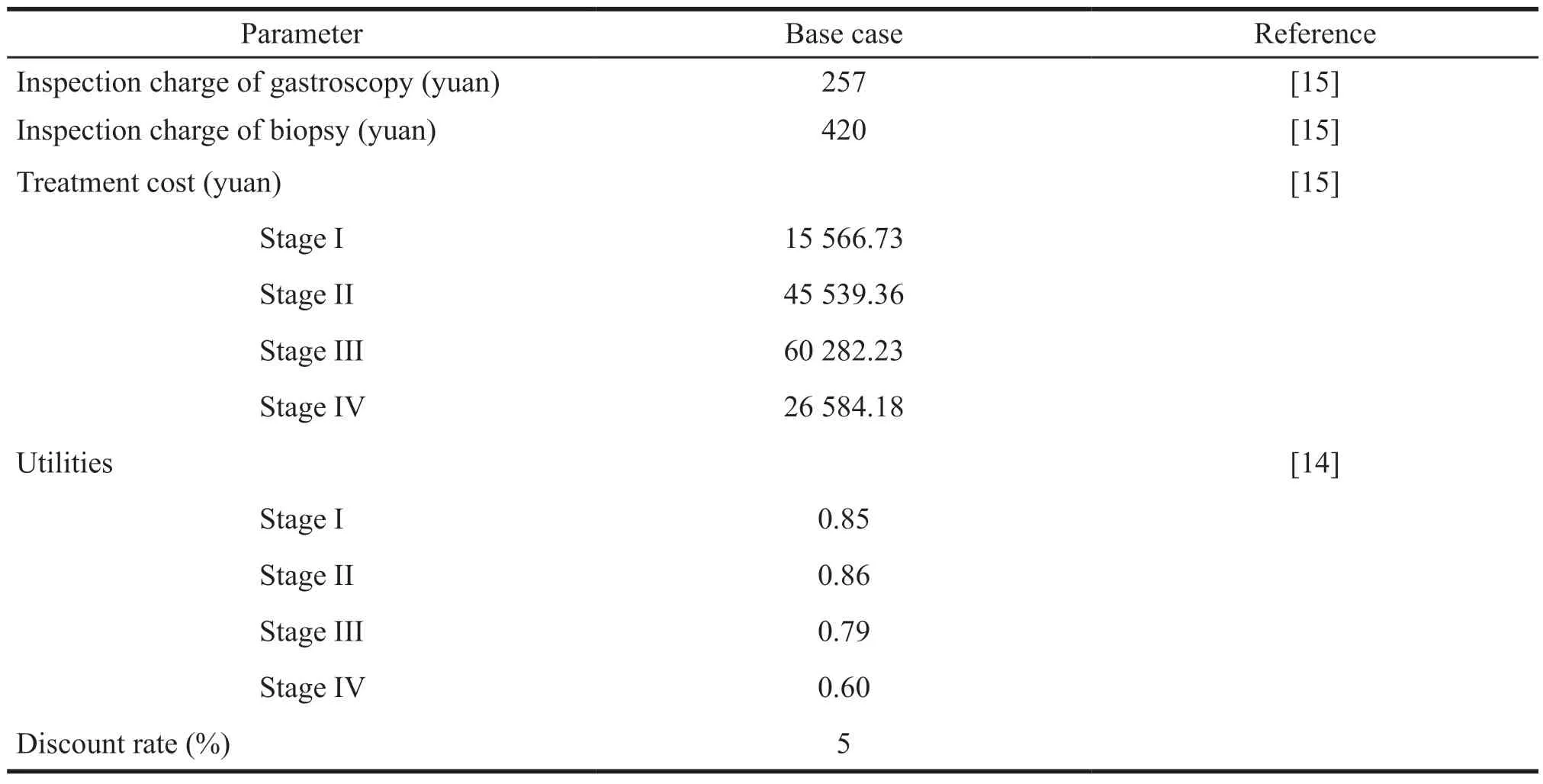
Table 2 Cost parameters and Utilities
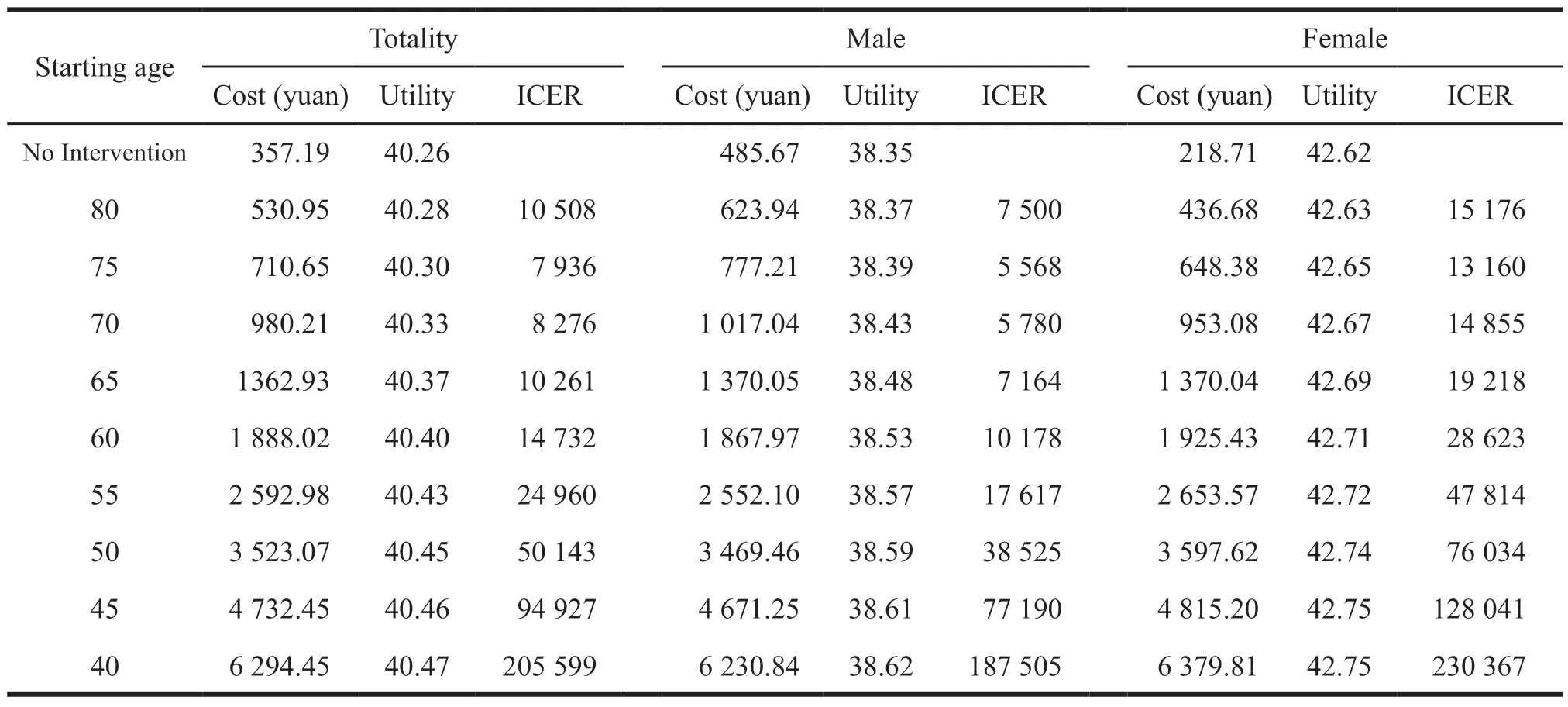
Table 3 Results of basic analysis
In 2019,China’s GDP per capita is 70 892 yuan.The results of the cost-utility analysis for different target groups are as follows.
(1) The schemes with ICER value less than two times of per capita GDP are for the general population to be screened for gastric cancer from the age of 50,men from the age of 50,and women from the age of 55.ICER is 0.71,0.54 and 0.67 times of GDP per capita in 2019,respectively.The above three schemes are economical.
(2) The schemes with ICER values between 2 and 3 times of per capita GDP are for the general population with gastric cancer screening from 45 and 40 years old,men from 45 and 40 years old,and women from 50 and 55 years old.The ICER for general population with gastric cancer screening at the age of 45 and 40 are 1.33 and 2.90 times of China’s per capita GDP in 2019,respectively.The ICER men starting at age 45 and 40 are 1.08 and 2.64 times of China’s per capita GDP in 2019,respectively.The ICER for women to be screened for gastric cancer from the age of 50 and 45 are 1.07 and 1.81 times of 2019 per capita GDP,respectively.
(3) If the ICER value is greater than 3 times of per capita GDP,women should be screened for gastric cancer from the age of 40,which is 3.24 times of China’s per capita GDP in 2019,and it is not economical.
2.2 Single factor sensitivity analysis
Based on the above analysis,this study will conduct single factor sensitivity analysis on three screening schemes,namely,screening at the age of 50 in the population with ICER less than 2 times of GDP per capita,screening for male at the age of 50,and screening for female at the age of 55.In this study,the cost of gastroscopy screening,the cost of treatment for stage I,II,III and IV gastric cancer and the utility parameters are raised by 20% and lowered by 20%,and the discount rate is raised to 8% and lowered to 0,respectively.Then,the sensitivity analysis is conducted(Table 4).
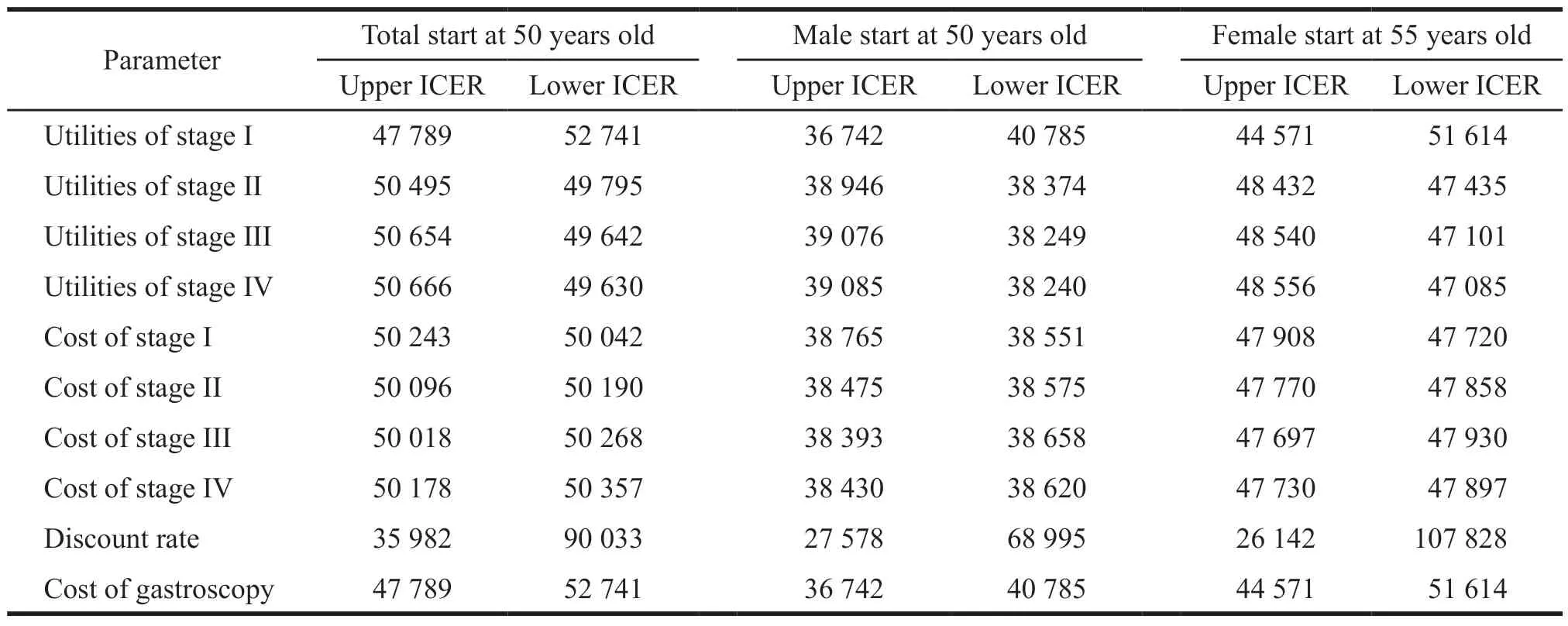
Table 4 Results of single factor sensitivity analysis
It can be seen from Table 4 that among the three schemes,the discount rate,the cost of gastroscopy screening,and the utility value of gastric cancer stage I have a greater impact on the ICER results.In the program targeting the general population and the female population,when all other factors except the discount rate change within its adjustment range,the incremental cost-utility ratio is less than 2 times per capita GDP in 2019,which is consistent with the basic analysis.In the plan that targets males,when all factors change within the adjustment range,the incremental cost-utility ratio is less than 2 times per capita GDP in 2019,which is consistent with the results of the basic analysis.
2.3 Probabilistic sensitivity analysis
This study conducted a probabilistic sensitivity analysis on the epidemiological parameters,cost parameters,and utility parameters of the above three programs.According to Monte Carlo simulation,the sampling is repeated 10 000 times,and the costeffectiveness acceptability curve is obtained (Fig.2).It can be seen from Fig.2 that for the general population,when the willingness to pay is 2 times per capita GDP,the probability of performing gastroscopy screening once a year from the age of 50 is 59%.For the male group,when the willingness to pay is 2 times per capita GDP,the probability to perform gastroscopy screening once a year from the age of 50 is 91%,and it is economical.For the female group,when the willingness to pay is 2 times per capita GDP,the probability to perform gastroscopy screening once a year from the age of 55 is 88%,and it is economical.
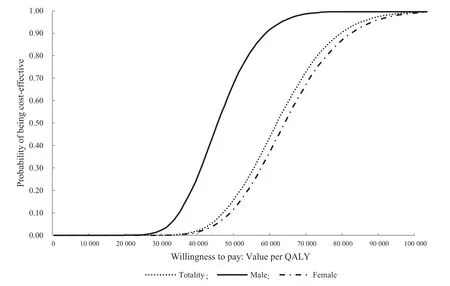
Fig.2 Probabilistic sensitivity analysis results
3 Conclusion and discussion
This study simulates different screening strategies and calculates the incremental costutility ratio.It is found that the ICER of gastroscopy screening for general populations starting from 50 years old is 50 143 yuan/QALY,which is less than 2 times per capita GDP,and it is economical.The results of the probabilistic sensitivity analysis show that when the willingness to pay is 2 times per capita GDP,the acceptance probability is 63%.If men and women in the general population start gastric cancer screening at the age of 50 and 55,respectively,the incremental cost-utility ratios are 38 525 yuan/QALY and 47 814 yuan/QALY,respectively.Besides,the willingness to pay is 2 times per capita GDP,the acceptance probability of probabilistic sensitivity analysis is 92% and 88% respectively.The results of single factor sensitivity analysis show that for the three options,the discount rate,gastroscopy screening cost,and gastric cancer phase I utility value have a greater impact on the ICER.Except for the discount rate,the other factors will increase when they change within the adjustment range,The cost-utility ratios are all less than 2 times per capita GDP in 2019,which is consistent with the results of the basic analysis.
There are still some limitations in this study.At present,there is no domestic practice for gastric cancer screening,and individual parameters of the Markov model can only be obtained from foreign literature.And because there is no research showing the difference between the annual screening and the screening every 2 to 3 years,this study only simulates the most common situation,and the screening is carried out once a year.At the same time,from the practice of Japan and South Korea,the compliance of the research objects cannot reach 100%,it is difficult to simulate the complex reality through the model.In addition,since there are a few studies on the burden of gastric cancer in China,this study only takes direct medical costs into consideration.In the future,relevant research can be carried out to obtain more detailed data to reduce the influence of the above biases on the research results.
杂志排行
亚洲社会药学杂志的其它文章
- Information for Authors
- Reflections on the Participation of Social Organizations in the Prevention of COVlD-19
- Current Situation and Suggestions on the Development of Diagnosis Related Group (DRG) Policy in China
- A Systematic Review of Economic Evaluation of CDK4/6 Inhibitors in HR+/HER2-Advanced Breast Cancer
- Research on the Extraction Techniques of Ginseng Based on Patent Analysis
- A Case Analysis of the lnfluencing Factors of Job Satisfaction of Licensed Pharmacists in Retail Pharmacies Based on SEM-Taking R Retail Pharmacy for an Example