Pancreatic transplant surgery and stem cell therapy:Finding the balance between therapeutic advances and ethical principles
2022-10-08MartinaPadovanoMatteoScopettiFedericoManettiDonatoMorenaDavideRadaelliStefanoErricoNicolaDiFazioPaolaFratiVittorioFineschi
Martina Padovano, Matteo Scopetti, Federico Manetti, Donato Morena, Davide Radaelli, Stefano D’Errico,Nicola Di Fazio, Paola Frati, Vittorio Fineschi
Martina Padovano, Federico Manetti, Donato Morena, Nicola Di Fazio, Paola Frati, Vittorio Fineschi, Department of Anatomical, Histological, Forensic and Orthopaedic Sciences,Sapienza University of Rome, Rome 00185, Italy
Matteo Scopetti, Department of Medical Surgical Sciences and Translational Medicine,Sapienza University of Rome, Rome 00189, Italy
Davide Radaelli, Stefano D’Errico, Department of Medicine, Surgery and Health, University of Trieste, Trieste 34149, Italy.
Abstract The latest achievements in the field of pancreas transplantation and stem cell therapy require an effort by the scientific community to clarify the ethical implications of pioneering treatments, often characterized by high complexity from a surgical point of view, due to transplantation of multiple organs at the same time or at different times, and from an immunological point of view for stem cell therapy. The fundamental value in the field of organ transplants is, of course, a solidarity principle, namely that of protecting the health and life of people for whom transplantation is a condition of functional recovery, or even of survival.The nature of this value is that of a concept to which the legal discipline of transplants entrusts its own ethical dignity and for which it has ensured a constitutional recognition in different systems. The general principle of respect for human life, both of the donor and of the recipient, evokes the need not to put oneself and one’s neighbor in dangerous conditions. The present ethical reflection aims to find a balance between the latest therapeutic advances and several concepts including the idea of the person, the respect due to the dead, the voluntary nature of the donation and the consent to the same, the gratuitousness of the donation, the scientific progress and the development of surgical techniques, and the policies of health promotion.
Key Words: Pancreas transplantation; Multi-organ transplants; Stem cell therapy; Ethical principles; Donor; Recipient
lNTRODUCTlON
Currently, the management of chronic diseases represents an issue of growing interest in relation to the incidence, the increase in life expectancy, and the loads deriving from prolonged care needs. An important problem related to chronic conditions is represented by the complications that inevitably and,sometimes even in the presence of adequate therapy, worsen the patient’s health. The complications of chronic diseases also affect health care by increasing the number of hospitalizations, the length of hospital stays, and health management costs. Therefore, the possibility of avoiding these implications constitutes a continuous challenge for healthcare professionals, spurring scientists to continuously identify new therapies aimed at overcoming the critical condition and consequent prevention of complications.
Chronic pancreatic diseases and specifically diabetes mellitus denote a burden for the health professions, as the worldwide incidence is continuously increasing; insulin therapy achieves good glycemic control but does not allow the restoration of damaged β-cells or prevent any complications related to glycemic changes. Over the years, countless approaches have been tried to definitively restore pancreatic function; first pancreas transplantation and later stem cell transplantation represent cuttingedge treatments and are the subject of great interest in this field of medicine.
Advances in pancreatic transplantology are currently at the center of heated debates in the medical,ethical, and legal fields. Therefore, similar treatments require an effort to clarify the ethical implications of pioneering procedures, often characterized by high complexity both from a surgical point of view,due to transplantation of multiple organs at the same time or at different times, and from an immunological point of view for stem cell therapy.
The present paper aims to outline an overview of the current perspectives of pancreatic replacement therapy with the aim of highlighting the ethical issues relating to the different procedures and providing useful information to professionals.
The formulation of the ethical considerations was based on a preliminary literature search on PubMed andReference Citation Analysis(https://www.referencecitationanalysis.com/) databases. Only contributions in English have been included; no time limits were applied. The review was conducted using MeSH terms, Boolean operators, and free text terms to broaden the search. The study design included case series, animal studies, retrospective and prospective studies, as well as reviews, clinical trials, and meta-analysis. No unpublished or gray literature was searched.
DlABETES MELLlTUS
Diabetes mellitus is an endemic pathology whose treatment poses several challenges to health professionals and determines a conspicuous healthcare expenditure globally. Worldwide, as documented by the International Diabetes Federation, the spreading of the disease is constantly increasing[1-3], with a prevalence for the years 2021 of about 537 million people. Type 1 diabetes mellitus (T1DM) affects about 10% of the general population, with greater prevalence among children and young adults; even in this age range, the incidence is continuously growing[4], with an overall annual increase of approximately 3%. In 2021, it was found that more than 3 out of 4 adults with diabetes live in low- and middle-income countries and that around 240 million adults have affected undiagnosed diabetes; concerning mortality data, it appears that in 2021 deaths related to diabetes and its complications were 6.7 million (1 every 5 s)[5].
T1DM is among the most common autoimmune disorders and is characterized by multifactoriality,with imposing importance of genetic predisposition; in detail, particular human leukocyte antigen polymorphisms are frequently predisposed[6]. From a pathophysiological point of view, the etiology must be related to the specific immune-based destruction of insulin-producing β-cells, sparing glucagon-producing α-cells, and somatostatin-producing δ-cells[7]. Specifically, this destruction is caused by an incorrect recognition as autoantigens of some cellular components (i.e.insulin, islet antigen 2, zinc transporter 8, and glutamic acid decarboxylase 65[8,9]). According to some authors, recognition as “foreign” proteins can occur because of posttranslational modifications, represented for example by citrullination, deamination, and disulfide bridge formation[10].
The peculiar clinical heterogeneity makes diagnosis difficult and often delayed, being frequently placed at the onset of symptoms[11]. Given the diagnostic delay and systemic involvement, subjects with T1DM have a tripled rate of hospitalization in relation to long-term complications[12], a deterioration in the quality of life, as well as a decrease in life span from 1 year to 13 years.
Although it is not a curative treatment, not regenerating the islets of Langerhans, the administration of exogenous insulin through daily injections or computerized pumps, represents the most common treatment for obtaining a condition of euglycemia. Actually, the administration of exogenous insulin and a healthy lifestyle reduce blood glucose, but despite this, vascular complications resulting in irreversible organic damage are inevitable in most patients[13,14]. Sometimes, even in the case of correct administration, episodes of hyperglycemia can occur and if persistent can lead to irreversible complications systemically. Occasionally, even in patients with good glycemic control, injections carried out repeatedly and erroneously in the same site can determine a lipodystrophic condition, at the basis of an abnormal release of the inoculated insulin with consequent episodes of hypoglycemia. The latter complication is life-threatening and is associated with a mortality rate of 3%-6%[15].
Therefore, the development of innovative treatments is not only a research challenge but a necessity for the entire population[16-18]. This indispensability also derives from the widespread involvement of young patients who in the absence of a curative therapeutic strategy must face T1DM and all the associated complications throughout life.
Whole pancreas and islet allotransplantation as well as stem cell therapy are currently the only treatments for T1DM capable of re-establishing a normoglycemic state without an exogenous insulin supply. At the same time, these treatments are effective in reducing or eliminating dietary restrictions and hyperglycemia-related organ damage.
PANCREAS REPLACEMENT THERAPY
Transplant surgery
Whole pancreas and islet allotransplantation have undergone in recent years a remarkable development related to the refinement of the selection criteria of the donor and the recipient, to the evolution of surgical techniques, and to the use of new immunosuppressive drugs that have led to a remarkable improvement of the organ and patient survival[19,20].
Synthetically, these treatments can be performed in patients with T1DM with good renal function,chronic kidney disease, and previous kidney transplant. As concern of the different therapeutic possibilities available, the choice of the ideal treatment must be weighted according to the state of the underlying diabetic disease, the presence of diabetes complications, age, general conditions, and surgical risk[21,22].
The most relevant clinical element to indicate pancreatic transplant alone is the presence of unstable diabetes (with frequent hyperglycemia, recurrent and unpredictable episodes of ketoacidosis,asymptomatic hypoglycemia with life-threatening despite correct insulin therapy) that is associated with at least two rapidly progressing complications (proliferative retinopathy, peripheral and/or autonomic neuropathy, and vasculopathy)[23]. The presence of adequate renal function must be ascertained in pancreatic transplant alone candidate patients since the subsequent immunosuppressive therapy, including potentially nephrotoxic drugs, may lead to a reduction in the functional reserve.
Simultaneous pancreas and kidney transplantation is indicated in patients with T1DM on dialysis or pre-dialysis[24]. An increasing number of scientific evidence reveal substantial advantages in the execution of the transplant before the start of dialysis. In fact, such a choice avoids complications related to uremia, reduces the costs of dialysis, and intervenes earlier on other chronic complications of diabetes[25,26]. Surgery is also affected by lower postoperative morbidity and mortality.
Furthermore, pancreas after kidney transplantation is proposed to patients with T1DM who have previously been transplanted only with kidney from cadaver or living donor, especially if a difficult metabolic control and rapid evolution of the degenerative complications of diabetes coexist. Among the main advantages, since an immunosuppressive therapeutic regimen is already in place, there is a reduction of risks with the persistence of the operative risk only[27]. Moreover, the latter is significantly lower than the risks related to the further development of secondary complications of diabetes,including the recurrence of diabetic nephropathy in the transplanted kidney[28].
Finally, allogenic pancreatic islet transplantation has the same indications as whole pancreas transplantation (sometimes associated with renal transplant) but is performed through infusion into the portal vein[29,30].
Currently, whole pancreas and islet allotransplantations still have important limitations related to donor scarcity, post-transplant graft loss, and immunosuppressive therapy[31,32]. For similar reasons,further research is underway to expand accessibility to pancreatic replacement therapy.
Stem cell therapy
Stem cell transplantation represents a cutting-edge treatment and falls within the broad context of regenerative medicine that allowing for the definitive recovery of damaged organs and tissues is experiencing a period of maximum expansion; this branch is involved in many areas of medicine finding application also in pancreatic diseases. As previously stated, regenerative medicine is heavily investigated in the treatment of T1DM, but some studies highlight its applicability also in type 2 diabetes mellitus[33]. To date, two main approaches have been tested to ensure the restoration of insulinproducing β-cells. The most common approach consists in the implantation in the recipient of pancreatic progenitor cells, whichin vivodifferentiate into β-cells and over months reach a functional mass composed of progenitor and other pancreatic cells[34]. The other approach involves thein vitrogeneration of β-cells and their subsequent implantation to reduce the volume of the transplant and restore pancreatic function in a short time[35-37].
The selection of the cell type for the implementation of the protocols provides for different possibilities. The stem cells can be classified in embryonic and non-embryonic “somatic” stem cells. Both groups share peculiar properties as the ability for unlimited or prolonged self-renewal and the capacity to differentiate into more specialized cell types[38,39].
The embryonic stem cells, obtained from the internal cell mass of the blastocyst[40,41], represent the gold standard concerning pluripotency; in fact, through different procedures, these cells can self-renew or differentiate into multiple cell lines, such as hematopoietic progenitors and endothelial cells, as well as cardiac, neuronal, and pancreatic tissues[42-46].
Non-embryonic stem cells include mesenchymal stem cells (MSCs), which are endowed with multipotency, and are therefore able to self-renew and differentiate into different cell lines[47]. The sources from which MSCs are obtained are represented by the bone marrow and adipose tissue[48].Such cells find wide application in the therapy of many degenerative and auto-immune diseases[49,50].Therefore, although the exact mechanism is currently not delineated, MSCs are used in the treatment of T1DM due to an immunomodulatory and reparative action on damaged tissues[51]; in detail, MSCs allow euglycemia to be reached restoring the β-cells and reducing the autoimmune response through an immunomodulatory function[52-54]. Specifically, the ability to regulate the immune response constitutes the main mechanism with an antidiabetic effect since, by ensuring the survival of the β-cells,it contributes to the achievement of euglycemia.
From a molecular point of view, they carry out an inhibitory action against T, B, and natural killer cells, while they perform an activating action against regulatory T cells and modulate the function of dendritic cells[55,56]; furthermore, these cells create a local immunosuppressive environment. In addition to the above property, MSCs can differentiate into lineage-specific progeny; anin vitrostudy has demonstrated the greater ability of adipose-derived MSCs to differentiate into β-cells[57]. As part of this regenerative capacity, some authors have described the secretion of cytokines and growth factors capable of stimulating β-cells[58]. MSCs exhibit low immunogenicity as they do not express costimulating molecules such as human leukocyte antigen-DR as well as CD80, CD86, CD40, and CD40L[59-62]. Therefore, in consideration of the immunomodulatory capacities, MSCs avoids allogenic rejection in humans and animal models[63], and they can be transplanted without the need for the recipient to take immunosuppressive therapy[64].
To re-establish pluripotency in mature stromal cells, some scientists developed cutting-edge protocols that resulted in the spread of inducible pluripotential stem cells[65,66]. Such a method introduces a new treatment for T1DM to carry out the autologous transplant[67-69].
ETHlCAL lSSUES
Transplant surgery
The ethics of transplant surgery is at the center of a bundle of anthropological, ethical, juridical, medical,and political questions. The application of transplant surgery requires reflections on the lawfulness and on the limits to the practice even more so in complex transplants such as the pancreatic one. For these reasons, the ethical assessment of pancreatic transplantation cannot disregard the evaluation of the general principles underlying the organ replacement therapy.
The fundamental value in the field of organ transplants is, of course, a solidarity principle, namely that of protecting the health and life of people for whom transplantation is a condition of functional recovery or even of survival[70]. The nature of this value is that of a concept to which the legal discipline of transplants entrusts its own ethical dignity and for which it has ensured a constitutional recognition in different systems. The general principle of respect for human life, both the donor and the recipient, evokes the need not to put oneself and one’s neighbor in dangerous conditions. In particular,if the transplant from a living donor involves problems of incompatibility in the recipient or a high risk for the life of the donor, the availability of one’s body for the good of another must be subordinated to the preservation of the integrity of the person involved. Nevertheless, the pursuit of the solidarity purpose requires, in addition to the attention for the implications concerning the living donor, the acceptance of some basic principles related to the corpse donation such as respect for the will manifested before death, the dignity of the person, and the values of relatives of the deceased.
The affirmation of the principle of solidarity and the positive overcoming of the principles of protection of life and integrity of the body also implies the gratuitousness of donation. In fact, especially in the case of the living donor, organ donation should be inspired by the firm will to save a life and not by the mere possibility of receiving a reward. With regard to the donation from corpses, gratuitousness is instead guaranteed, in addition to the principle of charity, by the concept of respect for the deceased person. The gratuity is not resolved in the pure and simple lack or renunciation of a pecuniary compensation, but it is characterized by the intent of solidarity and the achievement of a predetermined result not left to the free determination of the donor. Moreover, gratuitousness constitutes a guarantee of the freedom of consent, removed from the constraints of economic necessity[71].
Finally, the principle of justice constitutes an important ethical assumption in relation to the context of deficiency in which transplant surgery is expressed. Given that the supply of organs is inferior to the demand, it is crucial that the identification of the recipients is based, in addition to the medical considerations, on strict criteria that prevent the greater economic capacity from becoming the most important, if not the unique, condition of accessibility to the organs available[72]. In the allocation of organs,impartiality cannot be absolute since each choice is based on values and is therefore subject to reference criteria. Any decision on the matter involves the “cutting” of something and the “waste” of something else, precisely because each allocative choice is based on the preference of one solution over another.However, the inevitable partiality must not result in preconceived discrimination and the selection criteria must be conceived considering the analysis of the situations, the possibilities of realization, and the management complexity[73].
Stem cell therapy
The development of stem cell therapies requires continuous discussions and reflections in the medical,bioethical, religious, and judicial fields. Precisely, a broad debate that includes all aspects of the new therapeutic frontier from bench to bedside is needed.
As far as the experimental aspect is concerned, the possible use of stem cells in the treatment of T1DM is investigated in about 70 studies (www.clinicaltrials.gov); of these, 54 are in phases I and II of experimentation. In consideration of the pioneering nature of the research, the pursuit of methodological rigor aimed at obtaining reliable and reproducible results is fundamental[74]. Nonetheless, transparency in the sharing of results is desirable on the part of researchers[75]. In fact, scientific disclosure in such sensitive areas for health and public opinion must presuppose a clear discussion of the results, not generating false expectations and detailed in the aspects relating to the complications of the treatment.With reference to the last aspect, scientific and commercial competition can generate pressure regarding the declaration of results concerning problems such as tumorigenicity, neoangiogenic potential, and unwanted differentiation of stem cells[76].
The validation of stem cell-based therapies in the treatment of T1DM undoubtedly limits the problem of donor scarcity without eliminating the issues on access to care. In fact, the limited availability of this therapeutic possibility and the high costs currently pose serious sustainability problems. The problem is strongly accentuated by the epidemiological peculiarities of diabetes mellitus that presents a greater diffusion of decompensated and refractory to therapy forms among the socioeconomically disadvantaged groups of the population. Therefore, both in experimental and clinical practice, the inspiration to the principles of equity and justice is of great importance to guarantee equal therapeutic possibilities to all patients. Despite some still undefined regulatory and technological aspects, a prospect of certain usefulness in terms of improving access to care is represented by biobanking; the development of banks with large-scale storage represents a means to obtain the amplification of cellular reserves, the reduction of treatment costs, and ultimately the therapeutic possibilities for patients[77-79]. In parallel to what has been stated so far, the use of stem cells for the creation of experimental models of T1DM can certainly guarantee the personalization and accessibility to pharmacological treatments of higher quality and safety in the phase before replacement therapy[80].
Given the greater incidence of T1DM in pediatric and juvenile age, the prognostic aspects of the disease as well as the complexity of the therapies, further ethical aspects worthy of further study concern self-determination, information, and shared planning of care pathways. To jointly pursue the lengthening of life expectancy and the improvement of the quality of the same, it is of fundamental importance in such patients to carry out a global assessment of frailty, foreseeable risks, expected benefits, and life prospects[81]. In the context of stem cell-based therapies, it is all the more important to provide adequate responses to the patient’s requests since the quality of care necessarily depends on the conscious choice of a treatment capable of improving life and recovery expectancies[82,83]. Then, in a specialized therapeutic field such as regenerative therapy, it is possible to respect the principles of selfdetermination, dignity, and identity of the patient by promoting the global acceptance of the disease,clearly stating the therapeutic objectives, and sharing the concept of proportionality of the treatments.
POSlTlON STATEMENT
Pancreatic replacement therapy requires a significant scientific, regulatory, and ethical commitment. The enhancement of the efforts implemented by the different stakeholders presupposes an attitude aimed in general at avoiding injury to the person and at providing support to the rapid evolution of knowledge.
In a nutshell, having to express a position that can be useful to those involved in the experimentation and clinical use of pancreatic replacement therapies, a good practice should presuppose (Figure 1): (1)Adoption of a rigorous experimental method aimed at transparency to clearly state results and avoid the onset of false expectations; (2) Objective sharing of results with avoidance of pressures deriving from scientific and instrumental competition; (3) Comprehensive assessment including quality of life before treatment as well as prognostic aspects in terms of post-treatment morbidity and mortality; (4)Calibration of the therapeutic choice based on the availability of donors, the possibility of posttransplant graft loss, and the feasibility of immunosuppressive therapy; (5) Foundation of therapeutic choices on the protection of health and life, both of the donor and the recipient, in compliance with the principles of solidarity as well as respect for the dignity and integrity of the person; (6) Guarantee of gratuity to avoid donations for profit and ensure the freedom of donation; (7) Codification of strict criteria for inclusion in pancreatic replacement therapy paths through the evaluation of concrete cases,feasibility, and management complexity; (8) Avoidance of socioeconomic discrimination in the evaluation of therapeutic choices; (9) Guarantee of equal therapeutic possibilities to all patients inspiring experimental and clinical practice on the principles of equity and justice as well as having regard for the disadvantaged groups of the population; (10) Implementation of technologies for the spreading of innovative therapies and the expansion of access to care (e.g., biobanking); (11) Attention to aspects related to fragility, self-determination, information, and shared planning of care pathways, especially in the pediatric field; and (12) Promotion of the global acceptance of the disease through a clear sharing of therapeutic objectives, foreseeable risks, expected benefits, life prospects, and proportionality of the treatments.
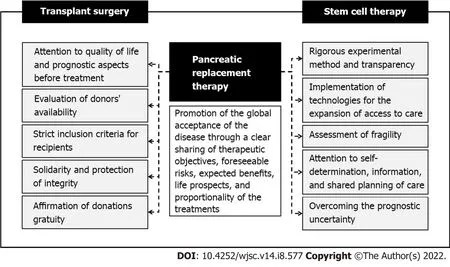
Figure 1 Fundamental principles leading experimental and clinical practice in pancreatic replacement therapy.
CONCLUSlON
The rapid advancement of knowledge and the implementation of therapeutic possibilities in the field of pancreatic replacement therapy imply different concerns relating to experimental and clinical practice.The heterogeneity of therapeutic strategies determines a wide range of ethical aspects differently inherent to transplant surgery and stem cell-based therapies. At present, it is essential to proceed with rigor to support the encouraging results obtained from scientific research from an ethical and legislative point of view. Therefore, a joint commitment of the different stakeholders is desirable so that in the near future it will be possible to proceed on a large scale to a definitive treatment against an extremely insidious disease, such as diabetes, in terms of prevalence and prognosis.
FOOTNOTES
Author contributions:All authors equally contributed to this paper with conception and design of the study,literature review and analysis, drafting, critical revision, and approval of the final version.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Italy
ORClD number:Martina Padovano 0000-0003-2452-7926; Matteo Scopetti 0000-0002-7259-3090; Federico Manetti 0000-0002-8047-6193; Donato Morena 0000-0001-6473-7632; Davide Radaelli 0000-0002-7053-6463; Stefano D'Errico 0000-0002-5064-6614; Nicola Di Fazio 0000-0003-4436-0203; Paola Frati 0000-0002-0358-7965; Vittorio Fineschi 0000-0002-1686-3236.
S-Editor:Fan JR
L-Editor:Filipodia
P-Editor:Fan JR
杂志排行

World Journal of Stem Cells的其它文章
- Metabolic determinants of stemness in medulloblastoma
- Sinomenine promotes differentiation of induced pluripotent stem cells into immature dendritic cells with high induction of immune tolerance
- Combination of mesenchymal stem cells and three-dimensional collagen scaffold preserves ventricular remodeling in rat myocardial infarction model
- How mesenchymal stem cell cotransplantation with hematopoietic stem cells can improve engraftment in animal models