Patient experience of residents with restricted primary care access during the COVID- 19 pandemic
2022-07-26TakuyaAokiYasukiFujinumaMasatoMatsushima
Takuya Aoki , Yasuki Fujinuma, Masato Matsushima
ABSTRACT
INTRODUCTION
In a context where the COVID— 19 pandemic has placed a tremendous burden on health—care systems around the world, primary care capabilities play pivotal roles. Primary care providers aid in the triage and treatment process, help educate patients and render preventive care including vaccination. To bypass physical contact and allow vulner—able patients to have access to primary care from the safety of their homes, some primary care providers leverage telemedicine.1In Western countries and Japan, most patients with COVID— 19 are seen first by primary care providers because the majority of infected individuals experience only mild to moderate symptoms.2
In Japan, as in other countries, the primary care sector has performed the initial assess—ment, including testing for COVID— 19, and triaged patients to determine those in need of hospitalisation.3The government has noti—fied the public that they should first visit their primary care physician (usual source of care(USC)) if they have symptoms suspected of COVID— 19, such as fever.4Japanese primary care services are generally provided in both community clinics and outpatient depart—ments of small— sized and medium— sized hospi—tals that are predominantly privately owned and managed.5The Ministry of Health,Labour and Welfare has recommended that all individuals should have a USC volun—tarily6and former surveys have reported that approximately half of the Japanese adult resi—dents had a USC.78However, patient regis—tration with primary care physicians has not been institutionalised.
During the pandemic, several countries reported that medical facilities have refused to provide care for patients with suspected or confirmed COVID— 19 infection.9This means that not only residents who do not have a USC but also those who have a USC may have restrictions in accessing COVID— 19 care. In Japan, some medical insti—tutions, including primary care facilities, have been rejecting possible COVID— 19 patients; therefore, Japan’s national and city governments are upping the pressure on medical institutions to take in COVID— 19 patients.1011The refusal may be due to concerns about cluster outbreaks within medical institutions and lack of staff, space for consultation and equipment to deal with the infections.However, it has not been qualified how much residents’access to COVID— 19 consultation is restricted owing to their primary care providers’ refusal to see patients with suspected COVID— 19. Furthermore, whether restricted primary care access during the pandemic is associated with patient experience has not previously been investi—gated. Patient experience is the core quality measure of patient— centredness, which is globally deemed to be one of the core aims of a healthcare system.1213
Therefore, in this study, we aimed to evaluate primary care access for COVID— 19 consultation among residents who have a USC and to examine their associations with patient experience during the pandemic in Japan.
METHODS Design, setting and participants
The data for this study were sourced from the National Usual source of Care Survey (NUCS), which was conducted in May 2021 during the COVID— 19 fourth wave in Japan.The NUCS was a nationwide mail survey that collected data on the USC, patient experience of primary care,healthcare utilisation, health conditions, health— related quality of life and sociodemographic characteristics of a representative sample of the Japanese adult population.7One of the primary research objectives of the NUCS was to evaluate primary care access for COVID— 19 consulta—tion among residents who have a USC and to examine their associations with patient experience. In the NUCS,a nationally representative panel in Japan, which was administered by the Nippon Research Center, was used to select potential participants. This panel comprised approximately 70 000 residents who were selected using a multistage sampling method and participated in a previous survey of the Nippon Research Center.14From the panel, 2000 potential participants aged 20—75 years were selected using stratified sampling by age, sex and residential area. The survey participants received ¥500 gift certificates.
Among adult residents who responded to the NUCS,eligible participants in this study were individuals who had a USC. To identify an individual’s USC, the following items were used in the Primary Care Assess—ment Tool (PCAT)15and the Medical Expenditure Panel Survey16: ‘Is there a doctor that you usually go to if you are sick or need advice on your health?’ A participant was considered to have a USC if they were able to iden—tify a physician who practices outside university hospi—tals. According to a previous national survey conducted by the Japan Medical Association in 2020, the propor—tion of Japanese adults who have a USC was 55.2%.8The eligible participants in this study, who have a USC, were considered to be highly representative because we used the resident panel selected by a probability sampling method.
Measures
Patient experience of primary care
The outcome measure in this study was patient experi—ence of primary care assessed by the Japanese version of Primary Care Assessment Tool Short Form (JPCAT— SF).17The JPCAT— SF is based on the PCAT,15which was devel—oped by the Johns Hopkins Primary Care Policy Center.This tool is a Japanese version of the PCAT and not a simple Japanese translation of the PCAT. It consists of fewer items than the original version for better usability.A previous study showed that the JPCAT— SF has good reliability and validity.17This 13— item tool comprises six multi— item domains addressing the following primary care attributes: first contact, longitudinality, coordination,comprehensiveness (services available), comprehensive—ness (services provided) and community orientation.15The JPCAT— SF scoring system is structured as follows: each response on a 5— point Likert scale (1=strongly disagree,2=somewhat disagree, 3=not sure, 4=somewhat agree and 5=strongly agree) is converted into an item score between 0 and 4. The calculated means of item scores in the same domain were multiplied by 25 to yield domain scores ranging from 0 to 100 points. The JPCAT— SF total score is the mean of the six domain scores and reflects an overall measure of primary care experience, with higher scores indicating better patient experience.
Primary care access for COVID-19 consultation
In this study, primary care access for COVID— 19 consul—tation was assessed from the patient’s perspective.Restricted primary care access for COVID— 19 consultation was defined as impaired access to an individual’s USC when COVID— 19 was suspected owing to fever during the outbreak. Survey respondents were asked about service availability in their USC using a standardised question‘Please respond to the situation after the outbreak of the new coronavirus. When you have a fever, would someone from your primary care physician’s facility see you?’ Participants were asked to rate this question on a 4— point scale (1=definitely, 2=probably, 3=probably not and 4=definitely not). We developed this question by modifying the items in the first contact domain of the PCAT and reviewing its face validity. Participants were identified as having restricted primary care access if they responded ‘definitely not’ or ‘probably not’ to this question.
Confounding factors
The potential confounding factors were selected on the basis of previous studies that suggested confounding relationships between primary care access and patient experience.518—20We assessed the following factors by using a self— administered questionnaire: age, sex, years of education, annual household income, number of chronic conditions, primary care physician location (clinic,hospital, other) and health— related quality of life assessed by the five— level version of the EuroQol five— dimensional questionnaire.21We used a validated list of 20 chronic conditions that were created based on previous multi—morbidity literature and their relevance to the primary care population22: hypertension, depression/anxiety,chronic musculoskeletal conditions causing pain or limitation, arthritis/rheumatoid arthritis, osteoporosis,chronic respiratory disease (asthma, chronic obstructive pulmonary disease or chronic bronchitis), cardiovas—cular disease, heart failure, stroke/transient ischaemic attack, stomach problem, colon problem, chronic hepa—titis, diabetes, thyroid disorder any cancer in the previous 5 years, kidney disease/failure, chronic urinary problem,dementia/Alzheimer’s disease, hyperlipidaemia and obesity.
Statistical analysis
Descriptive statistics were obtained for the participants’characteristics and the JPCAT— SF scores. To examine the association between primary care access for COVID— 19 consultation and patient experience assessed by the JPCAT— SF total score, we used multivariable linear regression analyses adjusting for confounding factors.In addition, we also performed exploratory analyses to investigate the associations between primary care access and each domain score of the JPCAT— SF using the same models. According to previous studies, a difference of >3—point in patient experience measures linearly scaled to a 0—100 range was considered significant in magnitude with regard to practical importance.52324
For each analysis, we used a two— sided significance level of p=0.05. Missing data for independent and dependent variables were adjusted by applying multiple imputations,with 20 imputations, using a fully conditional specifica—tion. Statistical analyses were conducted using R, V.4.1.0(R Foundation for Statistical Computing, Vienna, Austria;www.R—project.org).
RESULTS Participants’ characteristics
A total of 1757 individuals out of 2000 adult residents responded to the NUCS (response rate: 87.9%). Among them, we excluded 746 respondents who did not have a USC and seven respondents who did not respond to the survey item regarding access to COVID— 19 consultation.We performed analyses of the remaining 1004 eligible participants. Table 1 shows the characteristics of the eligible participants, with or without restricted primarycare access for COVID— 19 consultation. Among the eligible participants, 198 (19.7%) reported restricted primary care access for COVID— 19 consultation despite having a USC. Compared with participants without restricted primary care access, those with restricted primary care access had more chronic conditions (≥2 chronic condi—tions, 37.4% vs 33.5%).
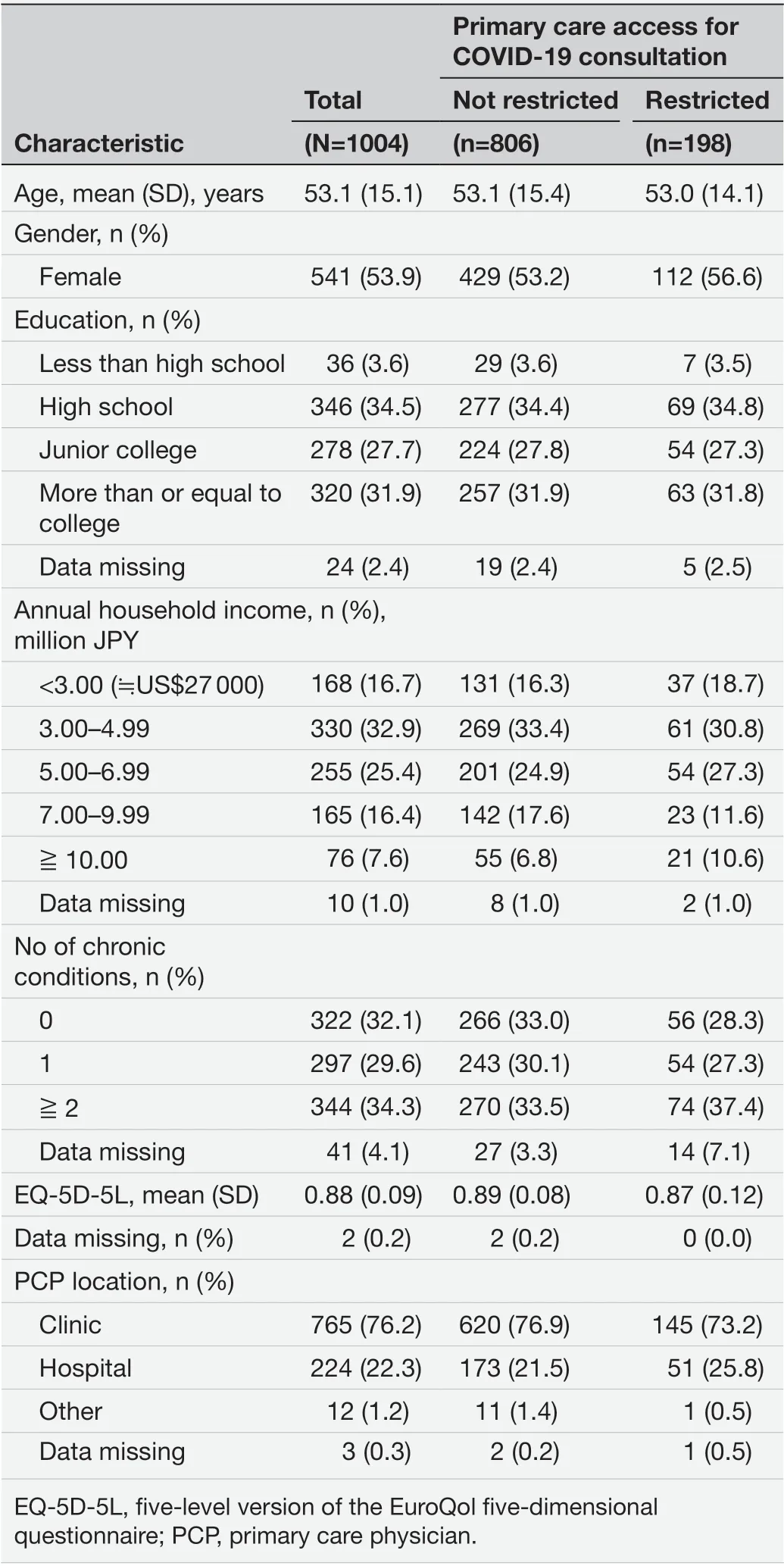
Table 1 Participants' characteristics
Primary care access for COVID-19 consultation and patient experience
Table 2 shows the distribution of JPCAT— SF scores. The average JPCAT— SF total score was 45.9 out of 100 points;the most highly scored domain was longitudinality(54.4), and the most poorly scored domain was firstcontact (32.9). Table 2 also compares the distribution of JPCAT— SF scores with or without restricted primary care access for COVID— 19 consultation. The participants with restricted primary care access had lower total scores and all domain scores compared with participants without restricted access.
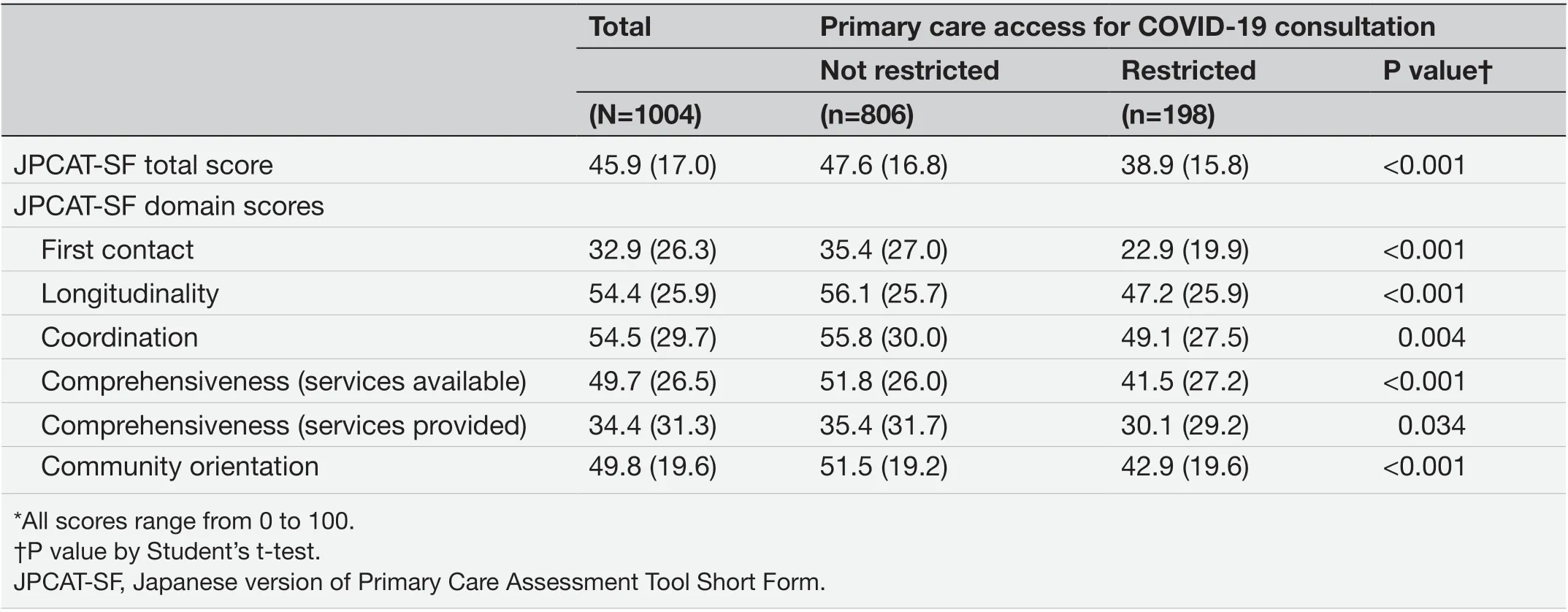
Table 2 Distribution of JPCAT- SF scores: mean (SD)
Table 3 shows the results of the linear regression anal—yses, examining the association between primary care access to COVID— 19 consultation and JPCAT— SF scores as measures of patient experience. After adjustment for possible confounders, restricted primary care access for COVID— 19 consultation was negatively associated with the JPCAT— SF total score (adjusted mean difference = −8.61,95% CI −11.11 to −6.10). In addition, restricted primary care access was significantly associated with a decrease in all JPCAT— SF domain scores. First contact had the strongest association with restricted primary care access for COVID— 19 consultation (adjusted mean difference =−12.26, 95% CI −16.02 to −8.50).
DISCUSSION This nationwide study in Japan revealed that approx—imately one— fifth of adult residents who had a USC reported restricted primary care access for COVID— 19 consultation owing to their primary care providers’refusal during the pandemic. Our study also found that restricted primary care access for COVID— 19 consul—tation was negatively associated with a wide range of patient experience assessed by the JPCAT— SF. Refusal of COVIID— 19 care by primary care providers was negatively associated with not only first contact, which is an attri—bute related to accessibility, but also with other attributesincluding longitudinality, coordination, comprehensive—ness and community orientation.
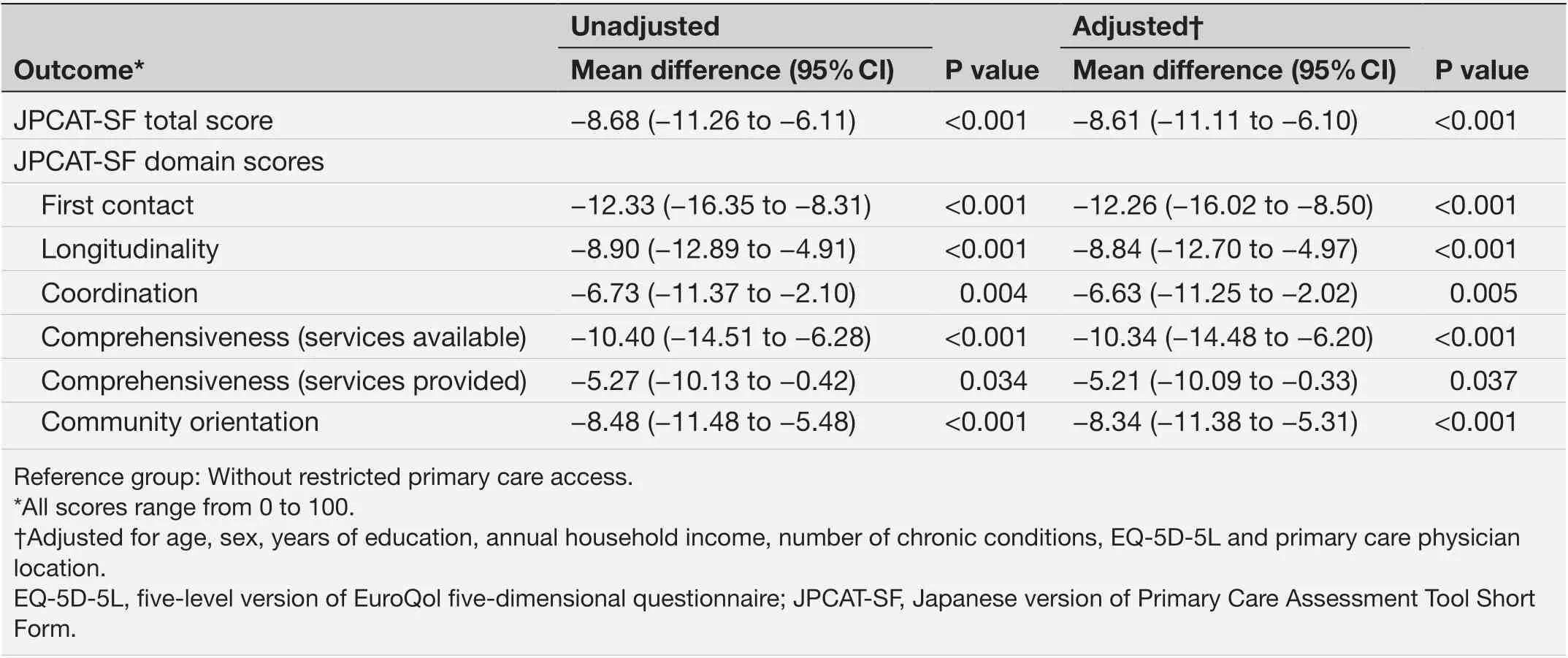
Table 3 Association between primary care access for COVID- 19 consultation and patient experience (n=1004)
Although there have been domestic and international news reports on the refusal of patients with suspected or confirmed COVID— 19 in primary care facilities, few studies have presented specific data. In a previous simu—lated patient study in primary care facilities in the USA,20% of participating facilities guided patients with suspected COVID— 19 to consultation in an emergency department or COVID— 19 hotline.25Such a provider’s response to COVID— 19 may have a broad impact on the residents’ experience because COVID— 19 is a health issue of great concern to residents. Since primary care attri—butes such as first contact, longitudinality, coordination,comprehensiveness and community orientation play an important role in COVID— 19 care,26the refusal of patients with suspected COVID— 19 may have led to residents’ eval—uation of their primary care provider as lacking in these characteristics. This overall poor primary care experience may lead to poor adherence to treatment of both commu—nicable and noncommunicable diseases, preventive care and inefficient patient behaviours such as bypassing a USC to seek care at higher— level healthcare facilities.27—30
Our study indicated that timely access to primary care during a pandemic may be a critical issue in improving patient experience. Refusal of COVID— 19 patients is not only an issue at the level of medical providers and facilities,but also at the healthcare system. For primary care facil—ities to respond to the pandemic, they need support from the government and outside medical institutions, such as education on infectious disease care and control, supplying necessary supplies and financial support. As a health policy issue in Japan, the application and spread of telemedicine have been slow even during the pandemic.31Therefore, it is necessary to improve access to care by telemedicine expan—sion while considering the quality, safety and equity of care,especially for vulnerable people who have multimorbidity. In addition, the free access system and the lack of patient regis—tration with primary care providers may lead some primary care providers not to responsibly manage the health of indi—vidual residents, including when COVID— 19 is suspected.
To the best of our knowledge, this is the first study to report residents’ primary care access for COVID— 19 consul—tation and examine their associations with patient experi—ence in Japan. A key strength of our study is the use of data from a nationwide study, with a sample representative of the Japanese adult population, which allows for generalisation of its results to the wider population. Another strength is the high study response rate compared with other national surveys. The PCAT is a validated and internationally estab—lished tool for evaluating patient experience of primary care attributes.
Our study also has several potential limitations. First, our assessment of primary care access was based on residents’perspectives and not on objective data from providers.However, subjective assessment of accessibility is also crucial because it directly relates to healthcare utilisation of resi—dents.32Second, we collected information on access to consultation when limited to fever, a typical symptom of COVID— 19, but not for other symptoms and conditions already confirmed as COVID— 19. Third, given that the data were cross— sectional, a causal relationship between restricted primary care access and patient experience can definitively not be established. Fourth, this study was conducted in Japan, which does not have a patient regis—tration system for primary care providers, and this should be considered when generalising the results of this study to other countries.
CONCLUSIONS
Approximately one— fifth of adult residents who had a USC reported restricted primary care access for COVID— 19 consultation during the pandemic in Japan. Our study also found that restricted primary care access for COVID— 19 consultation was negatively associated with a wide range of patient experience including first contact. Material, finan—cial and educational support to primary care facilities, the spread of telemedicine, and the application of a patient registration system might be necessary to improve access to primary care during a pandemic.
ContributorsAll authors (TA, YF and MM) of the paper contributed the conception or design of the work. TA performed the statistical analyses. TA, YF and MM interpreted the analyses. TA drafted the manuscript. All authors reviewed and edited the manuscript, contributed to the discussion of the data and performed critical review of the manuscript. All authors gave the final approval of the manuscript before submission. TA is the guarantor of the work and accepts full responsibility for the presented content.
FundingThis work was supported by JSPS KAKENHI Grant Number JP20K18849.
Competing interestsTA reports grants from JSPS KAKENHI, during the conduct of the study; and TA received lecture fees and lecture travel fees from the Centre for Family Medicine Development of Japanese Health and Welfare Co- operative Federation. MM received lecture fees and lecture travel fees from the Centre for Family Medicine Development of Japanese Health and Welfare Co- operative Federation. MM’s son- in- law worked at IQVIA Services Japan K.K. which is a contract research organisation and a contract sales organisation. MM’s son- in- law works at SYNEOS HEALTH CLINICAL K.K. which is a contract research organisation and a contract sales organisation.
Patient consent for publicationConsent obtained directly from patient(s).
Ethics approvalThe institutional review board of the Jikei University School of Medicine approved this study (approval no. 32- 416(10505)). Participants gave informed consent to participate in the study before taking part.
Provenance and peer reviewNot commissioned; externally peer reviewed.
Data availability statementNo data are available. Due to the nature of this research, participants of this study did not agree for their data to be shared publicly,so supporting data are not available.
Open accessThis is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially,and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
ORCID iD
Takuya Aoki http://orcid.org/0000-0002-8232-2155
杂志排行

Family Medicine and Community Health的其它文章
- Development and validation of the scale for measuring biopsychosocial approach of family physicians to their patients
- Acceptability of a task sharing and shifting model between family physicians and physiotherapists in French multidisciplinary primary healthcare centres: a cross- sectional survey
- Transitions in health service use among women with poor mental health: a 7- year follow- up
- Putting health workers at the centre of health system investments in COVID- 19 and beyond
- COVID- 19 vaccine hesitancy and related factors among primary healthcare workers in a district of Istanbul: a crosssectional study from Turkey
- Side effects and acceptability measures for thermal ablation as a treatment for cervical precancer in low- income and middle- income countries: a systematic review and meta- synthesis