Quality of life, depression and anxiety in potential living liver donors for pediatric recipients: A retrospective single center experience
2022-11-29PaulaReineFlaviaFeierEduardoAntunesdaFonsecaRoselyHernandesJoaoSedaNeto
Paula K Reine, Flavia Feier,Eduardo Antunes da Fonseca,Rosely G Hernandes,Joao Seda-Neto
Abstract
BACKGROUND
Living donor liver transplantation is a safe alternative for patients on a liver transplant list. Donor evaluation goes beyond physical variables to include social, emotional, and ethical aspects. The role of pre-donation sociopsychological evaluation of the donor candidate is as important to the success of the procedure as is the medical assessment. Success implies recovery from the operation and pro-mpt engagement in pre-transplant professional and social activities, without leading to psychological or physical distress. Psychological profiling of potential living liver donors (PLLD) and evaluation of quality of life (QOL) can influence outcomes.
AIM
To evaluate the socio-demographics and psychological aspects (QOL, depression, and anxiety) of PLLD for pediatric liver transplantation in a cohort of 250 patients.
METHODS
This was a retrospective cohort study of 250 PLLD who underwent psychological pre-donation evaluation between 2015 and 2019. All the recipients were children. The Beck anxiety inventory, Beck depression inventory, and 36-item short-form health survey (SF-36) scores were used to evaluate anxiety (Beck anxiety inventory), depression (Beck depression inventory), and QOL, respectively.
RESULTS
A total of 250 PLLD were evaluated. Most of them were women (54.4%), and the mean age was 29.2 ± 7.2 years. A total of 120 (48.8%) PLLD were employed at the time of evaluation for donation; however, most had low income (57% earned < 2 times the minimum wage). A total of 110 patients (44%) did not finish the donation process, and 247 PLLD answered a questionnaire to evaluate depression, anxiety, and QOL (SF-36). Prevalence of depression was of 5.2% and anxiety 3.6%. Although most of the PLLD were optimistic regarding the donation process and never had doubts about becoming a donor, some traces of ambivalence were observed: 46% of the respondents said they would feel relieved if a deceased donor became available.
CONCLUSION
PLLD had a low prevalence of anxiety and depression. The foundation for effective and satisfactory results can be found in the pre-transplantation process, during which evaluations must follow rigorous criteria to mitigate potential harm in the future. Pre-donation psychological evaluation plays a predictive role in post-donation emotional responses and mental health issues. The impact of such findings on the donation process and outcomes needs to be further investigated.
Key Words: Liver transplantation; Children; Outcomes; Living donation
INTRODUCTION
The use of living donors has become standard practice in the field of pediatric liver transplantation. The extensive use of this technique has become possible owing to careful patient selection and the proven safety of the procedure. However, donor selection must be explored beyond physical, laboratory, and radiological evaluations. The role of a pre-donation sociopsychological evaluation of a donor candidate is as important to the success of the procedure as is the medical assessment. This implies recovery from the operation and prompt engagement in pre-transplant professional and social activities without leading to psychological or physical distress.
Donor candidates may experience anxiety and other psychological distress during the assessment period[1-3], such as depression, decision ambivalence (coexistence of inconsistent or opposing perceptions)[3], and fear. In a scenario that includes severe disease in a child and the risk of death while on the waiting list, part of the psychological evaluation is to rule out the possibility of coercion, even if the donor candidate is related to the recipient. Furthermore, knowledge of the patient’s social status and quality of life (QOL) is crucial for a thorough psychological assessment that will inform the decisionmaking process, such as acceptance of potential donors.
Little is known about the relationship between eligibility criteria and significant predictors of psychological strain in living donation candidates[4]. Moreover, the predictors of psychological strain may vary in different social scenarios, and may include income, education, and religious orientation.
This study aimed to evaluate the prevalence of depression, anxiety, and QOL in potential living liver donors (PLLD) for pediatric recipients. It also describes the socioeconomic profile of this population.
MATERIALS AND METHODS
A cohort of 250 consecutive PLLD aged > 18 years was selected for the pre-donation evaluation. All the recipients were children. The PLLD underwent psychological assessments during the evaluation process for living donations at Hospital Sírio Libanês, São Paulo, Brazil, between January 2015 and May 2019. This study was conducted in accordance with the principles of the Declaration of Helsinki. The Ethics Committee of Hospital Sírio-Libanês approved this study.
PLLD with a history of drug abuse, dependence, or previous diagnoses of psychiatric disorders were excluded from the analysis. Demographic data were collected through a medical chart review. The patients answered a questionnaire designed to evaluate their perception of the living donation process. QOL was assessed using the 36-item short-form health survey (SF-36) questionnaire[5].
To classify potential donors according to anxiety and depression levels, Beck anxiety inventory (BAI)[6] and Beck depression inventory (BDI)[7] scores were utilized.
The medical outcomes study SF-36 comprises 36 items divided into eight domains: Role-physical (RP), physical functioning (PF), general health (GH), vitality (VIT), social functioning (SF), roleemotional (RE), mental health (MH), and bodily pain (BP). Scaled scores for each domain were the weighted sums of the answers to the domain questions, with each score transformed into a 0-100 scale, with higher scores indicating better functionality or less pain[5].
Demographic variables were also evaluated: Gender, age, relationship to the recipient, education, employment status, religion, marital status, region of origin, and monthly family income.
Specific questions were posed to the PLLD regarding donation and decision-making processes (included as a supplementary material for consultation).
Statistical analysis
The values are expressed as mean ± SD or median, and 25 and 75 percentiles. Categorical data are presented as absolute values and percentages. All analyses were performed using the SPSS 21.0 statistical package (IBM, Inc., Chicago, IL, United States). The statistical review of the study was performed by our institution's biomedical statistics team.
RESULTS
A total of 250 PLLD met the inclusion criteria and underwent psychological evaluation before donation, between January 2015 and May 2019. Most of them were women (54.4%), and the mean age was 29.2 ± 7.2 years. PLLD self-declared as afro-descendent in 49.6% of the cases; 46.3% were married, 51.6% selfdeclared as Catholic, and 53.7% had a college degree or equivalent. A total of 120 (48.8%) PLLD were employed at the time of evaluation for donation; however, most had low income (57% earned < 2 times the minimum wage) (Tables 1). Most PLLD (51%) lived in the same region as the transplant center, and 214 (85.6%) were family members of the recipient (Table 2). A total of 110 patients (44%) did not finish the donation process. Reasons for not completing the donation processes are described in Table 3.
A total of 247 PLLD answered a questionnaire to evaluate depression (BDI), anxiety (BAI), and QOL (SF-36). Prevalence of depression was of 5.2%. The results of the BDI index were minimal in 237 (94.8%) patients, light in 11 (4.4%), moderate in 2 (0.8%), and severe in none. Prevalence of anxiety was of 3.6%. The results of the BAI index were minimal in 241 (96.4%), light in eight (3.2%), moderate in one (0.4%), and severe in none.
The results of the evaluation of QOL through SF-36 in each domain were: 96.2 ± 8.7 PF, 91.3 ± 22.6 RP, 89.3 ± 15.2 BP, 75.5 ± 10.9 GH, 82.6 ± 16.3 VIT, 90.8 ± 17.9 SF, 88.9 + 24.5 RE, and 86.1 + 13.8 MH.
Although most of the PLLD were optimistic regarding the donation process (motivations and ambivalence questionnaire, Table 4) and never had doubts about becoming a donor, some traces of ambivalence were observed: 46% of the respondents said they would feel relieved if a deceased donor became available.
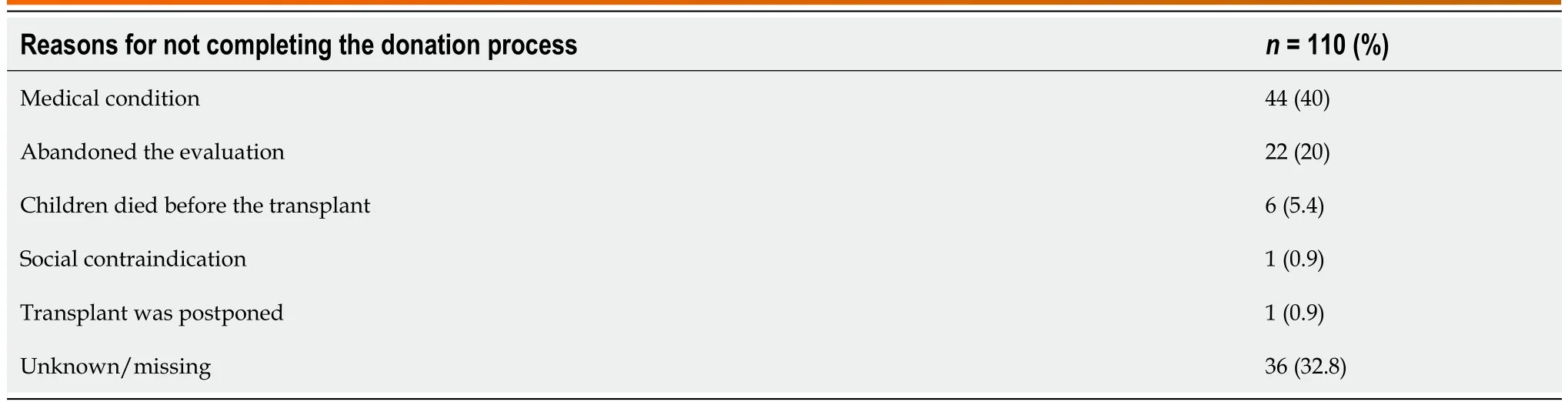
Table 3 Reasons for not completing the donation process
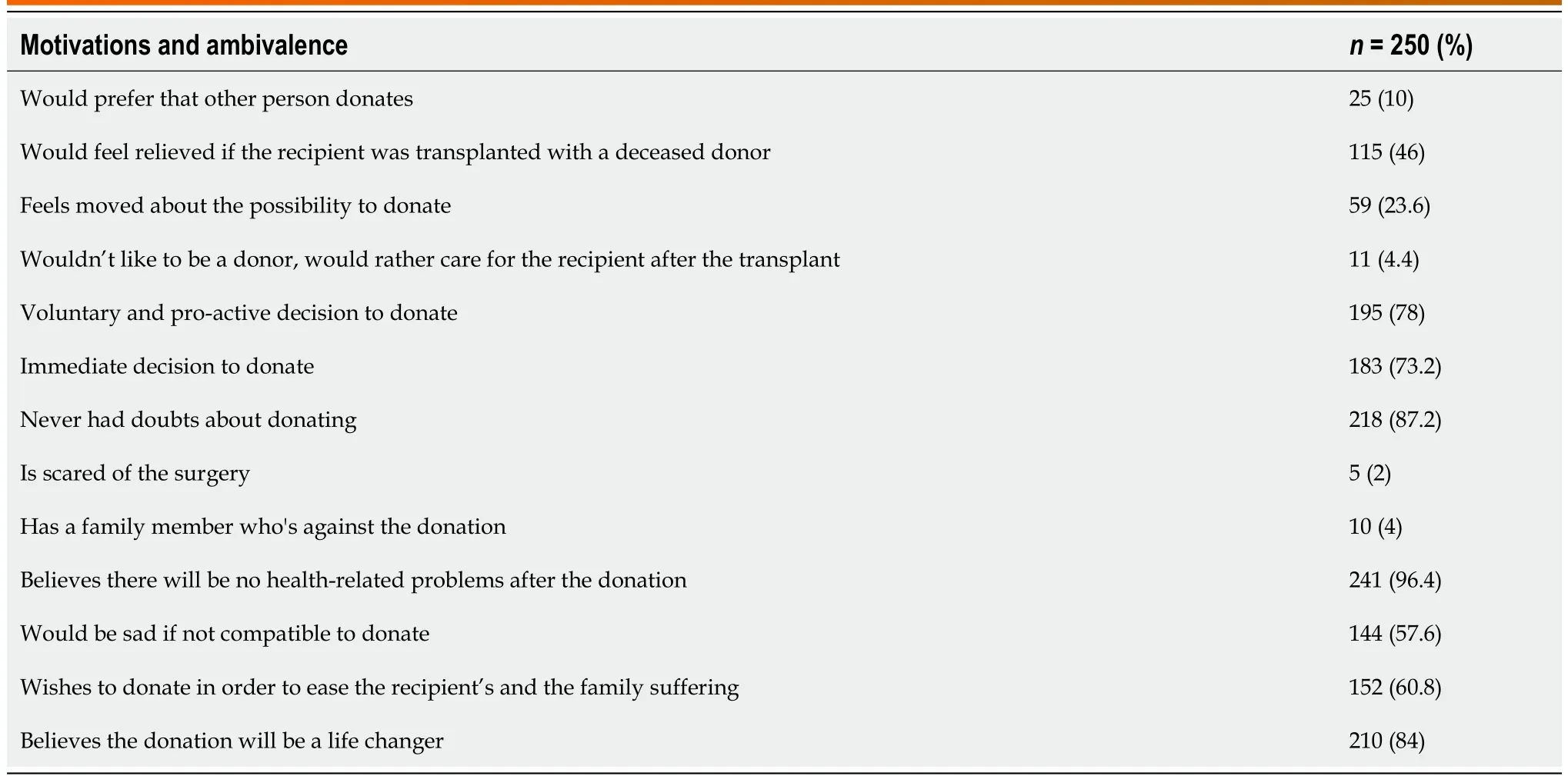
Table 4 Motivations and ambivalence in potential living liver donor
DISCUSSION
Socioeconomic characteristics have been shown to influence access to LDLT and promote health disparities in both adult and pediatric candidates[5-8]. PLLD profile may vary according to the region or country of origin, as well as the recipient’s age group (small children, adolescents, or adults). Most PLLD in this study were female, usually mothers, with a mean age of 29.2 years, and very low annual income. The national minimum wage in December 2021 in Brazil was $196 per month[9]; correspondingly, the annual income for 57% of the PLLD in this cohort was under $4704. This situation reflects the socioeconomic situation of our country, but the majority of liver transplantations were performed under Brazil's publicly-funded healthcare system (Sistema Único de Saúde), which covered all costs for donor and recipient care. A recent study performed in the United States on PLLD for children found a few different characteristics in these donors, especially a higher mean age (38), and a predominance of white individuals with college degrees[10]. One striking difference was the average age of the PLLD, which was nearly 10 years greater in the United States study than in the Brazilian study. It is conceivable that the PLLD in the present study, most of whom were mothers of the recipients, had children earlier, did not advance as far in their education, and had lower monthly incomes than potential donors in the United States. As for the remaining data in the comparison, although there are some common traits, we must point out that socio-demographic profiles are greatly influenced by cultural differences between countries and even by differences in the transplant centers assessing the patients. Despite the demographic differences encountered, the outcomes for donors and recipients reported by our group proved to be safe for donors[11] and with excellent short and long term results for the pediatric recipients[9,12].
Some studies have focused on donors' motivations, concerns, and feelings of ambivalence, as well as the influence that ties and relationships have on their decisions[13-15]. The present study evaluated the quality of the relationship between the potential donor and the recipient and/or the recipient's family, and found that this relationship is satisfactory for a significant part (98.4%) of the sample, regular for 1.2% of the sample, and nonexistent for 0.4%. Regular or nonexistent relationships probably involve PLLD who are not family members. The well-being and expectations of family members are taken into account and influence the decision to donate. In this regard, one study found that 94.1% of donors decide to donate to preserve the well-being of the whole family[15]. Another study[16] approaches the same family setting from a different perspective: family members who somehow show conflict towards the donation present high levels of anxiety, symptoms of depression, and low QOL. Ryu et al[15] have found differences in donor motivation levels linked to the donor-recipient relationship. According to the authors, parents donating to their children show higher motivation than children donating to their parents and present lower levels of anxiety and depression during the evaluation period prior to donation.
The World Health Organization (WHO)[17], in their report on prevalence estimates of mental disorders emphasizes some significant data that corroborate the results presented here. The proportion of depression in the world population in 2015 was estimated at 4.4% (vs 5.8% in the Brazilian population), being more prevalent among women (5.1%) than men (3.6%), with a total of 322 million people living with depression. There was an 18.4% increase in depression indices between 2005 and 2015, pointing to an increase in the disorder among the global population, including the higher-risk age group (55-74 years). Depression indices in the present study were 5.2% among potential donors. The potential donors are predominantly women, a risk factor for depression.
With regard to anxiety, the WHO[17], in their prevalence estimates of mental disorders, reported that the rate of anxiety disorders among the global population in 2015 was 3.6% (vs 9.3% in the Brazilian population) and was also more prevalent among women (4.6%) than men (2.6%), totaling 264 million people living with anxiety. Although the prevalence rates did not show significant differences among age groups, there was a slightly lower prevalence among the older age groups. The global anxiety indices grew by 14.9% between 2005 and 2015, suggesting an increase in disorders among the total population. Anxiety indices in the present study were 3.6% among potential donors. Similarly, the age group in our study presented a risk for anxiety, according to the WHO data. In regards to the SF-36 questionnaire, potential donors showed a lower impairment of QOL in GH, VIT and MH domains, and a greater impairment in the PF domain.
LDLT requires the donor to submit to surgery that has no medical benefit[15]. However, the process of preparing for the donation and the post-operative period may provide significant psychological benefits, such as finding new meaning in life and a feeling of plenitude for helping a loved one (in the case of a family member) or a person in need (in case of non-familial donors). This study evaluated the meaning that PLLD derived from the process and found the following benefits: improving the recipient's QOL (25.2%), saving a life (22.7%), a gesture of love (21.1%), a second chance for the recipient (14.9%), and doing good for someone else (13%). A separate question about their expectations regarding the donation obtained responses such as "a feeling of well-being with myself", "a new meaning for life through the donation", "better life conditions", and "family and social recognition" in 37.5% of cases. These data encourage important ethical questions, since a careful assessment of the donor, including a favorable physical and psychological evaluation, will minimize potential risks for the donor and are aligned with the bioethical principle of non-maleficence. Furthermore, the psychological benefits highlighted by this study and the spiritual benefits of a new meaning in life are in agreement with the bioethical principle of beneficence. Even though the reasons for not completing the donation process were not directly related to psychological aspects, it is difficult to know if in some instances it had a causative effect, such as in those who abandoned the evaluation during the donation process.
CONCLUSION
The scientific community places marked attention on the post-transplantation period, including the progress made by recipients and donors. However, the foundation for effective and satisfactory results can be found in the pre-transplantation process, during which evaluations must follow rigorous criteria to mitigate potential harm in the future. Pre-donation psychological evaluation is effective and plays a predictive role in post-donation emotional responses and mental health issues. Also, the sociodemographic findings of this particular population indicate the complexity of the donation process in a setting of low resources. The results of this study indicate the need for the transplantation community to take heed of the benefits of a thorough psychological evaluation of the potential donor, which will play a central role in predicting their emotional progress and the donation experience itself.
ARTICLE HIGHLIGHTS
Research results
A total of 250 PLLD were evaluated. Most of them were women (54.4%), and the mean age was 29.2 ± 7.2 years. A total of 120 (48.8%) PLLD were employed at the time of evaluation for donation; however, most had low income (57% earned < 2 times the minimum wage). Family members were the majority of the. A total of 110 patients (44%) did not finish the donation process. A total of 247 PLLD answered a questionnaire to evaluate depression (BDI), anxiety (BAI), and QOL (SF-36). Prevalence of depression was of 5.2% and anxiety 3.6%.
Research conclusions
The socio-demographic findings of this particular population indicated the complexity of the donation process in a setting of low resources. PLLD had a low prevalence of anxiety and depression. Predonation psychological evaluation plays a predictive role in post-donation emotional responses and mental health issues. The impact of such findings on the donation process and outcomes needs to be further investigated.
Research perspectives
Almost half of the evaluated potential donors did not complete the donation processes. Reasons for not completing the donation process should be further evaluated in other centers as well. To further study the impacts of donation among living liver donors, our group aims to evaluate the post-donation psychological outcome in these donors.
FOOTNOTES
Author contributions: Reine PK contributed to study design, data collection, manuscript writing; Feier F contributed to data analysis, manuscript writing; Hernandes RG contributed to data collection, manuscript final version critical analysis; da Fonseca EA contributed to manuscript writing, manuscript final version critical analysis; Seda-Neto J contributed to study design, manuscript writing, data analysis.
Institutional review board statement: The study was reviewed and approved for publication by our Institutional Reviewer.
Informed consent statement: It was exempted because of the retrospective nature of the study by the Hospital’s Ethics Committee.
Conflict-of-interest statement: None of the authors have any conflicts of interest related to the manuscript.
Data sharing statement: The original anonymous dataset is available upon request from the corresponding author at joaoseda@gmail.com.
STROBE statement: The authors have read the STROBE statement, and the manuscript was prepared and revised according to the STROBE statement.
Open-Access: This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin: Brazil
ORCID number: Paula K Reine 0000-0001-7087-0982; Flavia Feier 0000-0003-1339-2990; Eduardo Antunes da Fonseca 0000-0002-0853-2605; Joao Seda‐Neto 0000-0003-2267-5386.
S-Editor: Zhang H
L-Editor: A
P-Editor: Zhang H
杂志排行

World Journal of Hepatology的其它文章
- Natural history and management or liver aySuncuon ystorage disorders
- Immunotherapy for hepatocellular carcinoma: A promising therapeutic option for advanced disease
- Long-term and non-invasive in vivo tracking of DiD dye-labeled human hepatic progenitors in chronic liver disease models
- Hepatic involvement in children with acute bronchiolitis