Side effects and acceptability measures for thermal ablation as a treatment for cervical precancer in low- income and middle- income countries: a systematic review and meta- synthesis
2022-07-26EvelyneMariePiretBethPayneLaurieSmithJessicaTrawinJacksonOremGinaOgilvieCarolynNakisige
Evelyne Marie Piret , Beth A Payne, Laurie W Smith, Jessica Trawin, Jackson Orem, Gina Ogilvie, Carolyn Nakisige
ABSTRACT
I NTRODUCTION
Cervical cancer disproportionately affects women in low— income and middle— income countries (LMICs). Of the 311 000 total global cervical cancer deaths in 2018, nearly 90%were reported in LMICs, with this burden of disease expected to increase without mean—ingful intervention.1These disparities are largely due to differing levels of accessibility to effective prevention, screening and treat—ment strategies. For example, over 80% of high— income countries have an established cervical cancer screening programme while less than 50% of LMICs do, achieving average screening coverages of 63% and 19%,respectively.2What makes these low rates of coverage in LMICs so troubling is that cervical cancer is an almost entirely prevent—able disease. Practically all cases are caused by human papillomavirus (HPV) types for which an effective vaccine exists.3Furthermore, the disease’s extended natural progression from persistent HPV infection to precancerous cervical lesions, defined as ranging from low to high grade cervical intraepithelial neoplasia (CIN1—3), occurs over the course of years. Where relevant treatment modalities are accessible, early detection and remedia—tion are thus possible within a relatively large window of time prior to the development of invasive cancer.
To address this global health inequity, in November 2020, the WHO announced its goal to eliminate cervical cancer as a public health problem by the end of the century.1They have set 90—70—90 targets to be met by every country by 2030. These targets include having 90% of girls vaccinated with the HPV vaccine, 70% of women screened at least twice in their lifetime and 90% of women receiving treatment when precancerous or cancerous cervical lesions are detected through screening.1Given the limited progress of HPV vaccination campaigns in LMICs and current generations already exposed to HPV,effective screening and treatment programmes are essen—tial to reduce global incidence of cervical cancer and related mortality.
To effectively meet the screening and treatment targets,the WHO recommends a screen— and— treat approach for LMICs.4The screen— and— treat approach involves screening women for CIN without histological confir—mation followed by rapid treatment when results suggest the presence of precancerous lesions, preferably within the same visit. Screening for high— risk HPV types is the preferred method as resources permit, with visual inspec—tion with acetic acid (VIA) and/or visual inspection with Lugol’s iodine (VILI) available as alternative or confir—matory screening methods to HPV testing.4Referrals are given to women who require treatment for invasive cervical cancer.
Following positive screening test results, precancerous lesions can be removed by excision or destroyed by abla—tion in outpatient clinics. Given the resource requirements of excisional treatment methods, the WHO recommends that ablative techniques be prioritised for eligible patients when available.5The two primary ablative techniques recommended are cryotherapy and TA. Cryotherapy is an ablative technique that destroys tissue by freezing it using nitrous oxide or carbon dioxide gas. These gas— based units have been associated with inefficiencies in LMICs due to the continuous costs, procurement challenges and transportation issues of the gas tanks.6TA, also known as thermocoagulation and cold coagulation, is an ablative technique with comparable efficacy to cryotherapy that destroys tissue by heating it.78As with cryotherapy, it can be performed by a variety of medical providers and does not require anaesthesia. TA is relatively portable given its light weight and can be battery powered, enabling greater reliability in low— resource settings. As it does not use disposable parts or gas tanks, this method does not require continuous costs beyond maintenance, making it more feasible across healthcare settings, including community care and rural contexts.6
In 2019, TA was endorsed by the WHO guidelines for the treatment of precancerous lesions in LMICs based on early evidence of safety and efficacy, and its simplicity of use in screen— and— treat strategies. Yet, questions remain about the potential harms of overtreatment. Screen—and— treat programmes that use high— risk HPV tests (95%sensitivity and 84% specificity) and/or VIA tests (60%sensitivity and 84% specificity) result in overtreatment when all screened positive women are treated.5Over—treatment is defined as the percentage of women treated despite having no true lesions or lesions graded as CIN1,given that a large proportion of the latter would resolve without treatment. Reported rates of overtreatment from LMICs ranged from 30% to 69%.9—12The high poten—tial for overtreatment highlights the need to consider treatment side effects and patient acceptability alongside efficacy and logistical concerns when weighing the risks and benefits of different treatment options within screen—and— treat strategies.
This systematic review and meta— synthesis summarises rates of side effects and patient acceptability measures among women in LMICs receiving TA to treat suspected or confirmed precancerous lesions following cervical cancer screening.
METHODS Protocol and registration
This systematic review was registered on PROSPERO in August 2020 as PROSPERO 2020 CRD42020197605. The full protocol is accessible at https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020197605.
Search strategy and selection criteria
A search strategy was developed to identify papers that report on the use of TA for treatment of actual or suspected (HPV+) precancerous lesions on the cervix. A wide range of keywords were used to capture both cate—gories (online supplemental material; p1). To avoid over restricting our search, the search strategy did not include terms related to side effects or LMICs. The search was restricted to papers written in English.
The search strategy was adapted using the Polyglot Search Translator and executed in Ovid MEDLINE(1946—2020), EMBASE (1947—2020), CINAHL and CAB Global Health from database inception to 29 July 2020.13On 18 December 2020, the search strategy was rerun in the original four databases to capture any newly published research. At this time, additional searches were conducted in regional databases to access a greater number of papers from LMICs, specifically: Africa— Wide Information (AIM,1964—2020) and IMEMR, ISMEAR, LILACS, WPRIM and GHL through the WHO’s Global Index Medicus. As a final step, reference lists from relevant literature were reviewed to supplement the search strategy. Papers were uploaded to Covidence for review after duplicates were removed in EndNote (online supplemental figure S1).14
Research papers were included in this review if they met the following criteria: (1) participants were women living in an LMIC according to the World Bank GNI 2020,15(2) participants had completed a cervical cancer screening test to identify them as being at high risk of cervical precancer, with or without additional triage or histopathological diagnosis of cervical neoplasm, (3)the intervention used for treatment of the cervix was a recognised device for TA and (4) the study reported side effects of treatment (such as pain, bleeding, vaginal discharge or other) or quantitative measures of accept—ability (such as satisfaction, willingness to recommend treatment to others and patient experience). Papers with any mention of side effects or acceptability measures were included regardless of the use of standard definitions.For the purpose of this review, when referring to women participants, this includes every person who has a cervix.Papers that presented case studies, lacked original data or were written in a language other than English were excluded. The involvement of patients or the public was not appropriate in the design, conduct, reporting and dissemination of our research.
Study selection
To identify studies for inclusion, articles were assessed through two— stage review processes by BP and EMP.An initial title and abstract review was independently performed by both reviewers to screen papers for use of TA following a positive screening test indicating risk or confirmation of precancerous cervical lesions. For this initial stage, all conflicts regarding decision to include were managed through discussion between the two inde—pendent reviewers. Full text articles were then gathered from the original database source, or when full text was not found, corresponding authors were contacted to request manuscript copies. Articles underwent full text review by BP and EMP. Articles were included if they reported any side effects or measures of acceptability following TA and were conducted in LMICs. Any conflict in decision to include at this stage was managed through discussion between the two independent reviewers and with a third reviewer when required (GO).
Data extraction
Data were extracted by one reviewer into a study— specific spreadsheet. Summary data were taken from included studies for all primary outcomes, including side effects,willingness to recommend treatment to others, patient satisfaction and patient experience. Where rates were not provided or only aggregate side effects listed, authors were contacted to request individual participant data.Data extracted from the articles included the authors,year of publication, title, country where screening was conducted, study period, study design, sample char—acteristics, number of participants who received treat—ment, screening method, treatment method, treatment setting, treatment provider type, participants’ age, time to follow— up, assessment of side effects, side effects/adverse effects reported and reports of acceptability, as well as the study definition of side effects or acceptability measures reported and the way in which these outcomes were measured.
Risk of bias assessment
Full articles were individually evaluated for quality and risk of bias by BP and EMP using the assessment criteria devel—oped by Downs and Black.16The final assessment criteria on the risk of bias tool related to sample size and power was modified to a yes/no response to reflect the multiple study types included. This criterion was considered met when a study included justification for the sample size that indicated adequate power was achieved to meet the primary study endpoint. Both authors independently reviewed all included full text papers, with consensus on final rankings made through discussion.
Statistical analysis
Individual study side effect rates were summarised and 95% CIs calculated for each study using the Wilson score method. Pooled rates of side effects were calculated as proportions using the metaprop package in STATA(https://archpublichealth.biomedcentral.com/articles/10.1186/2049—3258—72—39). This method of synthesis esti—mates pooled proportions using a random effects model with binomial distribution, including the Freeman— Tukey double arcsine transformation to stabilise variances when estimates are close to 0 or 1. Study heterogeneity was estimated by calculating the I2. All studies with numeri—cally reported side effects were included in the analysis.Subgroup analysis was planned for place of treatment(facility or community; rural or urban setting), provider type (physician or nurse/midwife) and time to side effect assessment grouped as within 4 weeks of treatment or at >4 weeks after treatment. All analyses were performed using STATA V.15.0.17
RESULTS Study selection
A total of 1754 titles were identified through the data—base search on 29 June 2020. After removing duplicates,1336 were uploaded to Covidence for abstract and title screening. Two independent reviewers identified 64 papers for full text evaluation of which 12 were found to meet all inclusion criteria for this review.9—1118—26Of note,30 papers were identified as abstracts from conference proceedings with no full text available at that time. All authors of these abstracts were contacted to solicit infor—mation on final publication. Several authors reported manuscripts were under review and expected before the end of the year. As a result, a repeat of the database search was conducted on 18 December 2020, in addi—tion to the regional databases. This added a further 254 titles for abstract and title screening, and final inclusion of three more full papers.122728Two papers reported on overlapping study populations.1227The paper reporting on the largest study population was included in the meta— synthesis.12A subset of four studies that provided narrative results alone for a composite measure of all side effects were excluded from meta— synthesis due to concerns around reporting bias.23—26Study inclusion and reasons for exclusion at full text review are provided in the Preferred Reporting Items for Systematic Reviews and Meta— Analyses diagram (online supplemental figure S1).
Study characteristics
There were 2709 participants in the 15 papers included in the narrative portion of this review. The meta— synthesis includes information on side effects or measures of treat—ment acceptability for 2039 individual women across 10 studies. The studies included were conducted in Africa(seven studies); South— Eastern Asia (three studies); the Americas (two studies); and the Western Pacific region(three studies) (table 1). The number of participants receiving TA in included studies ranged from 5 women to 511 women (table 2). Significant heterogeneity across these studies’ inclusion criteria, specifically age range for cervical cancer screening enrolment, is noted in table 1. Included studies also varied in screening method and eligibility protocol used for TA. Screening models used a variety of combinations of methods for eligibility screening, including HPV testing (eight studies), VIA(seven studies), VILI (one studies) and cytology (one study) (table 1). Additional triage was performed using colposcopy or cervical cytology in five studies, and two studies based treatment decision on colposcopy results alone (table 1).
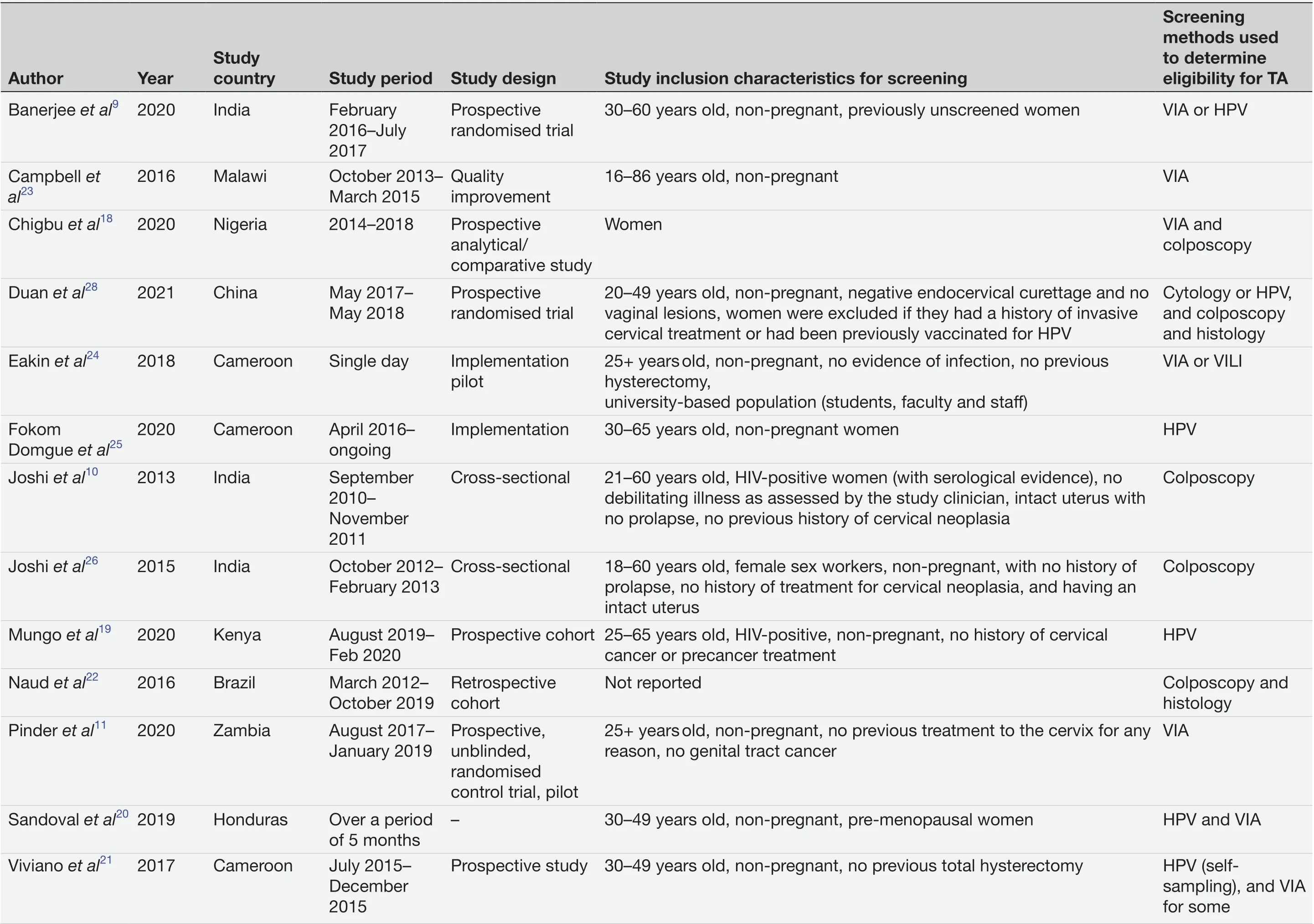
Table 1 Study characteristics and screening methods used to select candidates for TA

Table 1 Continued
Treatment sample size, method, place, provider and timing also varied between studies (table 2). The most common treatment application was performed using a probe heated to 100°C for 45 s with multiple applica—tions as needed to ensure adequate coverage of the trans—formation zone (TZ) (table 2). In all included papers,women were only eligible for treatment with TA after a positive screening test if the entire lesion was visible on the ectocervix, the squamocolumnar junction was visible,the lesion involved three quadrants or less of the TZ and there was no suspicion of glandular disease or invasive cancer, in accordance with the WHO guidance.4
Risk of bias
The risk of bias for included studies was moderate to high with a mean score on the Downs and Black’s checklist of 18.2 (±3.0) out of 27 possible points.16This checklist is broken down into sections related to quality of reporting,internal validity, confounding and selection bias, external validity and power. Areas of concern for each study are colour coded and presented in table 3. Quality of reporting was high, but issues of internal validity, confounding and selection bias and power were found in most studies.
Results from individual studies and meta-synthesis
The proportion of women with side effects is reported by 10 of the 15 included studies (online supplemental table S1). Studies included side effects that occurred both during treatment and post treatment, as ascertained during a follow— up study visit. The timing of follow— up visits ranged from 2 weeks to 12 months post treatment with the majority reporting at 1 month (table 2). The proportion of women reporting a composite of any one or more side effect at the time of treatment was 46%(95% CI 35% to 58%; I2=92.06%) (4 studies; n=1021)(figure 1A). No studies reported a composite rate of side effects post treatment.
Pain
Pain during or immediately after treatment was reported by eight studies using a variety of methods, including Visual Analogue Scales, pictorial aides and simple yes/nosurvey questions (online supplemental table S1). In four studies, pain was defined as abdominal pain, cramping and/or discomfort,9—1121while the remaining defined pain as abdominal pain alone.12192028No study reported provision of analgesia of any sort prior to treatment. The overall rate of reported pain at or immediately after treat—ment was 70% (95% CI 52% to 85%; I2=98.01%) (8 studies;n=1454) (figure 1B). Of the eight studies that report pain at treatment, a subset differentiated pain into categories of mild (70%, 95% CI 55% to 83%; I2=96.71%) (7 studies;n=1330), moderate (11%, 95% CI 3% to 22%; I2=96.49%)(5 studies; n=1108) and severe (2%, 95% CI 1% to 4%;I2=67.00%) (6 studies; n=1278) (figure 1C—E). Propor—tions of women reporting pain did not differ significantly based on study setting overall, but moderate pain and severe pain were more commonly reported when treat—ment occurred in a facility compared with community clinics (figure 1B,D,E). Two studies reported pain rated on a Visual Analogue Scale with means of 3.0/10.0.2128

Table 2 TA treatment methods and details for included studies
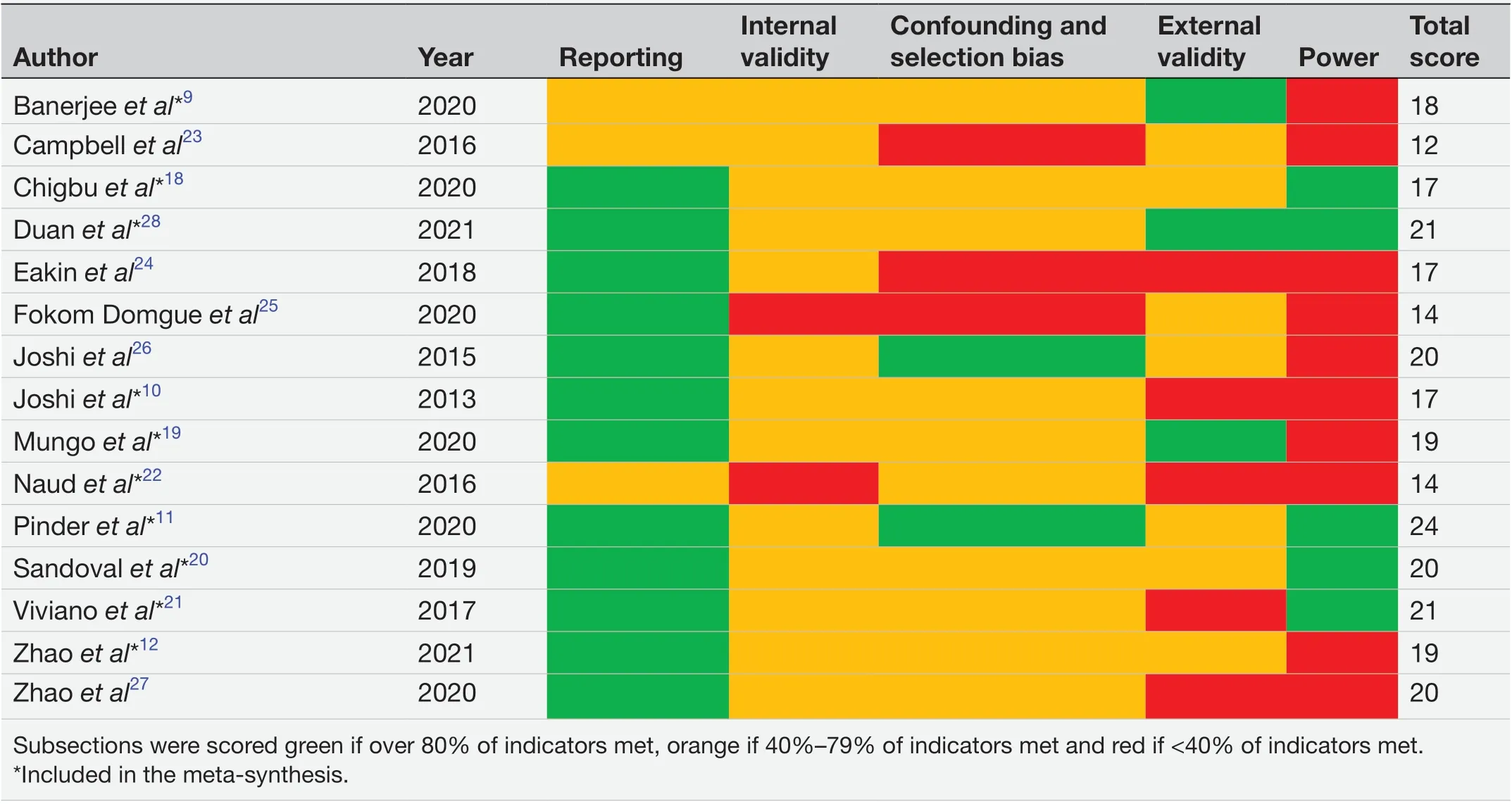
Table 3 Risk of bias assessment based on Downs and Black’s criteria16
Post— treatment pain at follow— up was less common,being reported by 8% (95% CI 3% to 14%; I2=94.06%)of women (7 studies, n=1777) (figure 2A) with a mean duration ranging from 2 days to 7 days (3 studies) (online supplemental table S1). Less pain was reported in studies with longer follow— up times (figure 2A).
Bleeding
Bleeding during or immediately after treatment was rare and occurred in 2% (95% CI 0% to 5%; I2=86.77%)of women and did not differ significantly by treat—ment setting (7 studies; n=1386) (figure 1F). Overall,as reported by women at follow— up, ongoing bleeding after treatment was much more common and occurred in 38% (95% CI 15% to 64%; I2=98.14%) of women (4 studies; n=856) (figure 2B). Reported rates of bleeding were significantly higher after a longer follow— up period,but this comparison is limited to a single small (n=74)study reporting after 4 months (figure 2B). Duration of bleeding was reported by 3 studies with one finding a median of 3.3 days (IQR=2—5 days), another reporting a mean of 10.6 days (±5.8), and the last reporting a mean of 10 days (online supplemental table S1).
Vaginal discharge
Vaginal discharge was ascertained at follow— up visits only and reported by 72% (95% CI 18% to 100%; I2=99.55%)of women (5 studies; n=771) (figure 2C). The duration of vaginal discharge was also reported by three of these studies with a mean ranging from 15 days to 17 days,and by another with a median of 14 days (online supple—mental table S1). Vaginal discharge did not differ based on timing of follow— up visit (figure 2C).
Other side effects
There were no reported hospitalisations following TA and no discontinuation of treatment due to side effects. A range of other side effects were reported in single studies or with unclear definitions that prevented meta— synthesis(online supplemental table S1). Seven cases of vasovagal response or faintness were reported overall with unclear timing.102022Clinical suspicion of infection based on foul smelling vaginal discharge was reported by Mungoet alin two women,19with symptoms resolving following antibi—otics. Vivianoet aldescribes three women with clinically diagnosed infections (specific diagnostic criteria not provided) requiring local antibiotics and an additional 9 women were provided prophylactic antibiotics at the 1— month follow— up visit due to delayed wound healing.21Three studies reported on a sensation of heat during treatment in 88.6%, 25% and 5.9% of women.121922One case of pelvic inflammatory disorder was reported 6 months after treatment (Naudet al) and two cases of pain while urinating (Sandovalet al).2022
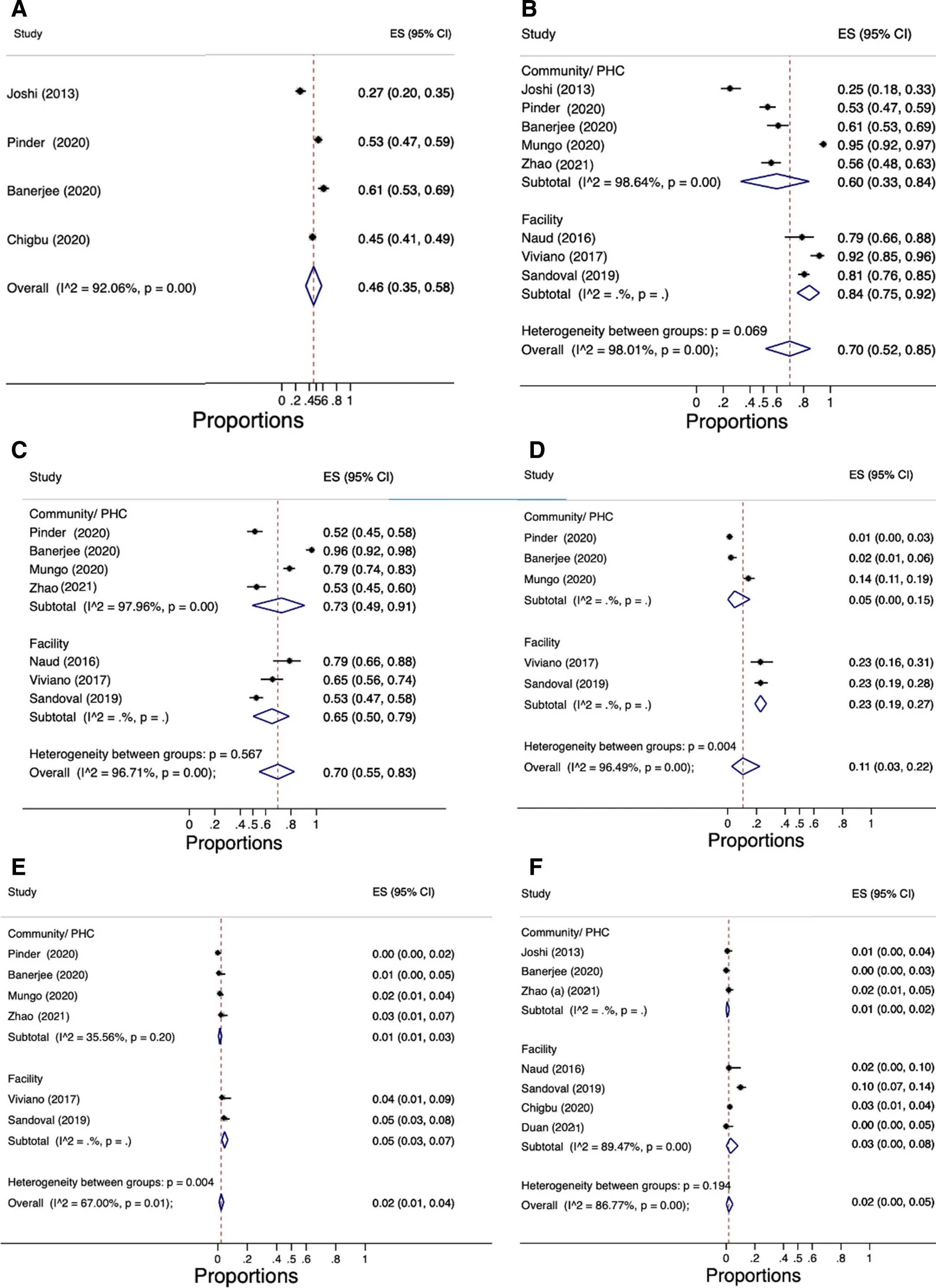
Figure 1 Side effects reported at treatment. (A) One or more side effect at treatment. (B) Pain at treatment, grouped by setting.(C) Mild pain at treatment, grouped by setting. (D) Moderate pain at treatment, grouped by setting. (E) Severe pain at treatment,grouped by setting. (F) Bleeding at treatment, grouped by setting. ES, estimate.
Patient acceptability
Patient acceptability, reported both at treatment and at follow— up, was most often measured as satisfaction with treatment or willingness to recommend the treatment to others (online supplemental table S2). Three studies(n=679) measured satisfaction with treatment as a binary indicator with 99% (95% CI 98% to 100%; I2=0.00%) of women indicating they were satisfied (figure 3A). When reported on a 5— point Likert scale by Chigbuet almean satisfaction was 3.9 (±1.3) at follow— up.18Willingness to recommend treatment to others was nearly universal in the 4 studies (n=998) reporting this measure (100%,95% CI 99% to 100%; I2=0.00%) (figure 3B). Two studies also reported acceptability based on patient experience rated as better or worse than expected immediately after treatment.1819Overall, 84% (95% CI 81% to 86%;I2=0.00%) rated the treatment as better than expected while 7% (95% CI 5% to 8%; I2=0.00%) rated the expe—rience as worse than expected (n=804).1819See online supplemental table S2 for reported acceptability measures in included studies in meta— synthesis.
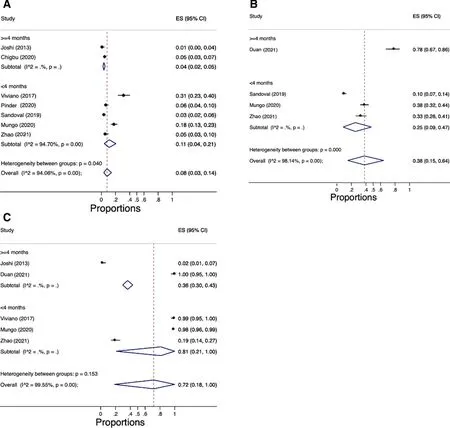
Figure 2 Side effects reported at follow- up. (A) Post- treatment pain at follow- up, grouped by timing of follow- up visit. (B) Posttreatment bleeding at follow- up, grouped by timing of follow- up visit. (C) Post- treatment vaginal discharge at follow- up, grouped by timing of follow- up visit. ES, estimate.
DISCUSSION
Our systematic review and meta— synthesis provides the first comprehensive picture of the current literature on the side effects and acceptability of TA specific to LMIC settings. Commonly reported side effects of TA are predominantly mild. There is a high level of treatment acceptability overall. The most common side effects were mild pain at treatment (70%, 95% CI 55% to 83%),vaginal discharge following treatment (72%, 95% CI 18%to 100%) and bleeding following treatment (38%, 95% CI 15% to 64%). Infection and vasovagal response to treat—ment were rare but did occur in a small number of study participants. Importantly, no side effects led to treatment being discontinued and there were no reported hospital—isations. The high rate of acceptability signals that women are willing to tolerate mild symptoms when undergoing treatment for cervical cancer prevention.
The types of side effects reported in this review of TA resemble those of cryotherapy. Literature reviews on cryotherapy report pain rates up to half of that of TA,ranging between 0% and 30% of women.5729However,when restricting analysis to the four available randomised studies, the WHO reports with moderate certainty that slightly fewer women experience pain when treated with TA (60.8%, 95% CI 49.7% to 75.2%) compared with cryo—therapy (65.4%).5Due to limited research and incon—sistent methodologies, true values remain uncertain.Adverse events following TA such as major bleeding and infections appear to occur at low rates similar to cryo—therapy, with higher rates occurring in those treated by excisional methods.52930
Though it is not expected to differ significantly, we were unable to assess rates of side effects and accept—ability specific to women living with HIV. As a popu—lation at greater risk of developing cervical cancer,31future research should continue to collect data specific to this group. Initial research has shown that women on antiretroviral therapy do not experience an increase in viral shedding following treatment with cryotherapy,suggesting it should not affect the risk of transmis—sion.3233These findings are likely to carry over to TA,though additional research is required to demonstrate it.
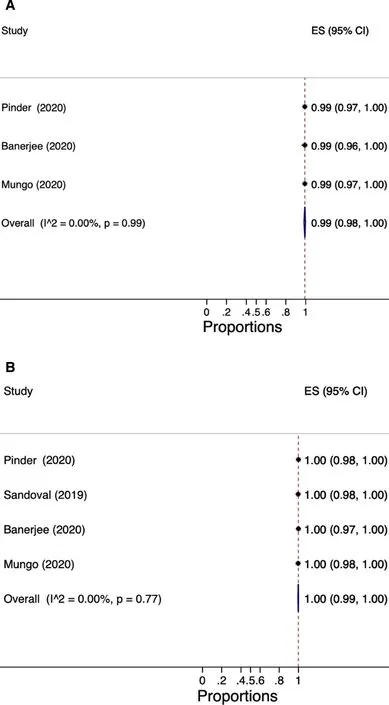
Figure 3 Measures of acceptability. (A) Satisfaction with treatment (yes/no). (B) Willingness to recommend treatment to others. ES estimate.
Applying the search strategy to regional databases allowed for the inclusion of a greater number of relevant publications, though it remained limited to publications in English due to capacity limits in our research team.Additionally, the broad inclusion criteria allowed for a greater number of relevant contexts and diverse study types to be included in the review. However, this also brought limitations such as inconsistent follow— up times,as well as heterogeneity between study populations and treatment methods that likely drove the wide CIs. Use of the random effects model to estimate pooled rates addresses this heterogeneity to some degree. Included studies had considerable heterogeneity in sample size,age, screening and eligibility protocol, data collection and data reporting. Additionally, clear descriptions of data collection and reporting methods were often lacking,a result of our topics of interests often being secondary outcomes in included studies. Only two (Mungoet aland Sandovalet al) of the 15 studies included in this review investigated side effects and acceptability as a primary outcome.1920There is a need for more quality research focused on side effects and measures of acceptability for TA.
A specific limitation in the synthesised pain rate is Sandovalet al’s initial failure to consistently distinguish between pain during the TA procedure and pain during the biopsy, leading to an overestimation of pain caused by TA in that study.20Mungoet alalso recognise this as a potential limitation in their study despite efforts by the research team to differentiate the two during pain assess—ments.19This represents a limitation to our review as well as a caution to future research to clearly distinguish between pain caused by treatment versus other same— day procedures. A standardised reporting method for side effects and acceptability would benefit intratreatment and intertreatment analyses. The side effects of interest identified in this comprehensive review can be used to support consistent future assessments, both at treatment and at follow— up.
Type of probe, treatment time and temperature also varied across included studies. Though greater consis—tency across studies may come from the WHO’s 2019 guidelines for TA, which suggest a minimum of 100°C for 20—30 s,5more research is needed to concretely establish an optimal treatment protocol to minimise side effects and pain. This may be particularly relevant to pain rates as Banerjeeet aland Sandovalet alidentified a positive association between the number of probe applications and reported levels of pain during treatment,920though Mungoet alfound no such association.19Within the included studies, 16%—62% of women required 2—4 appli—cations of the probe to cover the entire TZ.91219202228
Other potential long— term adverse effects of TA, such as its impact on reproductive health outcomes, are key to understanding overall acceptability but were out of scope for this review. Data remain limited, but research non— specific to LMICs report little to no effect of TA on rates of infertility or adverse obstetric outcomes such as premature births.534
Focusing on data collected in LMICs makes this review explicitly relevant to contexts where screen— and— treat programmes using TA are most likely to be implemented.Though overtreatment is inevitable with HPV— based and VIA— based screening, the mild side effects and high acceptability of TA suggest overtreatment should not hinder the implementation of accessible screen— and— treat programmes. Expanding access to screen— and— treat strate—gies by implementing programmes in community clinics is also supported by our findings that such settings resulted in lower rates of moderate and severe pain compared with TA treatment in facilities. This significant varia—tion, however, may be attributed in part to courtesy bias being more acute in smaller community clinics compared with larger facilities during pain evaluation. Continued assessments of TA across treatment settings is needed to support the development of standard protocols. TA is a relatively low cost, portable and rapid treatment option that can be effectively performed by a variety of health—care providers.5The high levels of acceptability, despite common reports of mild pain, support the standard prac—tice to treat without anaesthesia, further reducing barriers to widespread implementation. Primary care givers should continue to counsel women on the common side effects of TA presented here prior to treatment.
Conclusion
Overall, TA is an acceptable treatment method for cervical precancerous lesions with mostly mild side effects.Compared with alternative treatment methods, TA is feasible and effective within screen— and— treat programmes.These findings support the use of TA as an important tool toward achieving the WHO’s 2030 goal of treating 90%of women with detected precancerous lesions in LMICs as part of the 90—70—90 targets. Continued assessments of the side effects and acceptability of TA in low— resource settings are needed to support the optimal implementa—tion of screen— and— treat programmes.
AcknowledgementsWe thank the UBC research librarian for her guidance and expertise with database searching as well as the Global HPV student group at the Women’s Health Research Institute at BC Women’s Hospital for their guidance and support during EMP’s internship.
ContributorsEMP was responsible for the literature search, abstract and full text review, data extraction and writing-original draft. BP was responsible for study design and conceptualisation, development of methodology, abstract and full text review, risk of bias assessment, formal data analysis, interpretation of results and writing-reviewing and editing. LWS was responsible for conceptualisation,interpretation of results and writing-review and editing. JT was responsible for development of methodology and writing-review and editing. JO was responsible for interpretation of results and writing-review and editing. GO and CN was responsible for conceptualisation, funding acquisition, supervision, interpretation of results and writing-review and editing.
FundingSalary support for EMP, BP, LWS and JT was provided through a grant awarded to the principle investigator GO from the Canadian Institutes of Health Research (CIHR) for the ASPIRE Mayuge Trial (ISRCTN12767014; registered on 14 May 2019). The CIHR had no role in data collection, analysis, interpretation, report writing or the decision to submit this manuscript.
Competing interestsNone declared.
Patient consent for publicationNot applicable.
Ethics approvalNot applicable.
Provenance and peer reviewNot commissioned; externally peer reviewed.
Supplemental materialThis content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer- reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines,terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Open accessThis is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially,and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
ORCID iD
Evelyne Marie Piret http://orcid.org/0000-0001-9569-4989
杂志排行

Family Medicine and Community Health的其它文章
- Development and validation of the scale for measuring biopsychosocial approach of family physicians to their patients
- Acceptability of a task sharing and shifting model between family physicians and physiotherapists in French multidisciplinary primary healthcare centres: a cross- sectional survey
- Transitions in health service use among women with poor mental health: a 7- year follow- up
- Putting health workers at the centre of health system investments in COVID- 19 and beyond
- COVID- 19 vaccine hesitancy and related factors among primary healthcare workers in a district of Istanbul: a crosssectional study from Turkey
- Patient experience of residents with restricted primary care access during the COVID- 19 pandemic