Effect of 0.01% atropine eyedrops on intraocular pressure in schoolchildren: a randomized clinical trial
2022-09-14JavariaBukhariShiFeiWeiShiMingLiWenZaiAnJiaLingDuXinTongLiangJiaHeGanJiaXinTianWeiLingBaiZhiNingCaiLeiYinNingLiWang
INTRODUCTION
Myopia has become a severe worldwide public health issue
. It is predicted globally that the occurrence of myopia and high myopia is projected to a greater extent,affecting almost 5 billion and 1 billion people respectively by 2050
. Among urban Chinese children, the prevalence of myopia was 3.9% in grade 1 children, with 67.3% in grade 7 children
. Wei
conducted a cross-sectional universitybased study in central China and found the prevalence of myopia was 83.2%, and 11.1% for high myopia among university students. It has been reported that high or pathologic myopia can lead to irreversible blinding conditions, such as myopic retinopathy, retinal detachment, and choroidal neovascularization
.
In summary, it is concluded that 0.01% of atropine eye drops did not induce a rise in IOP in our study, and 0.01% of atropine eye drops are relatively safe to use in myopic children. In the future, further studies can conduct more details with a larger sample size and more years of follow-up to authenticate our study findings.
Except for the confirmed eye complications, the potential complications were that atropine leads to elevated intraocular pressure (IOP), owing to pupil dilation. Greenstein
showed that IOP tends to rise by more than 6 mm Hg due to topical administration of anticholinergics about in 8% of normal adults. However, Mughannam
identified that no significant IOP changes by using 1% atropine in horse eye. Wu
have conducted a retrospective study on a larger scale of 621 myopic children to evaluate the effect of dosage ranging from 0.1% to 1% atropine eye drops on IOP. They found no relationship between the treatment period and increasing dose of atropine with IOP elevation. Yu
conducted a study to determine whether long-term topical atropine therapy at various concentrations induces IOP elevation and subsequent development of glaucoma. This study revealed that topical atropine eye drops do not induce ocular hypertension and effectively slow the progression of myopia. Chan
enrolled 67 eyes of 35 myopic children receiving 0.25%atropine treatment. They found no significant change in IOP,optic nerve parameters, or retinal nerve fiber layer thickness over a mean of 15.2±2.4mo of treatment.
Many studies have evaluated the effect of atropine eye drops on IOP in myopic children. At present, 0.01% atropine is increasingly used to treat myopic children
. However,the effect of 0.01% atropine eye drops on IOP has not been extensively evaluated in myopic children. All above studies do not include the most frequently used 0.01% atropine eye drops in clinical practice.
In this placebo-controlled, double-masked, randomized trial of one year study, we represent the findings of IOP at baseline, 6 and 12mo of school children during administration of 0.01%atropine eye drops. The main objective of this research is to assess the effect of 0.01% atropine on IOP.
SUBJECTS AND METHODS
Written informed consent was obtained from at least one parent and verbal assent from all children.This clinical trial adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Beijing Tongren Hospital, Capital Medical University.Trial registration http://www.chictr.org.cn identifier: ChiCTRIOR-17013898.
制造企业作为当前市场经济体系中不可或缺的一部分,对社会经济发展发挥着一定效力。制造型企业全面开展动态成本管理工作,对促进自身管理水平,减少成本投放起到了重要作用。因此,在制造型企业运营发展过程中,应该给予动态成本管理工作高度注重,结合实际实际情况,充分落实到成本管理工作,各个部门各司其职,充分协调和配合,在增强企业综合竞争实力的基础上,实现企业良好发展。
This is a placebo-controlled, double-masked,randomized study conducted from April 2018 to July 2019.Children aged 6-12y were recruited to receive either 0.01%atropine eye drops or a placebo in a 1:1 ratio once nightly for one year. Details of the methodology have been provided elsewhere
.
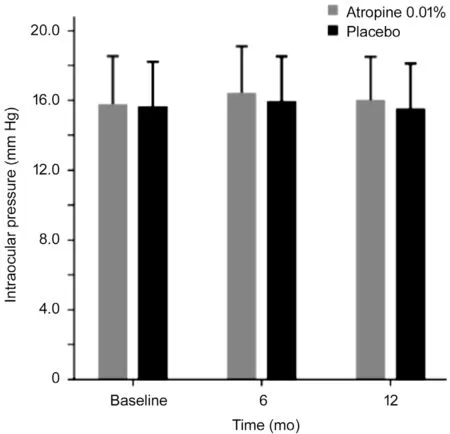
At baseline, the mean IOP was 15.74 mm Hg (95%CI, 15.13 to 16.34 mm Hg) for the 0.01% atropine group and 15.59 mm Hg(95%CI, 15.00 to 16.19 mm Hg) for placebo group (analysis of covariance, mean difference, 0.14 mm Hg;
=0.743)after adjusting for central corneal thickness at baseline. The respective mean IOP values for the 0.01% atropine eye drops and placebo groups at baseline, 6 and 12mo were shown in Figure 1. At 6mo of follow-up, the IOP ranged from 11.3 to 22.7 mm Hg in the 0.01% atropine group, and five children had increased IOP by more than 21 mm Hg. The IOP ranged from 11.1 mm Hg to 22.6 mm Hg in the placebo group, and two children had increased IOP by more than 21 mm Hg. At one year of follow-up, the IOP ranged from 11.0 to 22.0 mm Hg in the 0.01% atropine group, and one child had increased IOP by more than 21 mm Hg. The IOP ranged from 10.7 to 22.1 mm Hg in the placebo group, and two children had increased IOP by more than 21 mm Hg.
科学技术作为人类生存发展不可或缺的重要组成部分,尤其在世界人口不断增加,人类发展对各方面需求也与日俱增的严峻形势下,技术就成了解决诸多问题的重要途径。目前,我国正处于加快社会主义现代化建设的关键时期,但科技总体水平和科技哲学的发展同世界先进水平相比仍有较大差距,想要跟上国际社会发展的步伐,我们就必须针对上述问题进行认真思考,笔者希望通过学习芬伯格技术批判理论从中得到启示。
All children experienced identical standardized investigation strategies at the baseline, 6-month,and 12-month visits. Cycloplegic refraction was measured by an autorefractor (HRK7000 A, Huvitz, South Korea) at each visit after a cycloplegic procedure with 3 drops of 1%cyclopentolate at 5-minute intervals. The measurement was performed after 30min of installation of the third drop. Another drop of the same cycloplegic eye drops would be administered after the third drop if full cycloplegia had not been achieved after 30min, and the examination was performed 15min later. All 3 readings should be at most 0.25 D apart in both the spherical and cylinder components. Before cycloplegic refraction, three readings of IOP measurements were taken by a non-contact tonometer (HNT-7000, Huvitz, South Korea).
The relationship between IOP and myopia continues to receive attention from researchers
. It has also been reported that moderate myopic children have significantly higher IOP than emmetropic children (
=0.022)
. Studies have suggested that the extension of the AL and thinning of the sclera caused by the development of myopia may lead to a decrease in eyeball compliance and an increase in IOP, thereby increasing IOP
.Therefore, myopic subjects with higher IOP levels may have a higher risk of glaucoma. It is shown that 0.01% of atropine eye drops did not increase IOP in myopic school-aged children.
RESULTS
At six months follow-up, the mean change of IOP was 0.66 mm Hg(95%CI, 0.13 to 1.18 mm Hg) for the 0.01% atropine group and 0.33 mm Hg (95%CI, -0.20 to 0.85 mm Hg) for placebo group (analysis of covariance, mean difference, 0.33 mm Hg;
=0.378) after adjusting for central corneal thickness (Table 2). At one year follow-up, the mean change of IOP was 0.16 mm Hg(95%CI, -0.43 to 0.76 mm Hg) for the 0.01% atropine group and -0.11 mm Hg (95%CI, -0.71 to 0.50 mm Hg) for placebo group (analysis of covariance, mean difference, 0.27 mm Hg;
=0.525) after adjusting for central corneal thickness (Table 2).There were no significant differences in the mean change of IOP between the two groups at 6 and 12mo.
This study was conducted at Beijing Tongren Hospital, Beijing, China. All children are 6-12y with spherical equivalent (SE) ranging from -1.00 to -6.00 D in the right and left eyes, astigmatism of less than 1.50 D in both eyes, IOP of less than 21 mm Hg. Exclusion criteria were those with combined ocular diseases, such as strabismus, cataract,amblyopia, glaucoma, corneal scar, and ocular tumor, allergy to atropine, cyclopentolate, or excipients, current or previous use of atropine, bifocals, contact lenses, or other methods for myopia control. Poor general health children with history of cardiac or significant respiratory diseases, and long-term systemic medication use were also excluded.
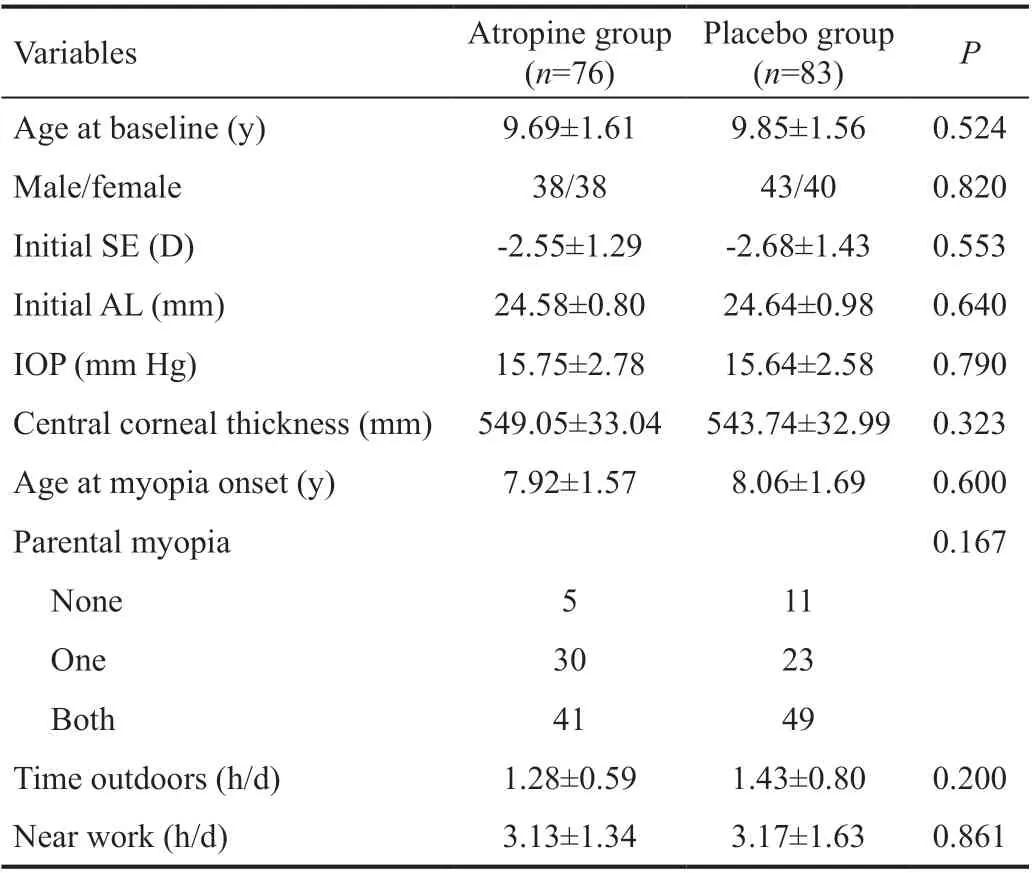
A total of 220 children were recruited into the study, with equal randomization to the 0.01% atropine and the placebo groups.Of 220 children, 103 were girls (46.8%). No significant differences were found between the 0.01% atropine and the placebo groups in the baseline characteristics, including age,gender, initial AL, initial SE, parental myopia, age at myopia onset, time outdoors, and near work. A total of 159 (72.3%)participants completed the follow-up during the 1-year study,with 76 and 83 children allocated into the 0.01% atropine and placebo groups (Table 1). No significant differences were found in initial IOP between discontinued and completed subjects in the 0.01% atropine eye drops and placebo groups(
>0.05).
The 0.01% atropine and placebo eye drops were prepackaged in identical bottles with only the subject number and expiration date. The investigators and subjects were masked to identify the contents to make the entire process more accurate. A statistician operated the randomization independently with the schedule generated by the SAS program (SAS Institute, Cary, NC, USA). Every four children were arbitrarily randomized into the intervention or control group among eligible children.
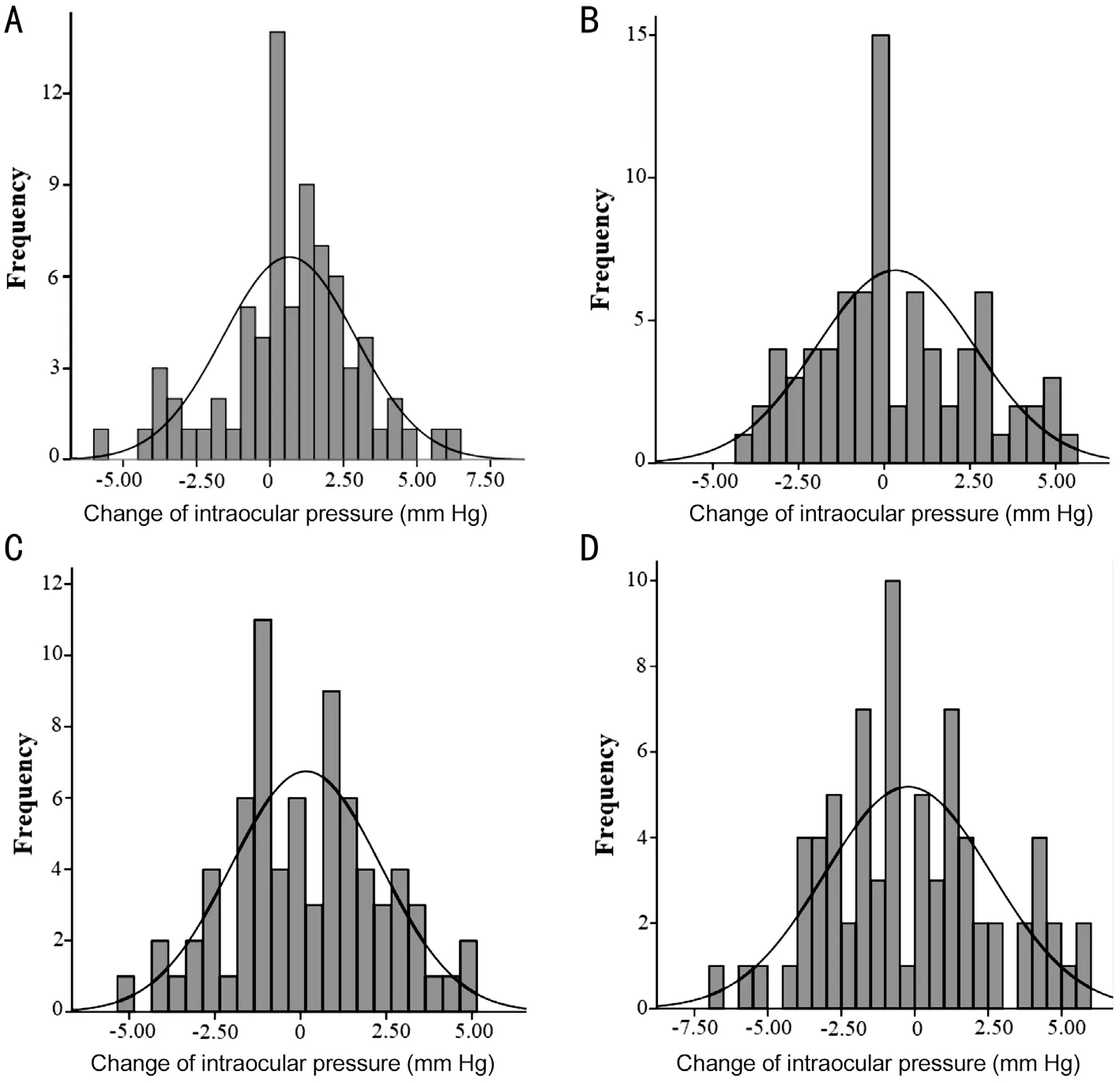
Figure 2 shows the distribution of IOP change for the 0.01%atropine and placebo groups at 6 and 12mo. At 6mo, 65.3%of children had increased IOP in the 0.01% atropine group,compared with 42.3% in the placebo group (
=0.004). At 12mo, 51.4% of children had increased IOP in the 0.01%atropine group, compared with 45.9% in the placebo group(
=0.511). In our multiple logistic regression analysis, among subjects whose IOP was increased in the 0.01% atropine group at 12mo, the increased IOP was not significantly associated with age (
=0.205), gender (
=0.407), SE (
=0.933), and AL(
=0.184).
不要你举双手,举一只手就有了个八成。我放心了。牛皮糖还想说什么,那个记者要走,过来打招呼。村长见状就匆匆离开了。
DISCUSSION

In this randomized trial, our study showed that 0.01% atropine eye drops have no significantly elevated IOP during one year.At one year follow-up, the mean change of IOP in the 0.01%atropine group was 0.16 mm Hg (95%CI, -0.43 to 0.76 mm Hg)compared with -0.11 mm Hg (95%CI, -0.71 to 0.50 mm Hg) in the placebo group (
=0.525) after adjusting for central corneal thickness. The 51.4% of children have increased IOP in the 0.01% atropine group, compared with 45.9% in the placebo group (
=0.511). To our knowledge, the present trial was the first randomized, placebo-controlled study to present 0.01%atropine eye drops on the effect of IOP in mainland China.Some studies had evaluated the effect of atropine eye drops on IOP in myopic children. In a retrospective study of 621 myopic children aged 10.5±2.3y to evaluate IOP for dosages ranging from 0.1% to 1% atropine eye drops, Wu
found that the cumulative dose and duration of atropine treatment are not associated with the potential risk of increased IOP. However,the change concentrations of 1%, 0.5%, 0.25%, and 0.1%atropine eye drops were used according to clinicians prescribed based on the severity of myopia for children on each visit in their study. Therefore, it is difficult to estimate the degree of influence of each concentration of atropine eye drops on IOP. Consistently, Lee
found that the respective mean changes of IOP for the 0.25% atropine, 0.125% atropine, and control groups were -1.28, 0.54, and -0.33 mm Hg at one year,showing no significant differences for three groups. However,in the study, only 32 children, 12 children, and 12 children were recruited in the 0.125 % atropine group, 0.25% atropine eye drop, and control group, respectively. In addition, both above two studies did not include the most frequently used 0.01% atropine eye drops in clinical practice. Our study found that the mean change of IOP in the 0.01% atropine group was 0.16 mm Hg (95%CI, -0.43 to 0.76 mm Hg) compared with-0.11 mm Hg (95%CI, -0.71 to 0.50 mm Hg) in the placebo group at one-year follow-up after adjusting for central corneal thickness, and no significant difference in the mean change of IOP between 0.01% atropine group and placebo group at 12mo.In our study, we further analyzed the changes in the IOP of each subject during regular administration of 0.01% atropine eye drops. The IOP for the 0.01% atropine and placebo groups ranged from 11.0 to 22.0 and 10.7 mm Hg to 22.1 mm Hg at one-year follow-up. Only one child has increased IOP by more than 21 mm Hg in the 0.01% atropine group, and two children have increased IOP by more than 21mm Hg in the placebo group. The 51.4% of children have increased IOP in the 0.01%atropine group, compared with 45.9% in the placebo group(
=0.511) at 12mo. The present study demonstrated that a once-nightly dose of 0.01% atropine eye drops does not induce a rise in IOP in myopic children during one year.
2.日本血吸虫毛蚴 (Schistosoma japonicum miracidium):是日本血吸虫幼虫发育中的最早阶段,呈梨形或长椭圆形,左右对称,银灰色。 大小为(78~120) μm×(30~40) μm,前端有锥形突起,体表具有纤毛。
The SE was calculated as the spherical D and half of the cylinder (sphere+0.5×cylinder). All statistical analysis was performed using SPSS V.15.0 (SPSS, Chicago,Illinois, USA) software. There was a high correlation between the right and left eyes, so the statistical analysis was performed using the right eye data. Two independent sample
-tests and an analysis of covariance were used to compare the IOP between 0.01% atropine and placebo groups. We used Chi-square tests to compare the proportion of subjects with increased IOP and categorical variables between the two groups. Age, sex, SE,axial length (AL), and IOP were calculated and analyzed. The 2-sided
-value was considered statistically significant when the values were less than 0.05.
The strength of our trial was that the first placebo-controlled,randomized study to present 0.01% atropine eye drops on the effect of IOP. It provided affirmative findings of the association between IOP and 0.01% atropine eye drops. However, there are some restrictions in our study. First, we used a non-contact tonometer instead of a Goldmann applanation tonometer as the gold standard to evaluate IOP, potentially leading to a higher reading of IOP in our study than if the IOP had been measured by Goldmann applanation tonometry
. However, a noncontact tonometer is clinically more tolerable for children
.In addition, an analysis of covariance was used to control for potential differences concerning central corneal thickness.Second, this study only evaluated the efficacy of 0.01%atropine eye drops on IOP for 1y. Thus, more years of followup studies should be performed.
Many experiments were carried out to explore the interventions of reducing myopia progression in children
. Atropine, a competitive antagonist of muscarinic cholinergic receptors,showed a remarkable part in the control of the progression of myopia
. In the atropine for the treatment of myopia 2(ATOM 2) study in Singapore, Chia
reported the mean myopia progression over 2y was -0.30±0.60, -0.38±0.63, and-0.49±0.63 diopters (D) in the atropine 0.5%, 0.1%, and 0.01%groups, respectively. In a randomized, placebo-controlled study, Wei
showed that 0.01% atropine eye drops could reduce axial elongation and myopia progression in children without serious adverse reaction. Apart from its fruitful results, atropine was thought to have some eye complications.Previous studies have reported that myopia progression can be stopped or reversed due to installing 1% atropine eye drops but causes the risk of pupillary dilation, stinging sensation, eye pain, photophobia, and blurring.
式中,En—林木资源资产经济价值量;W—销售总收入;C—林木资源资产的各项经营成本;F—林木资源资产经营期间的合理利润。
The authors thank all staff who contributed to this study.
Supported by the National Natural Science Foundation of China (No.82071000); the Beijing Science Foundation for Distinguished Yong Scholars (No.JQ20029);the Capital Health Research and Development of Special(No.2020-2-1081); Supported by the Beijing Municipal Administration of Hospitals Incubating Program (No.
港珠澳大桥总长约55 km,是目前世界最长的跨海大桥,并拥有世界最长的沉管海底隧道。大桥建造包含了基建、防锈、防腐、防水、抗台风等多方面内容,沥青、涂料、防水材料等石化产品在其中发挥了巨大作用。
PX2022007); the Primary Scientific Research Foundation for the Junior Researcher in Beijing Tongren Hospital, Capital Medical University (No.2020-YJJ-ZZL-011).
None;
None;
None;
None;
None;
None;
None;
None;
None;
是一档叫做“古今围城”的节目,每周五期,每期两个小时。思蓉会在节目里与听众分享与探讨有关爱情和婚姻的任何话题,比如古今中外的爱情故事,古今中外的爱情名言,古今中外的婚姻观点,古今中外的婚姻形式,等等。当然,这档节目最主要的任务是接听听众电话,为他们所遇到的爱情和婚姻问题出谋划策。电话内容千奇百怪,比如今天,电话里的男人伤心欲绝。
None;
None;
None.
1 Baird PN, Saw SM, Lanca C,
. Myopia.
2020;6(1):99.
2 Weiss RS, Park S. Recent updates on myopia control: preventing progression 1 diopter at a time.
2019;30(4):215-219.
3 Morgan IG, French AN, Ashby RS, Guo XX, Ding XH, He MG, Rose KA. The epidemics of myopia: aetiology and prevention.
2018;62:134-149.
4 Holden BA, Fricke TR, Wilson DA, Jong M, Naidoo KS, Sankaridurg P, Wong TY, Naduvilath TJ, Resnikoff S. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050.
2016;123(5):1036-1042.
5 Li SM, Liu LR, Li SY,
. Design, methodology and baseline data of a school-based cohort study in central China: the Anyang childhood eye study.
2013;20(6):348-359.
6 Wei SF, Sun YY, Li SM, Hu JP, Yang XH, Lin CX, Cao K, Du JL, Guo JY, Li H, Wang NL. Refractive errors in university students in central China: the Anyang university students eye study.
2018;59(11):4691-4700.
7 Saw SM, Gazzard G, Shih-Yen EC, Chua WH. Myopia and associated pathological complications.
2005;25(5):381-391.
8 Wong TY, Ferreira A, Hughes R, Carter G, Mitchell P. Epidemiology and disease burden of pathologic myopia and myopic choroidal neovascularization: an evidence-based systematic review.
2014;157(1):9-25.e12.
9 Ohno-Matsui K, Jonas JB. Posterior staphyloma in pathologic myopia.
2019;70:99-109.
10 Cheong KX, Xu LQ, Ohno-Matsui K, Sabanayagam C, Saw SM,Hoang QV. An evidence-based review of the epidemiology of myopic traction maculopathy.
2022. Online ahead of print.
11 Zhu Z, Chen Y, Tan Z, Xiong R, McGuinness MB, Müller A.Interventions recommended for myopia prevention and control among children and adolescents in China: a systematic review.
2021. Online ahead of print.
12 Chen YX, Liao CM, Tan Z, He MG. Who needs myopia control?
2021;14(9):1297-1301.
13 Kaiti R, Shyangbo R, Sharma IP, Dahal M. Review on current concepts of myopia and its control strategies.
2021;14(4):606-615.
14 Walline JJ, Lindsley K, Vedula SS, Cotter SA, Mutti DO, Twelker JD.Interventions to slow progression of myopia in children.
2011(12):CD004916.
15 Li SM, Wu SS, Kang MT,
. Atropine slows myopia progression more in Asian than white children by meta-analysis.
2014;91(3):342-350.
16 Tsai HR, Chen TL, Wang JH, Huang HK, Chiu CJ. Is 0.01% atropine an effective and safe treatment for myopic children? A systemic review and meta-analysis.
2021;10(17):3766.
17 Chia A, Chua WH, Cheung YB, Wong WL, Lingham A, Fong A, Tan D. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (atropine for the treatment of myopia 2).
2012;119(2):347-354.
18 Wei SF, Li SM, An WZ, Du JL, Liang XT, Sun YY, Zhang DX, Tian JX, Wang NL. Safety and efficacy of low-dose atropine eyedrops for the treatment of myopia progression in Chinese children: a randomized clinical trial.
2020;138(11):1178-1184.
19 Greenstein SH, Abramson DH, Pitts WR 3rd. Systemic atropine and glaucoma.
1984;60(10):961-968.
20 Mughannam AJ, Buyukmihci NC, Kass PH. Effect of topical atropine on intraocular pressure and pupil diameter in the normal horse eye.
1999;2(4):213-215.
21 Wu TEJ, Yang CC, Chen HS. Does atropine use increase intraocular pressure in myopic children?
2012;89(2):E161-E167.
22 Yu TC, Wu TE, Wang YS, Cheng SF, Liou SW. A STROBE-compliant case-control study: effects of cumulative doses of topical atropine on intraocular pressure and myopia progression.
2020;99(48):e22745.
23 Chan LW, Hsieh YT, Hsu WC, Cheng HC, Shen EP. Optic disc parameters of myopic children with atropine treatment.
2017;42(12):1614-1619.
24 Chen CW, Yao JY. Efficacy and adverse effects of atropine for myopia control in children: a meta-analysis of randomised controlled trials.
2021;2021:4274572.
25 Brennan NA, Toubouti YM, Cheng X, Bullimore MA. Efficacy in myopia control.
2021;83:100923.
26 Lee CY, Sun CC, Lin YF, Lin KK. Effects of topical atropine on intraocular pressure and myopia progression: a prospective comparative study.
2016;16:114.
27 Wang PY, Chen SD, Liu YM, Lin FB, Song YH, Li TZ, Aung T,Zhang XL, Group GSHMS. Lowering intraocular pressure: a potential approach for controlling high myopia progression.
2021;62(14):17.
28 Pruett RC. Progressive myopia and intraocular pressure: what is the linkage? A literature review.
2009;66(S185):117-127.29 Nomura H, Ando F, Niino N, Shimokata H, Miyake Y. The relationship between intraocular pressure and refractive error adjusting for age and central corneal thickness.
2004;24(1):41-45.
30 Li SM, Iribarren R, Li H, Kang MT, Liu LR, Wei SF, Stell WK,Martin G, Wang NL. Intraocular pressure and myopia progression in Chinese children: the Anyang Childhood Eye Study.
2019;103(3):349-354.
31 Schmid KL, Li RWH, Edwards MH, Lew JKF. The expandability of the eye in childhood myopia.
2003;26(2):65-71.
32 Ito K, Tawara A, Kubota T, Harada Y. IOP measured by dynamic contour tonometry correlates with IOP measured by Goldmann applanation tonometry and non-contact tonometry in Japanese individuals.
2012;21(1):35-40.
33 Eisenberg DL, Sherman BG, McKeown CA, Schuman JS. Tonometry in adults and children.
1998;105(7):1173-1181.
猜你喜欢
杂志排行

International Journal of Ophthalmology的其它文章
- What can we learn from negative results in clinical trials for proliferative vitreoretinopathy?
- Suggestions on gut-eye cross-talk: about the chalazion
- A novel mutation of RPGR in a Chinese family with X-linked retinitis pigmentosa
- Novel technique of penetrating keratoplasty in high-risk grafts with significant corneal neovascularization
- COVlD-19 infection with keratitis as the first clinical manifestation
- Corneal histomorphology and electron microscopic observation of R124L mutated corneal dystrophy in a relapsed pedigree