Endoscopic therapy using a self-expandable metallic stent with an anti-migration system for postorthotopic liver transplantation anastomotic biliary stricture
2022-09-22LarissaWermelingerPinheiroFernandaPrataMartinsGustavoAndradeDePaulonicaciaCamposContiniAngeloPauloFerrariErmelindoDellaLibera
INTRODUCTION
Biliary tract lesions are common postoperative adverse events (AEs) after orthotopic liver transplantation (OLT).Anastomotic biliary strictures (ABSs) occur most frequently and are responsible for approximately 40% of all complications after OLT[1-4].
Endoscopic balloon dilation followed by placement of side-by-side multiple plastic stents (MPSs) in repeated procedures every 3-4 mo,up to 12 mo,is the standard treatment for ABS.This treatment strategy has a high success rate,ranging from 70% to 100%[1,5].
Despite such a high success rate,this strategy demands repeated procedures[1,6-9].Recent studies using fully covered self-expandable metallic stents (FCSEMS) have shown encouraging results,with resolution rates similar to those observed with the MPS strategy[5,7,10].However,a high FCSEMS migration rate of between 10% and 40% has been reported,which is a possible limitation for its use[5-7,10].
In a narrow creek28 she found a whole troop of little human children, quite naked, and sporting about in the water; she wanted to play with them, but they fled in a great fright; and then a little black animal came to the water; it was a dog, but she did not know that, for she had never before seen one
We hypothesized that a FCSEMS with an anti-migration system (Am-FCSEMS) could be an alternative for postorthotopic-OLT (p-OLT) ABS treatment.Recently,a study with promising results compared the use of an Am-FCSEMS with other types of conventional metallic stents in regards to the p-OLT ABS resolution rate and their respective migration rates[11].
This study was conducted at Hospital Israelita Albert Einstein (HIAE),São Paulo,Brazil.HIAE is a private tertiary care referral centre where approximately 150 OLTs are performed yearly.
MATERIALS AND METHODS
The objective of this study was to evaluate the efficacy of endoscopic treatment using an Am-FCSEMS in patients with p-OLT ABS.
Patients
In conclusion,in this retrospective study,endoscopy therapy using an Am-FCSEMS or flaps for p-OLT ABS is safe and effective,with the stricture´s high-resolution rate probably being due to the absence of stent migration.
The male eagle seized the rabbbit with sharp craws and killed it. When getting ready to fly away, the scene before his eyes made him startled. Just now under the body of the old gray rabbit lay four stiff baby rabbits. Love is broad and profoud, yet also cruel.
37. Ancient dame leaning on a staff: The woman has the appearance of a venerable grandmother or village wise woman. The children are placated102 by her harmless appearance.Return to place in story.
This study was conducted in accordance with the World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects and was approved by our institution's Human Research Committee.The patients provided written informed consent prior to inclusion in the study.
Procedures
Endoscopic retrograde cholangiopancreatography (ERCP) was performed using a therapeutic video duodenoscope (TJF-180 Olympus Optical Co.,Ltd.,Tokyo,Japan) with patients under monitored anaesthesia.After selective biliary cannulation,cholangiography was performed for the evaluation and characterization of biliary stricture,followed by the passage of a guidewire.After positioning the guidewire,biliary sphincterotomy was performed in patients with native papilla,and an Am-FCSEMS (10 mm in final diameter and 60 or 80 mm in length,BCT Hanarostent
M.I.Tech,Co.) was placed (Figure 1A and B).Balloon dilation of the stricture was performed only if necessary to introduce the stent.According to the physician’s choice,the length of the stent was determined during cholangiography to place the proximal end between the stricture and the hepatic hilum and the distal end in the duodenum.Patients were followed up for clinical signs of biliary obstruction and scheduled to have the stent removed after 12 mo if no complications occurred.
Endpoints
The primary study endpoint was the efficacy of the endoscopic treatment of p-OLT ABS using an Am-FCSEMS for a 12-mo period.Efficacy was evaluated based on ABS resolution.After stent removal,the biliary stricture was considered resolved if there was no stricture observed on cholangiography or a minimum stricture that allowed the passage of a 12-mm inflated extractor balloon without difficulty.Secondary endpoints were technical success (defined as stent placement),adverse effects related to ERCP (bleeding or pancreatitis),and stent dysfunction (migration or obstruction).
RESULTS
62.Flew into such a rage that she burst: Trolls are supposed to burst when exposed to sunlight. See more about trolls in the note above. The troll s self-destruction is reminiscent of Rumpelstiltskin s self-destructive rage.Return to place in story.

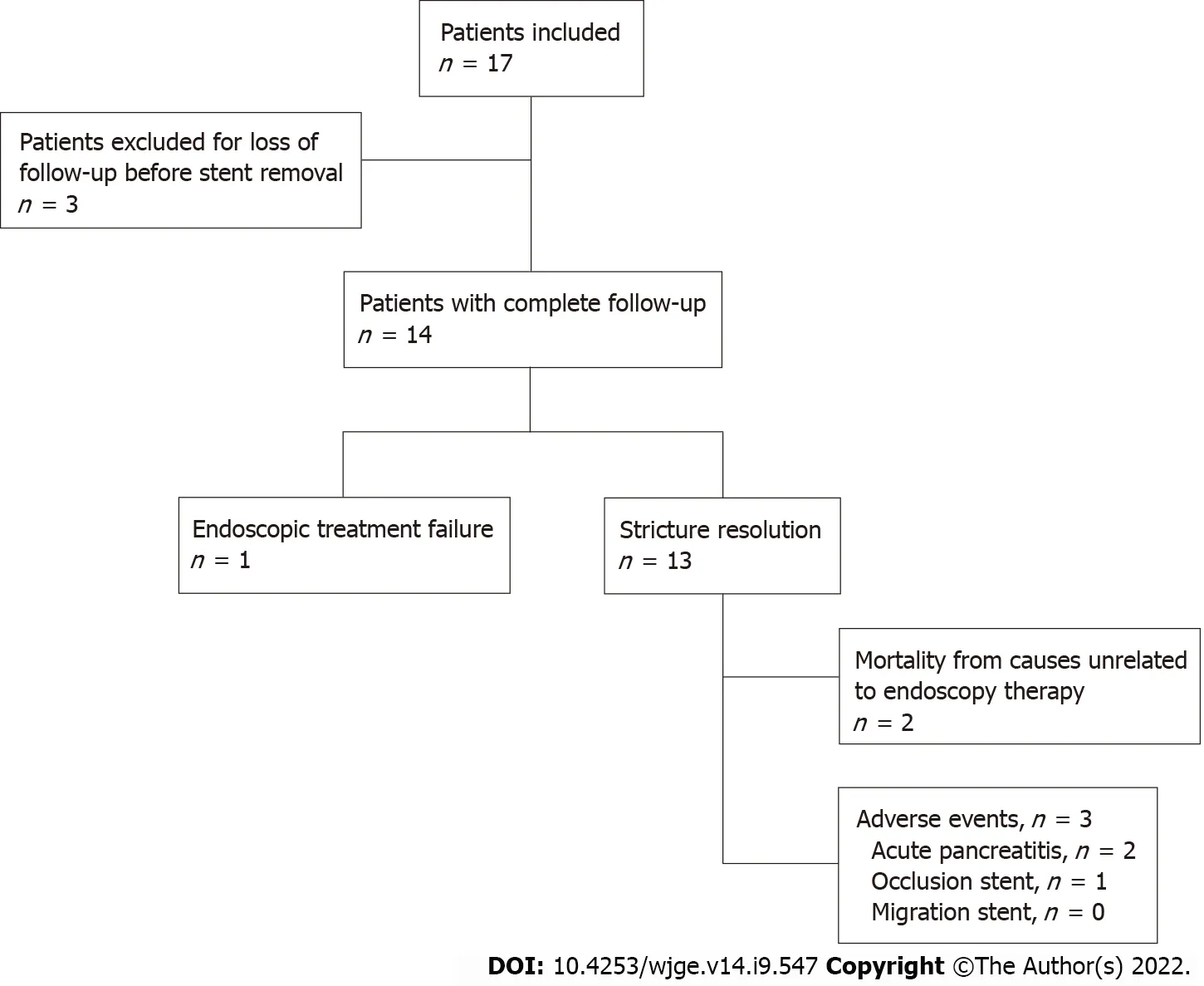
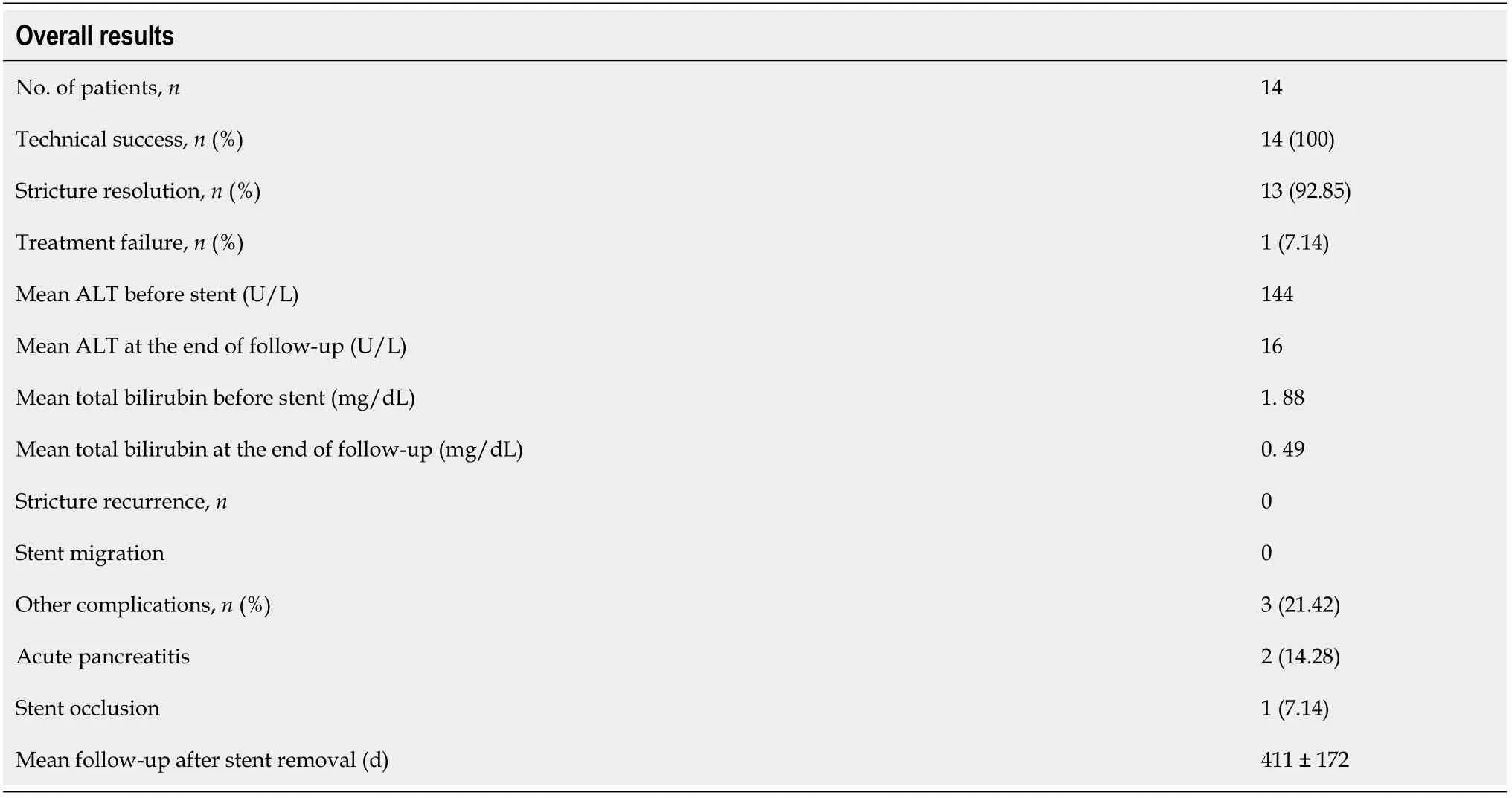
Complete resolution of the stricture occurred in 13/14 patients (92.85%).Only 1 patient (7.14%) experienced endoscopic treatment failure after 338 d with the stent in place,which was determined by cholangiography as persistence of stricture.This patient was referred for endoscopic treatment using MPSs for a longer period.AEs occurred in 3 out of 14 patients (21.42%).There were 2 patients (14.28%) with mild acute pancreatitis and 1 patient (7.14%) with stent dysfunction (occlusion by biliary sludge and stones with cholangitis),which was treated endoscopically without the need for stent removal.There was no distal migration of the stent in any patient (Table 2).There was no mortality related to ERCP and/or endoscopic therapy with the stent.After removal of the Am-FCSEMS,all 13 patients who had ABS resolution were followed-up (411 ± 172 d),and there was no need for further endoscopic therapy or stricture recurrence.Two patients died from causes unrelated to endoscopy therapy.
DISCUSSION
The longer stent maintenance period (12 mo) in our study in relation to other studies with metallic stents[2,7] and the absence of migration possibly related to the antimigration mechanism may have contributed to the favourable result observed in our patients.
Our present study shows that p-OLT ABS treatment with an Am-FCSEMS is effective and safe,with a stricture resolution rate of 92.85%,which is comparable to the results of other studies involving MPSs[5,9,12] and FCSEMSs[5,7,13].In our study,the average time between liver transplantation and endoscopy therapy for ABS was lengthy (116 wk),which may have impacted the results and thus,is a possible limitation of this study[3,6,8].Nevertheless,our results were comparable with those of other studies that used this anti-migration stent model[11].
The technical success rate of 100% in this series,which is comparable to that in other studies[6,12,14],demonstrates the applicability of this technique.No patients experienced distal migration of the stent.As described in previous studies,the main disadvantage of using FCSEMS is the high migration rate of up to 37.5%[10,12,14,15].It is possible that treatment with an Am-FCSEMS may present better results due to the lower risk of migration and longer stent patency.Although in our study assessment of costs was not an included objective,it is possible that since this stent has a lower migration rate its use could result in a lower number of procedures and thus lower costs,but this hypothesis should be verified in future controlled studies.
The AEs observed with ERCP-related therapy and/or stenting were mild pancreatitis and delayed stent obstruction.All patients in whom the stent was placed underwent biliary sphincterotomy,and mild acute pancreatitis was related to the ERCP procedure in 2 out of the 14 patients (14.2%).Despite this higher rate of complications compared to that in the literature[5-7,13],these patients underwent successful clinical treatment.Stent dysfunction (obstruction) occurred late and was caused by biliary sludge or stones,with jaundice and cholangitis occurring in only one patient (7.1%).This complication and its endoscopic treatment with or without stent replacement is described in the literature[5,6].This patient was treated with antibiotics and endoscopy without the need for stent replacement.
This study shows that treatment using Am-FCSEMS has a high rate of stenosis resolution,probably due to the absence of stent migration,and may result in a lower number of procedures.
My husband and I had been together for six years, and with him I had watched as his young children became young teenagers. Although they lived primarily with their mother, they spent a lot of time with us as well. Over the years, we all learned to adjust, to become more comfortable with each other, and to adapt to our new family arrangement. We enjoyed vacations together, ate family meals, worked on homework, played baseball, rented videos. However, I continued to feel somewhat like an outsider, infringing1 upon foreign territory. There was a definite boundary line that could not be crossed, an inner family circle which excluded me. Since I had no children of my own, my experience of parenting was limited to my husband s four, and often I lamented2 that I would never know the special bond that exists between a parent and a child.
Considering the treatment of patients with p-OLT ABS,the use of FCSEMSs may be an interesting alternative in relation to MPS therapy,considering FCSEMS placement presents comparable results with fewer ERCP procedures[4,5,7,10].However,spontaneous stent migration may be a limitation of FCSEMS placement[10,12,14].
This retrospective study has some limitations,such as a small sample size from a single centre.Another limiting point for this study is the lack of a control group.However,our results showed that treatment with Am-FCSEMS can be an alternative for patients with p-OLT ABS.Therefore,prospective and comparative studies should be encouraged to evaluate the efficacy of endoscopic treatment using Am-FCSEMS versus MPSs.Nevertheless,we present similar results for the resolution of ABS compared to those in other studies using MPSs and FCSEMSs as well as a recent study using an Am-FCSEMS.In this series,the advantage of treatment using an Am-FCSEMS in relation to treatment with MPSs was the need for only two ERCP procedures over 12 mo,while the advantage in relation to FCSEMS therapy was the absence of migration.
CONCLUSION
From April 2018 to October 2020,17 patients between 18 and 76 years of age diagnosed with p-OLT ABS who were referred to the endoscopy unit were considered for inclusion in this retrospective study,regardless of previous endoscopic treatment (MPS or FCSEMS).The exclusion criteria were pregnancy,nonanastomotic biliary or hilar stricture,hepatic artery stenosis/thrombosis,isolated biliary fistulae,and patient refusal.To avoid the risk of biliary intrahepatic duct occlusion secondary to stent placement,a distance shorter than 2 cm from the stricture to the hepatic hilum was also considered an exclusion criterion.
ARTICLE HIGHLIGHTS
Research background
Endoscopic therapy using multiple plastic stents is the standard therapy for postorthotopic liver transplantation (p-OLT) anastomotic biliary stricture (ABS).However,this approach demands repeated procedures.Recent studies using fully covered self-expandable metallic stents (FCSEMS) have shown encouraging results,but migration occurs in 10% to 40% of cases.We hypothesized that a FCSEMS with an anti-migration system (Am-FCSEMS) could be an alternative for treatment in patients with p-OLT ABS.
Some people would call it an extremely lucky chance happening, the result of a hole in the church wall, an old tablecloth, a pastor’s ingenuity19 in solving a problem and so on. But the combination of events was far too complex for it to have been merely “coincidence.”
Research motivation
The efficacy of treatment using an Am-FCSEMS for p-OLT ABS is not yet well established.The outcomes of endoscopic treatment using this type of stent have become clinically relevant.
Research objectives
This study aimed to evaluate the efficacy of endoscopic treatment using an Am-FCSEMS in patients with p-OLT ABS.
You have to laugh and find humor every day. You ve got to have a dream. When you lose your dreams, you die. We have so many people walking around who are dead and don t even know it! There is a huge difference between growing older and growing up.
40.I swore not to by heaven: Despite great hardship, the princess keeps her promise not to reveal to any human being what has happened to her; thus she proves her moral virtue, which finally brings about retribution and a happy ending. Here the dangers which the heroine must master are inner ones: not to give in to the temptation to reveal the secret (Bettelheim 1975, 137).
Research methods
This study was conducted in a private tertiary care centre in São Paulo,Brazil.From April 2018 to October 2020,patients with p-OLT ABS and indications for endoscopic therapy were included in this study,and an Am-FCSEMS (10 mm in final diameter and 60 or 80 mm in length) was placed (Hanarostent MI Tech,Co).
Research results
Technical success occurred in all 14 patients (100%).There were no cases of distal stent migration.Complete resolution of the stricture occurred in 13/14 patients (92.85%).Adverse events occurred in 3/14 patients (21.42%): 2 patients with mild acute pancreatitis and 1 patient with stent dysfunction (occlusion).No deaths occurred related to therapy.After Am-FCSEMS removal,all 13 patients who had ABS resolution were followed-up for an average of 411 ± 172 d,and there was no stricture recurrence or need for further endoscopic therapy.
As they only had food for a short time longer, and saw a miserable6 death awaiting them, Maid Maleen said, We must try our last chance, and see if we can break through the wall
Research conclusions
Endoscopy therapy using an Am-FCSEMS for p-OLT ABS is safe and effective,with the stricture´s highresolution rate probably being due to the absence of stent migration.
Research perspectives
No complications occurred during stent removal.In this study,no serious complications or deaths related to endoscopic treatment were reported.The average follow-up of patients who had stricture resolution after removal of the metallic stent was 411 d.There was no ABS recurrence during follow-up.This positive result may be related to the prolonged maintenance of the metallic stent,which was longer than 6 mo[2,5].
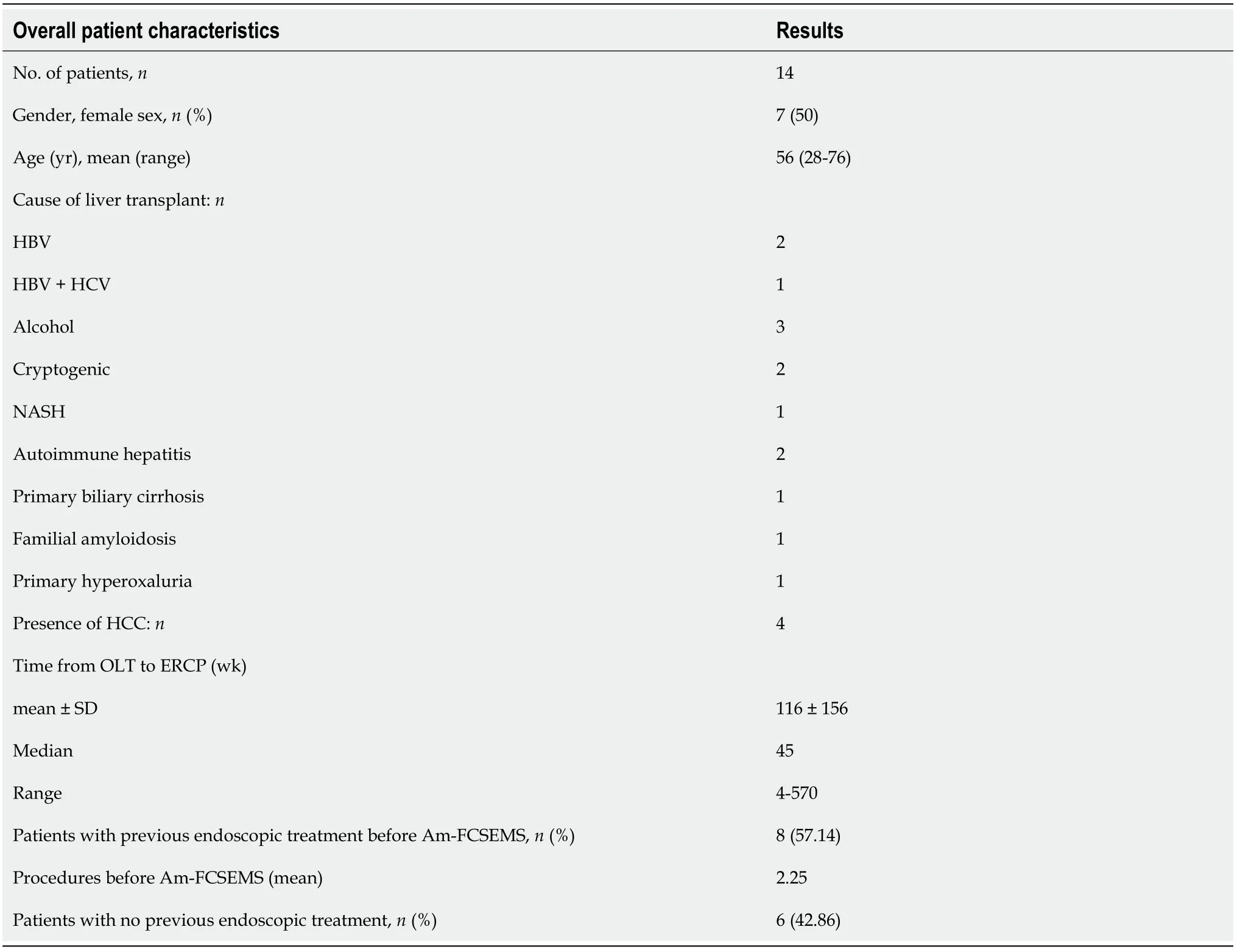
A total of 17 patients were included.Three patients were excluded due to loss to follow-up before stent removal (12 mo) (Figure 2).The average age of the 14 patients included and followed was 56 years (range: 28-76);7 women had an average age of 42 ± 11.2 years,and 7 men had an average age of 69 ± 5.8 years.Patient characteristics are shown in Table 1.Among the 14 patients,8 (57.14%) had already undergone treatment with FCSEMS and/or MPSs,but endoscopic management was considered unsuccessful,with an average number of procedures before inclusion in this study of 2.25 ± 1.04 (range: 1-4).The other 6 patients (42.85%) received an Am-FCSEMS as the first treatment.Regardless of previous treatment,the average interval from p-OLT to the first ERCP was 116 wk (range: 4-570).The average duration of placement of an Am-FCSEMS in this study was 362 ± 109 d (range: 226-609).The length of stent placement was 6 cm in 8 patients and 8 cm in 6 patients.Technical success (stent placement) occurred in all 14 patients (100%).The clinical follow-up after stent removal was 411 ± 172 d (range: 55-692).All stents were removed using foreign body forceps or snares without any technical difficulty (Figure 1C).
Pinheiro LW,Martins FP,Contini MLC,and De Paulo GA contributed to the data acquisition;Pinheiro LW,De Paulo GA,Ferrari AP,and Della Libera E contributed to the data analysis and interpretation;Pinheiro LW contributed to the elaboration of article draft;Martins FP and Contini MLC contributed to the elaboration and review of article draft,critical review for important intellectual content;De Paulo GA contributed to the critical review of final paper for important intellectual content;Ferrari AP and Della Libera E contributed to the critical review and approval of the final submitted version.
This retrospective study was approved by the Institution's Human Research Committee of Hospital Israelita Albert Einstein (No.37755020.3.0000.0071).
All study participants,or their legal guardian,provided informed written consent.
No additional data are available.
When the saint saw that the prince was not to be moved, he said: Learn and know, O youth! that Waq of Qaf is in the Caucasus and is a dependency of it
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) licence,which permits others to distribute,remix,adapt,and build upon this work noncommercially and licence their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See https://creativecommons.org/Licenses/by-nc/4.0/
Brazil
Larissa Wermelinger Pinheiro 0000-0003-2272-4715;Fernanda Prata Martins 0000-0002-7017-9910;Gustavo Andrade De Paulo 0000-0002-7926-9373;Mônica Lúcia Campos Contini 0000-0002-1532-787X;Angelo Paulo Ferrari 0000-0002-7062-288X;Ermelindo Della Libera 0000-0002-1098-7975.
Yan JP
A
Yan JP
1 Williams ED,Draganov PV.Endoscopic management of biliary strictures after liver transplantation.
2009;15: 3725-3733 [PMID: 19673012 DOI: 10.3748/wjg.15.3725]
2 Thuluvath PJ,Pfau PR,Kimmey MB,Ginsberg GG.Biliary complications after liver transplantation: the role of endoscopy.
2005;37: 857-863 [PMID: 16116539 DOI: 10.1055/s-2005-870192]
3 Pascher A,Neuhaus P.Biliary complications after deceased-donor orthotopic liver transplantation.
2006;13: 487-496 [PMID: 17139421 DOI: 10.1007/s00534-005-1083-z]
4 Ryu CH,Lee SK.Biliary strictures after liver transplantation.
2011;5: 133-142 [PMID: 21814591 DOI: 10.5009/gnl.2011.5.2.133]
5 Coté GA,Slivka A,Tarnasky P,Mullady DK,Elmunzer BJ,Elta G,Fogel E,Lehman G,McHenry L,Romagnuolo J,Menon S,Siddiqui UD,Watkins J,Lynch S,Denski C,Xu H,Sherman S.Effect of Covered Metallic Stents Compared With Plastic Stents on Benign Biliary Stricture Resolution: A Randomized Clinical Trial.
2016;315: 1250-1257 [PMID: 27002446 DOI: 10.1001/jama.2016.2619]
6 Devière J,Nageshwar Reddy D,Püspök A,Ponchon T,Bruno MJ,Bourke MJ,Neuhaus H,Roy A,González-Huix Lladó F,Barkun AN,Kortan PP,Navarrete C,Peetermans J,Blero D,Lakhtakia S,Dolak W,Lepilliez V,Poley JW,Tringali A,Costamagna G;Benign Biliary Stenoses Working Group.Successful management of benign biliary strictures with fully covered self-expanding metal stents.
2014;147: 385-95;quiz e15 [PMID: 24801350 DOI: 10.1053/j.gastro.2014.04.043]
7 Martins FP,De Paulo GA,Contini MLC,Ferrari AP.Metal versus plastic stents for anastomotic biliary strictures after liver transplantation: a randomized controlled trial.
2018;87: 131.e1-131.e13 [PMID: 28455159 DOI: 10.1016/j.gie.2017.04.013]
8 Sharma S,Gurakar A,Jabbour N.Biliary strictures following liver transplantation: past,present and preventive strategies.
2008;14: 759-769 [PMID: 18508368 DOI: 10.1002/lt.21509]
9 Krok KL,Cárdenas A,Thuluvath PJ.Endoscopic management of biliary complications after liver transplantation.
2010;14: 359-371 [PMID: 20682241 DOI: 10.1016/j.cld.2010.03.008]
10 Jiménez-Pérez M,Melgar Simón JM,Durán Campos A,González Grande R,Rodrigo López JM,Manteca González R.Endoscopic Management of Post-Liver Transplantation Biliary Strictures With the Use of Fully Covered Metallic Stents.
2016;48: 2510-2514 [PMID: 27742337 DOI: 10.1016/j.transproceed.2016.09.008]
11 Bordaçahar B,Perdigao F,Leblanc S,Barret M,Duchmann JC,Guillaumot MA,Chaussade S,Scatton O,Prat F.Clinical efficacy of anti-migration features in fully covered metallic stents for anastomotic biliary strictures after liver transplantation: comparison of conventional and anti-migration stents.
2018;88: 655-664 [PMID: 30003877 DOI: 10.1016/j.gie.2018.06.035]
12 García-Pajares F,Sánchez-Antolín G,Pelayo SL,Gómez de la Cuesta S,Herranz Bachiller MT,Pérez-Miranda M,de La Serna C,Vallecillo Sande MA,Alcaide N,Llames RV,Pacheco D,Caro-Patón A.Covered metal stents for the treatment of biliary complications after orthotopic liver transplantation.
2010;42: 2966-2969 [PMID: 20970584 DOI: 10.1016/j.transproceed.2010.07.084]
13 Kahaleh M,Behm B,Clarke BW,Brock A,Shami VM,De La Rue SA,Sundaram V,Tokar J,Adams RB,Yeaton P.Temporary placement of covered self-expandable metal stents in benign biliary strictures: a new paradigm?
2008;67: 446-454 [PMID: 18294506 DOI: 10.1016/j.gie.2007.06.057]
14 Traina M,Tarantino I,Barresi L,Volpes R,Gruttadauria S,Petridis I,Gridelli B.Efficacy and safety of fully covered selfexpandable metallic stents in biliary complications after liver transplantation: a preliminary study.
2009;15: 1493-1498 [PMID: 19877248 DOI: 10.1002/lt.21886]
15 Tarantino I,Traina M,Mocciaro F,Barresi L,Curcio G,Di Pisa M,Granata A,Volpes R,Gridelli B.Fully covered metallic stents in biliary stenosis after orthotopic liver transplantation.
2012;44: 246-250 [PMID: 22354824 DOI: 10.1055/s-0031-1291465]
杂志排行

World Journal of Gastrointestinal Endoscopy的其它文章
- Simulation-based mastery learning in gastrointestinal endoscopy training
- Endoscopic ultrasound elastography for malignant pancreatic masses and associated lymph nodes:Critical evaluation of strain ratio cutoff value
- Screening for hilar biliary invasion in ampullary cancer patients
- Clinical profile,diagnostic yield,and procedural outcomes of single balloon enteroscopy: A tertiary care hospital experience
- Role of endoscopic ultrasound in evaluation of patients with missed common bile duct stones
- Isolated esophageal tuberculosis:A case report