Metabolic-associated fatty liver disease is associated with low muscle mass and strength in patients with chronic hepatitis B
2022-09-01CecyMariadeLimaSantosMatheusDuarteBritoPedroAlvesSoaresVazdeCastroThaisPontellodeVriesNatalyLopesVianaMartaPaulaPereiraCoelhoOlvioBritoMalheiroTatianaBeringMariaCristinaGonzalezRosngelaTeixeiraRodrigoDiasCambraiaGif
Cecy Maria de Lima Santos, Matheus Duarte Brito, Pedro Alves Soares Vaz de Castro, Thais Pontello de Vries, Nataly Lopes Viana, Marta Paula Pereira Coelho, Olívio Brito Malheiro, Tatiana Bering, Maria Cristina Gonzalez, Rosângela Teixeira, Rodrigo Dias Cambraia, Gifone Aguiar Rocha, Luciana Diniz Silva
Cecy Maria de Lima Santos, Thais Pontello de Vries, Nataly Lopes Viana, Marta Paula Pereira Coelho, Rosângela Teixeira, Luciana Diniz Silva, Sciences Applied to Adult Health Care Post-Graduate Programme Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte 30130-100, Minas Gerais, Brazil
Cecy Maria de Lima Santos, Matheus Duarte Brito, Pedro Alves Soares Vaz de Castro, Thais Pontello de Vries, Nataly Lopes Viana, Rosângela Teixeira, Rodrigo Dias Cambraia, Luciana Diniz Silva, Outpatient Clinic of Viral Hepatitis, Instituto Alfa de Gastroenterologia, Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte 30130-100, Minas Gerais,Brazil
Matheus Duarte Brito, Pedro Alves Soares Vaz de Castro, Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte 30130-100, Minas Gerais, Brazil
Olívio Brito Malheiro, Department of Locomotor System, Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte 30130-100, Minas Gerais, Brazil
Tatiana Bering, Department of Food and Nutrition, Universidade Federal de Mato Grosso, Cuiab á 78060-900, Mato Grosso, Brazil
Maria Cristina Gonzalez, Postgraduate Program in Health and Behaviour, Catholic University of Pelotas, Pelotas 96015-560, Rio Grande do Sul, Brazil
Gifone Aguiar Rocha, Laboratory of Research in Bacteriology, Faculdade de Medicina,Universidade Federal de Minas Gerais, Belo Horizonte 30130-100, Minas Gerais, Brazil
Luciana Diniz Silva, Department of Internal Medicine, Universidade Federal de Minas Gerais,Belo Horizonte 30130-100, Minas Gerais, Brazil
Abstract BACKGROUND Although the prognostic relevance of sarcopenia has been increasingly recognised in the context of liver disease, there is a paucity of data evaluating body composition in patients with chronic hepatitis B (CHB). Beyond virus-related factors, nutritional and metabolic aspects can be associated with skeletal muscle abnormalities in these patients and should not be disregarded.AIM To evaluate the association between components of sarcopenia and demographic, clinical, lifestyle,nutritional, and biochemical variables in CHB patients.METHODS Dual-energy X-ray absorptiometry (DXA) was used to assess muscle mass by quantifying appendicular lean mass (ALM) adjusted for body mass index (ALMBMI). Muscle function was evaluated by hand grip strength (HGS) and the timed up and go test. Metabolic-associated fatty liver disease (MAFLD) was defined according to the criteria proposed by an international expert panel. A body shape index and the International Physical Activity Questionnaire were used to assess central obesity and physical activity level, respectively.RESULTS This cross-sectional study included 105 CHB outpatients followed at the tertiary care ambulatory centre (mean age, 48.5 ± 12.0 years; 58.1% males; 76.2% without cirrhosis; 23.8% with compensated cirrhosis). The DXA-derived fat mass percentage was inversely correlated with the ALMBMI (r = -0.87) and HGS (r = - 0.63). In the multivariable analysis, MAFLD, sedentarism and central obesity were positively and independently associated with low ALMBMI. MAFLD and central obesity were independently associated with low HGS.CONCLUSION MAFLD and central obesity were associated with low muscle mass and strength in patients with chronic hepatitis B, independent of the liver disease stage.
Key Words: Chronic hepatitis B; Appendicular lean mass; Muscle strength; Metabolic associated fatty liver disease; Central obesity; Physical performance
lNTRODUCTlON
Globally, approximately 462 million adults are underweight, whereas 1.9 billion are either overweight or obese[1,2]. In this scenario, according to the World Health Organization definition, the double burden of malnutrition is “characterized by the coexistence of undernutrition along with overweight, obesity or diet-related noncommunicable diseases, within individuals, households and populations, and across the life-course”[1,2]. Translating this definition into the hepatic disease context, several investigations have demonstrated that malnutrition and overweight can simultaneously be present in a patient[3-8].Malnutrition contributes to the development of skeletal muscle abnormalities[3,4]. The loss of skeletal muscle mass, function and performance is considered primary when it is associated with ageing itself,i.e., primary sarcopenia; however, it can also be related to chronic diseases,i.e., secondary sarcopenia[9,10]. Furthermore, abnormalities in muscle mass and function may coexist with obesity, resulting in sarcopenic obesity, which is associated with liver-related complications and adverse outcomes[5,6]. The interaction between skeletal muscle abnormalities and metabolic factors such as obesity, insulin resistance and metabolic syndrome play a key role in the progression of liver fibrosis[5-8].
In real-world settings, researchers have identified an overlap between two or more factors associated with the progression of fibrosis in a substantial number of patients with cirrhosis[11-15]. Although in patients with chronic hepatitis B (CHB), long-term antiviral therapy is effective in discontinuing viral replication and reducing the development of cirrhosis and/or hepatocellular carcinoma (HCC),subgroups of patients are still prone to fibrosis progression, even achieving virological sustained response with potent nucleos(t)ide analogue therapy[16-18]. This evidence sheds light on putative risk factors for fibrosis advancement other than hepatitis B virus (HBV)-related factors. Among these factors,host and environmental factors should be highlighted, such as nutritional and metabolic characteristics.
With respect to nutritional status, in a previous study including individuals chronically infected with HBV or hepatitis C virus (HCV), sarcopenia was identified in 7.1%, 11.8%, and 21.9% of noncirrhotic,compensated cirrhotic (Child-Turcotte-Pugh A), and decompensated cirrhotic (Child-Turcotte-Pugh B/C) patients, respectively[19]. More recently, Han and colleagues examined the influence of sarcopenia on liver fibrosis among 506 patients with CHB[7]. Sarcopenia was significantly associated with liver disease severity, especially among HBV-positive subgroups with obesity, insulin resistance, metabolic syndrome and liver steatosis[7]. Although secondary sarcopenia is a well-known predictor of liver fibrosis in patients with nonalcoholic fatty liver disease (NAFLD), the interaction between sarcopenia and CHB is poorly understood. On the other hand, in line with the increasing prevalence of NAFLD, the coexistence of HBV infection and fatty liver disease has frequently been identified worldwide[8.20].
Recently, an international expert panel outlined metabolic-associated fatty liver disease (MAFLD) as hepatic steatosis in the presence of overweight, diabetes, and/or a combination of other metabolic disorders[21]. In contrast to the previous criteria for the diagnosis of NAFLD, the diagnosis of MAFLD is based on the degree of metabolic derangement and does not require the exclusion of other aetiologies of hepatic disease[21]. The role of superimposed MAFLD in CHB progression is still unclear. Despite the risks and consequences associated with low muscle mass in subjects chronically infected with HBV,there is a paucity of data evaluating body composition in this population. Thus, the aim of this study was to investigate the association between components of sarcopenia and demographic, clinical,lifestyle, nutritional, and biochemical variables in patients chronically infected with HBV.
MATERlALS AND METHODS
This was a cross-sectional study comprising 105 consecutive outpatients who were aged > 18 years with confirmed CHB diagnosis attending the Viral Hepatitis Outpatient Clinic, University Hospital, Belo Horizonte, Brazil, between 2017 and 2020. Each patient met the inclusion criteria of the study for CHB as confirmed by the presence of specific HBV seromarkers and HBV-DNA.
The Viral Hepatitis Outpatient Clinic is an outpatient care ambulatory of a metropolitan tertiary teaching hospital that admits patients for the treatment of chronic viral hepatitis. All participants signed the informed consent form. The study was designed and conducted following the Declaration of Helsinki and was approved by the Ethics Committee of Federal University of Minas Gerais/UFMG(ETIC 0404.0.203.000 - 10; CAAE, 07761212.2.0000.5149).
Study population
All patients were screened for other hepatic diseases. The following patients were excluded from the study: those aged < 18 years; women who were pregnant or breastfeeding; those with hepatic encephalopathy, HBV/HCV or HBV/human immunodeficiency virus (HIV) coinfection; patients who had causes of liver disease other than HBV infection and advanced diseases such as chronic kidney disease,heart failure, chronic pulmonary disease, and neoplasia, including HCC. Patients were also excluded if they were using drugs known to be associated with fatty liver disease.
Since fluid overload interferes with body composition assessment, the Child-Pugh-Turcotte score was assessed for each patient, and those with a Child-Pugh-Turcotte score > 7 points and/or decompensated cirrhosis were not included in the study[22,23]. The diagnosis of cirrhosis was based on standard clinical, biochemical, radiological, and histological parameters[15]. Each patient underwent a detailed physical examination, particularly for the presence of bilateral lower extremity oedema and ascites.Additionally, all included patients had serum albumin levels ≥ 3.5 g/dL and the absence of ascites confirmed by abdominal ultrasound.
Laboratory parameters
Blood samples were obtained from each patient after 12 h of overnight fasting for HBV diagnosis and biochemical and haematological evaluation. Fasting blood glucose levels, glycated haemoglobin, total cholesterol and fractions, triglycerides, alanine aminotransferase (ALT), aspartate aminotransferase(AST), gamma-glutamyl transpeptidase, alkaline phosphatase, albumin, total bilirubin, prothrombin activity, complete blood count test and creatinine were evaluated by routine laboratory methods.
Diagnosis and classification of chronic hepatitis B virus infection
CHB infection was classified as recommended by the EASL Clinical Practice Guidelines[24]. HBeAgpositive or HBeAg-negative chronically infected patients who presented HBV DNA > 2000 IU/mL, ALT> 2 × upper limits of normal and/or at least moderate liver necroinflammation or fibrosis during clinical follow-up were categorised as having CHB and underwent antiviral treatment[24]. All of them had undetectable HBV-DNA viral loads. Patients who were treatment-naïve with intrinsically low HBV viral load met the HBV chronic infection classification[24].
HBV status and HBV-DNA viral load were evaluated by chemiluminescence immunoassay (Ortho-Clinical Diagnostics™ VITROS™, Cumberland County, NJ) and a commercial test (Abbott Real Time HBV Viral Load, Lake Bluff, IL), respectively, according to the manufacturers’ instructions.
Clinical comorbidities and metabolic derangement evaluation
Hypertension, diabetes mellitus, dyslipidaemia and metabolic syndrome were defined in accordance with international guidelines[25-28]. Hepatic steatosis was diagnosed as the presence of fatty liver determined by ultrasound and/or histological assessment. The diagnosis of liver steatosis on ultrasound was based on increased hepatic echogenicity, hepatic attenuation of the ultrasound beam and hepatorenal index[29-31]. In addition, the hepatic steatosis index (HSI), a quantitative method for the evaluation of fatty liver disease validated for patients with HBV, was calculated according to the following formula: 8 × (ALT/AST ratio) + BMI (+2, if female; +2, if diabetes mellitus)[32,33]. MAFLD was defined according to the International Expert Consensus Statement[21].
Liver histological assessment
The METAVIR score was used to assess the severity of fibrosis and the degree of liver inflammation/activity[34]. The grading and staging of fatty liver were defined using criteria proposed by Bruntet al[35] for histological lesions.
Lifestyle assessment
A current/past history of alcohol use was investigated as part of the lifestyle evaluation. Risky alcohol consumption was defined as a consumption of more than 20 g and 30 g of alcohol daily for women and men, respectively, for more than five years[36].
Participant habitual physical activity was assessed using the International Physical Activity Questionnaire (IPAQ) short version validated for the Brazilian population[37]. Physical activity was dichotomised into normal [moderate-to-high categorical scale of IPAQ ≥ 600 metabolic equivalent of task (MET)-min/wk] or low (< 600 MET-min/wk). A trained person administered the questionnaires.
Anthropometry assessment and nutritional status
A nutritionist carried out all nutritional evaluations (C.M.L.S.). Weight and height were measured with a mechanical platform-type Filizola®(Filizola, São Paulo, Brazil). Light indoor clothing could be worn,excluding sweaters, belts, and shoes. We used Quetelet's formula to calculate BMI as a ratio between weight in kilograms and height in metres squared (kg/m2), and for elderly subjects, we used the Lipschitz classification[38,39].
Waist circumference (WC) was measured in the horizontal plane midway between the lower rib edge and the upper iliac crest in the standing position with a nonstretchable tape (cm). Central obesity was diagnosed as waist circumference > 102 cm in males and > 88 cm in females[28].
“A body shape index” (ABSI), an indirect measure of central obesity, was calculated as WC/(BMI2/3×height1/2) and expressed in m11/6.kg−2/3[40-42]. The original ABSI values were < 0.1 and were multiplied by 1,000 to derive numbers on the order of magnitude of WC[42]. The fourth sex-specific quartile was used as the cut-off point to categorise the patients into the following groups: “higher ABSI” (> 82.4 for men and > 83.2 for women) and “nonhigher ABSI”.
Malnutrition was evaluated by using subjective global assessment (SGA). Patients were classified as follows: Nourished (SGA A), suspected to be malnourished or moderately malnourished (SGA B), and severely malnourished (SGA C)[43].
Evaluation of body composition
Whole-body dual-energy X-ray absorptiometry (DXA) exams were performed according to the procedures recommended by the manufacturer on a Discovery W densitometer (Hologic, Inc., Bedford,MA), software version 3.3.0. All procedures were carried out by blinded assessors and interpreted by the same operator (O. B. M.). The analysis included whole-body DXA measurements as fat mass (FM)and appendicular lean mass (ALM) or appendicular lean soft tissue (ALST), which is the sum of the lean mass of the arms and legs (kg)[44]. ALM was adjusted for BMI (ALMBMI), and patients in the first sexspecific quintile (< 0.767 for men and < 0.501 for women) were considered to have low ALMBMI. The criteria were adapted from the Foundation for the National Institutes of Health Biomarkers Consortium Sarcopenia Project consensus (FNIH Consensus)[10].
High DXA-derived FM was considered greater than 27.0% for men and 38.0% for women[45].
Handgrip strength assessment
Handgrip strength, used to evaluate muscle strength, was measured with the hand-held dynamometer JAMAR®(Asimow Engineering Co., Los Angeles, CA). Subjects were seated with their elbows flexed at 90° and supported at the time of the measurement[46]. During handgrip strength measurement, we asked the patient to grip the dynamometer with maximum strength and hold the grip for 3 s. We collected three measurements from each hand in an alternating manner, and the maximum strength was defined as the greatest of the six measurements[46]. Handgrip strength was considered low when it was< 30 kg for males and < 20 kg for females (1.0 SD below the mean of a reference Brazilian population)[47,48].
Timed up-and-go test
The timed up-and-go test (TUG) measures the time it takes an individual to stand up from an armchair,walk a distance of three metres, turn, walk back to the chair and sit down again[49]. Patients in the fourth age- and sex-specific quartile were considered to have low physical performance according to the TUG values [for both men and women (age in years), 20-29 years, 9 s; 30-39 years, 10 s; 40-39 years, 11 s;50-59 years, 12 s. For men 60-80 years, 14 s and for women 60-80 years, 18 s] modified from Furlanettoet al[50].
To improve the accuracy of the results, biochemical evaluation, abdominal ultrasound, liver biopsy,DXA, interview as well as lifestyle evaluation, anthropometric assessment and nutritional status were obtained from each patient at the time of her or his inclusion in the study.
Statistical analysis
Data were analysed with IBM SPSS (IBM Corp., Armonk, NY), statistical software package version 26.0.Descriptive statistics were used to provide information regarding the demographic, clinical, metabolic,lifestyle, nutritional, and biochemical data. The Shapiro-Wilk test was used to evaluate whether the data were normally distributed. For the comparison of percentages, the asymptotic Pearson'sχ2test was used.The Mann-Whitney U test or Kruskal-Wallis test was used for comparing the medians, and Student's t test or ANOVA was used for comparing the means.
The strength of the associations between, FM and ALMBMIand FM and HGS was analysed by Spearman's correlation. The correlation coefficient was interpreted as follows: 0.00-0.30 negligible, 0.30-0.50 Low, 0.50-0.70 moderate, 070-0.90 high and 0.90-1.00 very high[51].
Multiple logistic regression models were used to appraise the factors independently associated with the components of sarcopenia, low ALMBMI, low HGS and low physical performance (dependent variables, categorised as 0, absent or 1, present). We selected the following independent variables:demographics (age and sex); anthropometrics (ABSI); stage of liver disease (with compensated cirrhosis and without cirrhosis); metabolic derangement (MAFLD); sedentary lifestyle (IPAQ < 600 METmin/wk); and prescribed medications (polypharmacy). Associations were evaluated by univariate analysis, and all variables withPvalues < 0.20 were included in the full models of logistic regression.Odds ratios and 95% confidence intervals were used as estimates of the risk. The Hosmer-Lemeshow test was used to assess the adequacy of the models.
To avoid the effect of collinearity, muscle abnormalities, low ALMBMIand low HGS were not included in the same logistic regression models.
The level of significance was set atPvalues ≤ 0.05.
RESULTS
Characteristics of the study population
The baseline characteristics of the patients are summarised in Table 1. The mean age of the patients was 48.5 ± 12.0 years, and 58.1% were men. At clinical follow-up, 61 (58.1%) and 44 (41.9%) patients met the criteria of CHB and HBV chronic infection, respectively[24]. Those categorised as CHB underwent antiviral treatment for at least 12 mo and had undetectable viral loads (Table 1). Out of 105 patients, 94(89.5%) were diagnosed as HBeAg-negative, and 25/105 (23.8%) had compensated cirrhosis, which was more frequent in men than in women.

Table 1 Main characteristics of the patients with chronic hepatitis B according to sex (n = 105)
With respect to the nutritional data, ALMBMI(0.882 ± 0.147vs0.589 ± 0.097;P <0.001) and HGS (43.5 ±11.0vs24.9 ± 4.8;P <0.001) were significantly higher in men than in women. Women had a significantly higher mean BMI (27.4 ± 4.6vs25.5 ± 4.1 kg/m2;P =0.02) and mean FM (40.9 ± 5.2vs26.7 ± 6.2;P <0.001) than men. Most patients (98.1%) were well nourished according to the SGA [SGA = 103 and SGB= 2 (1.9%)]. No differences were observed in mean or median of waist circumference (90.3 ± 12.2vs89.9± 12.2 cm;P =0.87), ABSI [80.0 (77.0; 82.4)vs78.9 (75.7; 83.2) (m11/6. kg-2/3);P =0.37] or the timed up and go test [10.0 (8.9; 11.7)vs10.0 (8.1; 10.9) (sec);P =0.42] between men and women, respectively.
Overweight/obesity (57.1%) was the most frequent clinical and metabolic abnormality, followed by hepatic steatosis (38.1%), blood hypertension (32.4%), dyslipidaemia (18.1%), metabolic syndrome(18.1%) and diabetes mellitus (10.5%). As an elevated prevalence of clinical and metabolic abnormalities was identified, the patients were categorised into non-MAFLD and MAFLD groups. MAFLD was diagnosed in 29 of 105 patients with CHB. Among these patients, 14 (48.2%) had overweight or obesity;20.7% had overweight/obesity, hypertension and diabetes mellitus; 10.3% had overweight/obesity,hypertension and dyslipidaemia; 6.9% had overweight/obesity, hypertension, diabetes mellitus and dyslipidaemia; 6.9% had hypertension and diabetes mellitus; 3.5% had hypertension and dyslipidaemia;and 3.5% had dyslipidaemia.
Concerning hepatic steatosis assessment, all patients underwent liver ultrasound evaluation, and liver biopsy was available in 41 patients (39%). In the MAFLD group, hepatic steatosis was diagnosed by ultrasound in 17/29 (58.6%) patients and by both histological analysis and ultrasound in 12 (41.4%)patients. The HIS [median (interquartile range, 25th- 75thpercentile)] was significantly higher in the MAFLD group [42.5 (37.6-44.8)] than in the non-MAFLD group [34.8 (30.9-40.4);P <0.001].
Clinical characteristics of patients with or without muscle abnormalities
Out of 105 participants, 8 (7.6%) had low ALMBMIand HGS combined, and 5 (4.8%) had low ALMBMI,HGS and physical performance combined.
Patients with low ALMBMIwere older, had a higher prevalence of general or central obesity, high DXA-derived FM, low HGS, compensated cirrhosis, clinical and metabolic disorders, sedentary lifestyle and risky alcohol consumption (Supplementary Table 1). General or central obesity, high FM, low ALMBMI, polypharmacy, and clinical and metabolic abnormalities were more frequent in patients with low HGS than in those without low muscle strength (Supplementary Table 2). There were no significant differences between low ALMBMI(Figure 1A) and low HGS (Figure 1B) within different age range groups.

Figure 1 Mean percentage of patients chronically infected with hepatitis B virus. A: With low appendicular lean mass adjusted for body mass index(BMI); B: Low handgrip strength adjusted by BMI according to age range (Student's t-test, P ≤ 0.05).
Polypharmacy tended to be more frequent in CHB patients with low physical performance (19.4%)than in those without abnormal functional performance (5.4%,P =0.06) (Supplementary Table 3).Angiotensin-converting inhibitor, angiotensin-receptor blockers, amlodipine, amitriptyline, atenolol,carvedilol, diltiazem, entecavir, furosemide, hydrochlorothiazide, indapamide, insulin, metformin,omeprazole, propranolol, spironolactone, statin and tenofovir disoproxil fumarate were the medications used by the patients. None of the individuals taking statins had myalgia, muscle weakness or increased creatine phosphokinase.
Neither ALMBMInor muscle function was associated with antiviral therapy use. All patients with coexisting low ALMBMI, HGS and physical performance had MAFLD, central obesity, sedentary lifestyle and high FM (Supplementary Table 4).
Correlation between DXA-derived fat mass percentage and muscle abnormalities
DXA-derived FM was inversely correlated with ALMBMI(r= -0.87;P <0.001) (Figure 2A) and HGS (r= -0.63;P <0.001) (Figure 2B).

Figure 2 Correlation between Dual-energy X-ray absorptiometry-derived fat mass percentage and muscle abnormalities. A: Correlations between fat mass percentage and appendicular lean mass adjusted for body mass index; B: Correlations between fat mass percentage and handgrip strength in patients chronically infected with hepatitis B.
Liver necroinflammatory activity and muscle abnormalities
Neither ALMBMInor muscle function was associated with abnormal aminotransferase levels.
Factors associated with low appendicular lean mass adjusted for body mass index
In the univariate analysis, age, high ABSI, compensated cirrhosis, MAFLD and low IPAQ (< 600 METmin/wk) were included (Table 2). High ABSI, MAFLD and sedentary lifestyle remained positively and independently associated with low ALMBMIin the multivariable analysis (Table 2). In patients with hepatic steatosis, HSI was inversely correlated with ALMBMI(r= -0.50;P <0.001) (Figure 3A), and HSI was higher in patients with low ALMBMIthan in those without (Figure 3B).

Table 2 Univariate and multivariable analyses of variables associated with skeletal muscle abnormalities and function in 105 patients with chronic hepatitis B
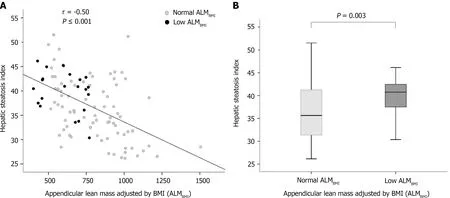
Figure 3 Factors associated with low appendicular lean mass adjusted for body mass index. A: Correlation between hepatic steatosis index and appendicular lean mass adjusted by body mass index in patients chronically infected with hepatitis B; B: Box plots representing the hepatic steatosis index. The upper and lower limits of the boxes represent the 75th and 25th percentiles, respectively; the horizontal bar across the box indicates the median, and the ends of the vertical lines indicate the minimum and maximum data values (P = 0.003).
Factors associated with low handgrip strength adjusted for body mass index
High ABSI, compensated cirrhosis, MAFLD and polypharmacy were included in the univariate analysis(Table 2). High ABSI and MAFLD remained positively and independently associated with low HGS in the univariate analysis (Table 2).
Factors associated with low physical performance
Age and polypharmacy were included in the univariate analysis (Table 2). Polypharmacy remained positively and independently associated with low physical performance in the multivariable analysis.
DlSCUSSlON
Muscle abnormalities have been identified in 13.0% to 40.0% of patients with liver cirrhosis, and recent reports have recognised their clinical significance[4-8]. However, there are limited data evaluating the loss of muscle quantity and quality in patients with CHB[7].
To the best of our knowledge, this is the first study to demonstrate that MAFLD and central obesity are associated with muscle abnormalities in the setting of CHB. Patients chronically infected with HBV with MAFLD had a 3.8-fold increased risk of muscle wasting compared to those without MAFLD. We also found that patients with central obesity had a threefold increased risk of muscle abnormalities in comparison with patients without central obesity.
In the current study, all CHB patients had quiescent virological activity. Although the long-term risk factors for cirrhosis and HCC, such as elevated levels of ALT and high HBV viral load, were not verified in our patients, 27.6% of them fulfilled the MAFLD criteria[14,21,52]. Thus, the presence of overweight,obesity or diet-related noncommunicable diseases should not be disregarded.
Concerning patients with cirrhosis, recent studies have shown that the presence of both obesity and muscle abnormalities was associated with higher rates of mortality than either condition alone[5,6].Myosteatosis, the infiltration of fat in skeletal muscle, has been associated with worse survival in cirrhotic patients compared to those with normal body composition[53]. In individuals with NAFLD,the presence of low muscle volume and high muscle fat has been associated with poor functional performance and metabolic comorbidities[53].
Conversely, investigations exploring muscle composition abnormalities in patients with CHB are scarce. Our findings are similar to those of a previous study reporting that the frequency of obesity was higher in CHB patients with muscle abnormalities than in those without this condition[7]. When the authors categorised the participants according to metabolic factors, a strong association between muscle abnormalities and advanced fibrosis was identified in patients with obesity, insulin resistance, metabolic syndrome and hepatic steatosis[7]. These data suggest that mechanisms associated with muscle abnormalities identified in patients with NAFLD/NASH could be found in patients chronically infected with HBV[8,53].
Regarding fatty liver disease, we must bear in mind the complexity of mechanisms implicated in skeletal muscle damage. Lee and colleagues identified that up to 12.0% of patients diagnosed with NAFLD had sarcopenia independent of obesity and insulin resistance, and approximately 30.0% of sarcopenic individuals without metabolic syndrome and obesity had NAFLD[54,55]. These results point to a bidirectional muscle-liver axis as a possible pathophysiological contributor to either nonhepatic- or hepatic-related complications. The mechanisms involved in muscle-liver crosstalk include insulin resistance, increased inflammation, myokines secreted by skeletal muscles, myostatin, adiponectin,vitamin D deficiency and physical inactivity[8]. Therefore, based on these facts, it remains of utmost importance to detect additional risk predictors, other than those related to HBV, for adverse liver and nonliver outcomes.
Given the relevance of metabolic derangement in the liver disease course, an expert panel proposed a new definition for metabolic dysfunction in the presence of liver disease, renaming NAFLD as MAFLD,which, unlike NAFLD, does not require the exclusion of other hepatic diseases[21]. Large longitudinal cohort investigations demonstrated that superimposed MAFLD, NAFLD and nonalcoholic steatohepatitis (NASH) in adults with CHB were associated with advanced fibrosis, necroinflammatory activity,liver-related complications and all-cause mortality[11-14].
Nevertheless, the impact of coexisting hepatic steatosis on HBV-related disease progression remains complex and controversial[20]. A recent investigation reported that although coexisting fatty liver was observed in approximately 34.0% of CHB patients receiving HBV antiviral therapy, hepatic steatosis was associated with a low risk of HCC[56].
In our study, low physical performance was associated with polypharmacy. Recently, Venter and colleagues[57] observed a significantly greater weight gain in patients with HIV treated with dolutegravir plus two prodrugs of tenofovir (tenofovir disoproxil fumarate and tenofovir alafenamide fumarate), especially in combination with TAF, than in participants who were treated with the standard-care regimen. Translating this evidence into the CHB context, it is important to mention that prodrugs of tenofovir have been extensively used worldwide as first-line options and long-term therapy for patients with chronic HBV infection[24]. The effects of nucleos(t)ide analogues on body composition in HBV-infected individuals have scarcely been investigated. However, previous studies have demonstrated fat body increases and mitochondrial alterations with long-term antiviral treatment[58,59].
Limitations of our study were the inclusion of patients attending a referral centre, which may have made them not be representative of all patients with CHB, and the cross-sectional nature of our investigation that precluded the possibility of recognising any cause-effect relationship between adverse skeletal muscle status and the coexisting fatty liver in patients with CHB. In addition, a detail of DXAderived measurements is their restraint in discerning any level of intramuscular fat infiltration.Furthermore, the inclusion of a control group of patients with MAFLD but without CHB should be assessed in a sequential investigation.
Although skeletal muscle abnormalities have been highly important in the course of chronic liver disease, there is no universal consensus to define and diagnose this condition in this population.Especially in patients with CHB, there is a need to endorse the definitions and cut-off values for assessing muscle mass (quantity/quality) and function. Regarding issues related to coexisting liver steatosis and myosteatosis[8,56], body composition assessment could shed light on the interplay among muscle, adipose tissue and liver in patients with CHB[7,8,53].
CONCLUSlON
In conclusion, MAFLD and central obesity were associated with muscle abnormalities in patients with CHB, independent of the stage of liver disease. These findings point to crosstalk between metabolic factors and skeletal muscle abnormalities in CHB. Both clinicians and researchers should emphasise the importance of holistic and integrated management of patients infected with HBV. The coexistence of CHB, muscle abnormalities, obesity, and metabolic dysregulation may be involved in the pathophysiology of nonhepatic- and hepatic-related outcomes. Thus, metabolic and skeletal muscle abnormality assessments should be encouraged among HBV-chronically infected individuals.
ARTlCLE HlGHLlGHTS
Research background
Recently, the clinical significance of sarcopenia in hepatic disease has been increasingly recognised.However, in chronic hepatitis B patients, the factors linked to skeletal muscle abnormalities have scarcely been investigated. Among them, host and environmental factors, such as nutritional and metabolic characteristics, should be evaluated.
Research motivation
Sarcopenia was identified in 7.1%, 11.8%, and 21.9% of noncirrhotic, compensated cirrhotic (Child-Turcotte-Pugh A), and decompensated cirrhotic (Child-Turcotte-Pugh B/C) patients, respectively. More recently, Han and colleagues observed that sarcopenia was significantly associated with liver disease severity, especially among hepatitis B virus (HBV)-positive subgroups with obesity, insulin resistance,metabolic syndrome and liver steatosis.
Research objectives
To investigate the association between components of sarcopenia and demographic, clinical, lifestyle,nutritional, and biochemical variables in HBV-chronically infected patients.
Research methods
Dual-energy X-ray absorptiometry (DXA) was used to assess muscle mass by quantifying appendicular lean mass (ALM) adjusted for body mass index (ALMBMI). Muscle function was evaluated by hand grip strength (HGS) and the timed up and go test. Metabolic-associated fatty liver disease (MAFLD) was defined according to the criteria proposed by an international expert panel. A Body Shape Index and the International Physical Activity Questionnaire were used to assess central obesity and physical activity level, respectively.
Research results
This cross-sectional study included 105 chronic hepatitis B (CHB) outpatients followed at the tertiary care ambulatory centre (mean age, 48.5 ± 12.0 years; 58.1% males; 76.2% without cirrhosis; 23.8% with compensated cirrhosis). The DXA-derived fat mass percentage was inversely correlated with the ALMBMI(r= - 0.87) and HGS (r= - 0.63). In the multivariable analysis, MAFLD, sedentarism and central obesity were positively and independently associated with low ALMBMI. Central obesity was independently associated with low HGS. MAFLD and central obesity were independently associated with low HGS.
Research conclusions
Among patients with CHB, metabolic-associated fatty liver disease (MAFLD) and central obesity were associated with low muscle mass and strength. Metabolic and skeletal muscle abnormality appraisal should be encouraged among HBV-chronically infected individuals.
Research perspectives
Further large-scale case-control studies are needed to evaluate the role of MAFLD in HBV-chronically infected patients, including individuals with MAFLD but without CHB.
ACKNOWLEDGEMENTS
The authors appreciate all participants for their contribution to this study and the Outpatient Clinic of Viral Hepatitis staff of the Instituto Alfa de Gastroenterologia, Faculdade de Medicina, Universidade Federal de Minas Gerais.
FOOTNOTES
Author contributions:All authors have made substantial contributions; Santos CML, Rocha GA, Silva LD, and Bering T designed the research (project conception, development of overall research plan, and study oversight); Santos CML, Malheiro OB, Brito MD, Castro PASV, Vries TP, Viana NL, Coelho MPP, and Cambraia RD conducted the research (data collection); Malheiro OB, Teixeira R, and Gonzalez MC provided essential materials for the research;Santos CML, Malheiro OB, Brito MD, Castro PASV, Vries TP, Viana NL, Coelho MPP, Cambraia RD, and Silva LD analysed the data or performed the statistical analysis; Santos CML, Rocha GA, and Silva LD wrote the paper; and Santos CML, Rocha GA, and Silva LD had primary responsibility for the final content; all authors critically revised the manuscript, agree to be fully accountable for ensuring the integrity and accuracy of the work, and read and approved the final manuscript.
Supported bythe Fundação de Amparo à Pesquisa do Estado de Minas Gerais, No. APQ - 02320 - 18.
lnstitutional review board statement:The study was designed and conducted following the Declaration of Helsinki and was approved by the Ethics Committee of Federal University of Minas Gerais/UFMG (ETIC 0404.0.203.000 - 10;CAAE, 07761212.2.0000.5149).
lnformed consent statement:All study participants, or their legal guardian, provided informed written consent prior to study enrollment.
Conflict-of-interest statement:All authors report no conflict of interest.
Data sharing statement:No additional data are available.
STROBE statement:All authors have read the STROBE Statement checklist of items, and the manuscript was prepared and revised according to the STROBE Statement checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Brazil
ORClD number:Cecy Maria de Lima Santos 0000-0003-4452-4298; Matheus Duarte Brito 0000-0002-1296-6705; Pedro Alves Soares Vaz de Castro 0000-0002-1183-7610; Thais Pontello de Vries 0000-0002-0572-5911; Nataly Lopes Viana 0000-0002-2175-4034; Marta Paula Pereira Coelho 0000-0003-2074-8959; Olívio Brito Malheiro 0000-0001-8149-5698; Tatiana Bering 0000-0002-5288-6216; Rosângela Teixeira 0000-0003-2192-722X; Rodrigo Dias Cambraia 0000-0002-1481-3294; Gifone Aguiar Rocha 0000-0002-1858-3166; Luciana Diniz Silva 0000-0003-0061-7361.
S-Editor:Wang LL
L-Editor:A
P-Editor:Cai YX
杂志排行
World Journal of Hepatology的其它文章
- Long-term liver allograft fibrosis: A review with emphasis on idiopathic post-transplant hepatitis and chronic antibody mediated rejection
- Outcomes of patients with post-hepatectomy hypophosphatemia: A narrative review
- Simple diagnostic algorithm identifying at-risk nonalcoholic fatty liver disease patients needing specialty referral within the United States
- Higher cardiovascular risk scores and liver fibrosis risk estimated by biomarkers in patients with metabolic-dysfunction-associated fatty liver disease
- Prevalence of sarcopenia using different methods in patients with non-alcoholic fatty liver disease
- Effect of probiotics on hemodynamic changes and complications associated with cirrhosis: A pilot randomized controlled trial