lmpact of utilization of hepatitis C positive organs in liver transplant:Analysis of united network for organ sharing database
2022-07-04AmaninderDhaliwalBanreetDhindsaDarylRamaiHarlanSaylesSaurabhChandanRajaniRangray
Amaninder Dhaliwal,Banreet Dhindsa,Daryl Ramai,Harlan Sayles,Saurabh Chandan,Rajani Rangray
Amaninder Dhaliwal,Department of Gastroenterology and Hepatology,Moffitt Cancer Center,Tampa,FL 33612,United States
Βanreet Dhindsa,Department of Gastroenterology and Hepatology,University of Nebraska Medical Center,Omaha,NE 68198,United States
Daryl Ramai,Department of Internal Medicine,The Brooklyn Hospital Center,Brooklyn,NY 11201,United States
Harlan Sayles,Department of Biostatistics,University of Nebraska Medical Center,Omaha,NE 68198,United States
Saurabh Chandan,Rajani Rangray,Department of Gastroenterology and Hepatology,Creighton University Medical Center,Omaha,NE 68124,United States
Abstract BACKGROUND The utility of hepatitis C virus(HCV)organs has increased after the Food and Drug Administration approval of direct acting anti-viral(DAA)medications for the HCV treatment.The efficacy of DAA in treating HCV is nearly 100%.AIM To analyze the United Network for Organ Sharing(UNOS)database to compare the survival rates between the hepatitis C positive donors and negative recipients and hepatitis C negative donors and recipients.METHODS We analyzed the adult patients in UNOS database who underwent deceased donor liver transplant from January 2014 to December 2017.The primary endpoint was to compare the survival rates among the four groups with different hepatitis C donor and recipient status:(Group 1)Both donor and recipient negative for HCV(Group 2)Negative donor and positive recipient for HCV(Group 3)Positive donor and negative recipient for HCV(Group 4)Both positive donor and recipient for HCV.SAS 9.4 software was used for the data analysis.Kaplan Meier log rank test was used to analyze the estimated survival rates among the four groups.RESULTS A total of 24512 patients were included: Group 1: 16436,Group 2: 6174,Group 3: 253 and Group 4: 1649.The 1-year(Group 1: 91.8%,Group 2: 92.12%,Group 3: 87%,Group 4: 92.8%),2-year(Group 1: 88.4%,Group 2: 88.1%,Group 3: 84.3%,Group 4: 87.5%),3-year(Group 1: 84.9%,Group 2: 84.3%,Group 3: 75.9%,Group 4: 83.2%)survival rates showed no statistical significance among the four groups.Kaplan Meier log rank test did not show any statistical significance difference in the estimated survival rates between Group 3 vs all the other groups.CONCLUSION The survival rates in hepatitis C positive donors and negative recipients are similar as compared to both hepatitis C negative donors and recipients.This could be due to the use of DAA therapy with cure rates of nearly 100%.This study supports the use of hepatitis C positive organs in the selected group of recipients with and without HCV infection.Further long-term studies are needed to further validate these findings.
Key Words: Hepatitis C;Liver transplant;Survival;United Network for Organ Sharing;Direct acting antiviral
lNTRODUCTlON
In the United States,there has been increase in the number of cases in need for liver transplantations(LT)in the last decade while the availability of organs is unchanged[1].The major contributing factor to this is limited availability of donor liver.Due to persistence of viable organ shortage in United States,it is of utmost importance that all transplantable organs are utilized to their maximum potential[2].With the advent of direct acting anti-viral(DAA)therapy,the rate of cure of hepatitis C virus(HCV)has increased dramatically.This has been reflected by nonalcoholic fatty liver disease and alcoholic liver disease overtaking HCV as the leading cause for LT in the United States[1,2].The rates of HCV-positive waitlisted patients and HCV-positive LT recipients have decreased by 8.2% and 7.6% respectively between 2006 and 2016[1].
Prior to approval of DAA therapy,recurrence of HCV after LT was the most common cause of graft failure and reduced recipient survival in those for were HCV positive as compared to HCV negative patients[3,4].This recurrence of HCV greatly influenced the allocation of HCV positive donors leading to severe under-utilization of these organs,especially in HCV negative recipients[5-8].Development of newer generation DAAs have resulted in interferon free regimens with high sustained virologic response(SVR)rates post LT[9-12].
These newer generation DAAs have high potency and low adverse event rates leading to increase in inclination for utilizing HCV positive donor organs,including those with high viral load.However,concerns exist regarding these medications as 5% of the patients have failure to achieve SVR after undergoing DAA therapy.This puts the patients at risk for developing chronic HCV or cholestatic hepatitis with increased possibility of need of re-transplantation.
The aim of this study is perform a comparative analysis on odds of survival between the HCV positive donors and negative recipients as compared to HCV negative donors and recipients,using United Network for Organ Sharing(UNOS)database.
MATERlALS AND METHODS
We obtained data from the UNOS registry which contains data on all transplantations in the United States.Analysis was limited to records from April 1,2014 or later,where both recipient and donor were at least 18 years or age,and HCV status was recorded for both recipient and donor.Some recipients appeared in the data set multiple times,but analysis for this study was limited to the first transplant recorded for each patient using a data element which recorded the number of previous transplants for each recipient.The remaining observations were classified into four groups based upon the HCV status of both donors and recipients:(Group 1)both donor and recipient negative,(Group 2)negative donor and positive recipient,(Group 3)positive donor and negative recipient,and(Group 4)both donor and recipient positive.
Descriptive statistics for each of the four groups,including demographic and clinical characteristics for both recipients and donors and causes of death were calculated using means and standard deviations for continuous measures and counts and percentages for categorical measures.The primary outcome was overall survival time with death indicated using the composite death indicator and censoring for those who did not die during the study period occurring at the date of last patient followup with the latest patient follow-up taking place on September 7,2018.Note that all surviving patients were not censored at this date,this is just the latest date a patient was observed.Comparisons of overall survival between groups were made using log-rank tests and estimates of group survival at various time points following transplant.All analysis was completed using SAS v9.4(The SAS Institute,Cary,NC).
RESULTS
We included a total of 24512 transplants in our analysis.Group 1 and 2 formed the majority of the transplants with 67.05% and 25.19% respectively.Group 3 consisted of 1.03% of transplants with 253 patients undergoing positive donor and negative recipient transplants while the remaining 6.73% were in Group 4.The percentages of males in the four groups were 62.87,75.92,66.80 and 76.53,respectively.The mean age(years)of recipients was comparable: Group 1(54.66 ± 11.63),Group 2(59.08 ± 6.82),Group 3(56.13 ± 10.9)and Group 4(58.92 ± 6.76).The mean age of donors was comparable as well: Group 1(42.72 ± 15.60),Group 2(42.96 ± 15.09),Group 3(40.00 ± 12.41)and Group 4(37.71 ± 11.82).
Cold ischemia times(hours)were similar in all the groups Group 1(6.07 ± 2.23),Group 2(6.20 ± 2.46),Group 3(6.45 ± 2.03)and Group 4(6.15 ± 2.51).The mean body mass index of the recipients were evenly matched as well: Group 1(29.1 ± 6.12),Group 2(28.67 ± 5.38),Group 3(28.92 ± 6.08)and Group 4(28.92 ± 6.08).The mean model for end-stage liver disease(MELD)scores were also similar in all groups: Group 1(25.22 ± 10.86),Group 2(19.41 ± 11.26),Group 3(21.74 ± 8.39)and Group 4(18.24 ± 7.95).
Anoxia was the most common cause of death(37.89%)followed by stroke(31.31%)and head trauma(28.4%).Majority of the transplants in all groups were whole LT: Group 1(99.05%),Group 2(99.14%),Group 3(99.60%)and Group 4(99.94%).These demographics can be seen in Tables 1 and 2.The most common primary diagnosis at listing was alcoholic cirrhosis/acute alcoholic hepatitis(26.26%)followed by HCV cirrhosis(20.92%),non-alcoholic steatohepatitis cirrhosis(15.36%)and hepatoma(12.28%).These can be seen in Table 3.
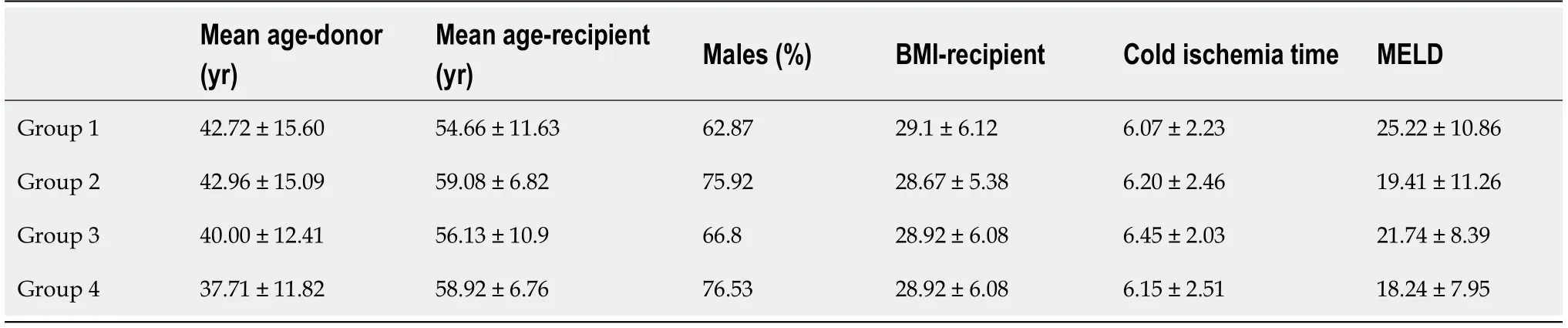
Table 1 Demographics of different transplanted groups
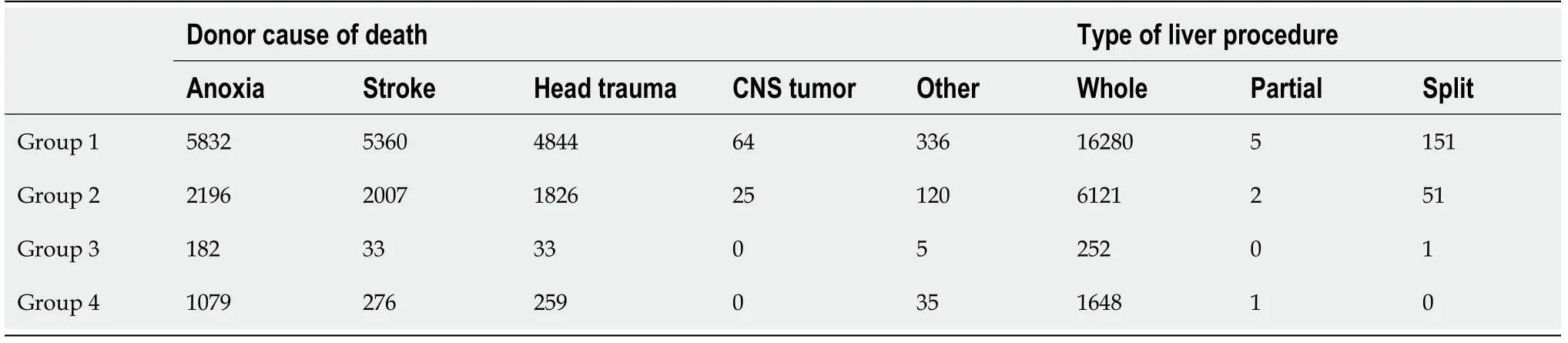
Table 2 Cause of donor death and type of liver transplant in different groups
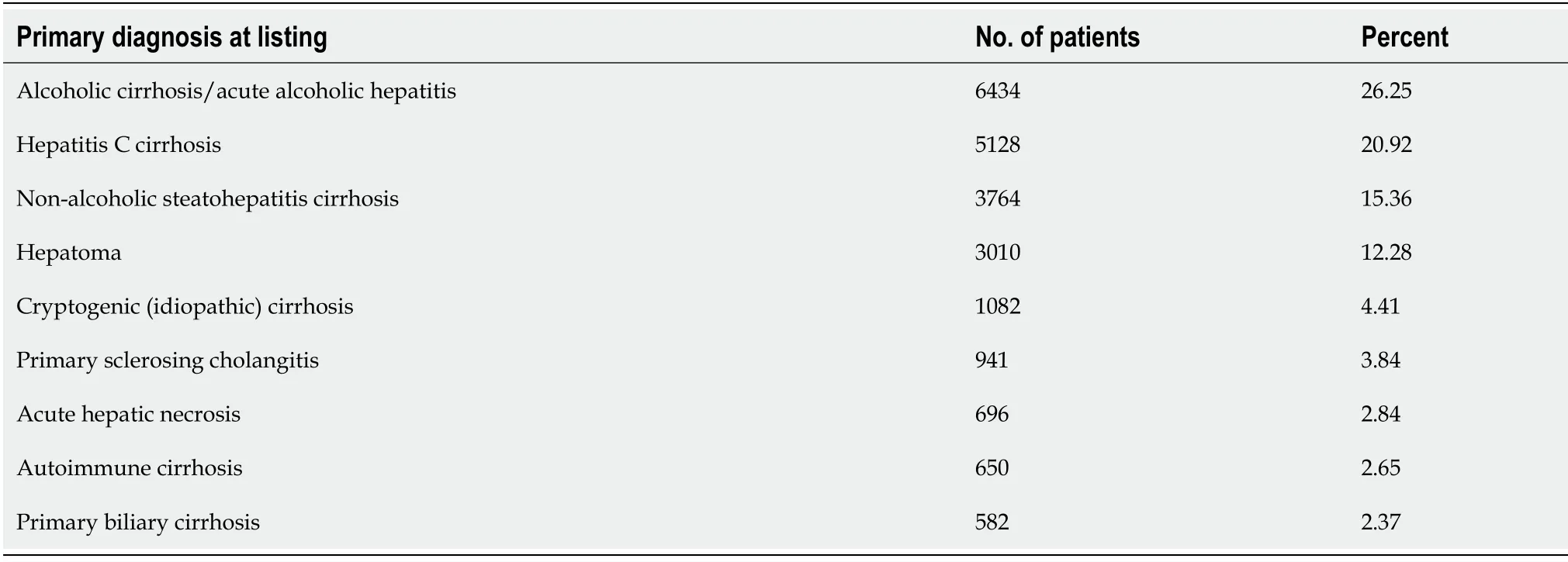
Table 3 Diagnosis of transplant recipients at the time of listing
A log-rank test for survival differences between the four groups did not show any significance(P= 0.46).Observation of survival rates at 1-year(Group 1: 91.81%,Group 2: 92.13%,Group 3: 87.01%,Group 4: 92.89%),2-year(Group 1: 88.4%,Group 2: 88.1%,Group 3: 84.3%,Group 4: 87.5%),3-year(Group 1: 84.9%,Group 2: 84.3%,Group 3: 75.9%,Group 4: 83.2%)found that survival rates for Group 3 were lower at each point than the other three groups,which were all relatively close together.However,a second long-rank test comparing Group 3vsall the other groups was also not significant(P= 0.11,Figure 1).
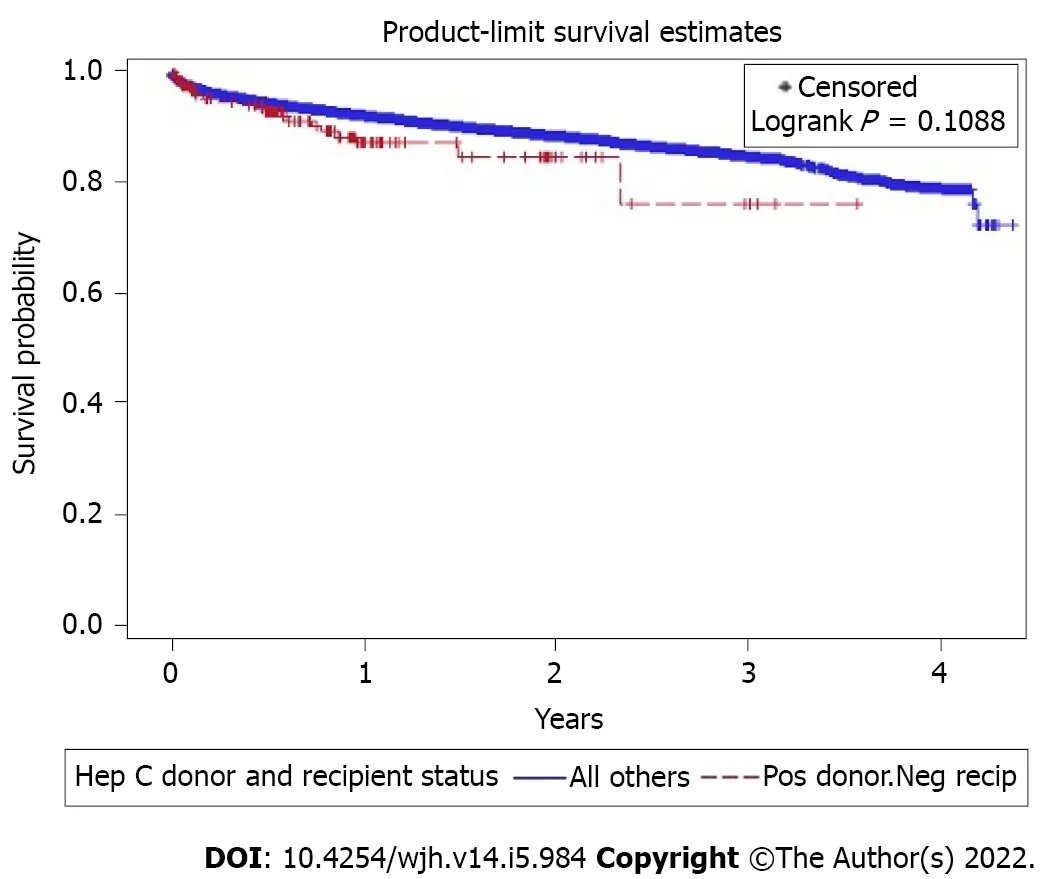
Figure 1 Kaplan Meier curve showing survival analysis between group 3 and other groups.
DlSCUSSlON
Despite the increasing number of LT over the years,the need for organ donors continues to outpace the availability of organs with estimated waitlist mortality of 20%[13].
In the United States,since 2000,the increased mortality related to the catastrophic opioid epidemic presented an opportunity to recruit more organ donors.However,the enthusiasm was curtailed by a relatively higher prevalence of HCV when compared to the general population[14].Initially,the organsfrom HCV+ donors were primarily reserved for HCV+ recipients or those suffering from fulminant hepatic failure[15].But there is still a reticence to use organs from HCV+ donors in HCV- recipients because of clinical and ethical considerations.
One of the biggest barriers to use HCV+ donor organs is the concern for increased risk of posttransplant HCV transmission.Another concern with the use of HCV+ donor liver grafts is because of the limited literature on post-transplantation outcomes.Laiet al[16]studying 99 recipients of HCV+ donor liver grafts demonstrated significantly higher unadjusted 1-year and 3-year rates of advanced fibrosis for recipients of HCV+ donor grafts(14% and 48%)vsHCV- donor grafts(7% and 33%,P= 0.01)[16].Khapraet al[17]studying 29 recipients of HCV+ donor liver grafts showed significantly more fibrosis and a faster rate of progression compared with recipients of HCV- donor liver grafts[17].Interestingly,when the analysis was stratified to mean donor age,both the studies showed poorer outcomes with older donors of age greater than 45 years and 50 years respectively[16,17].But it must be noted that these studies were done in an era when antiviral therapy was initiated at later stages of fibrosis and there was low response to these regimens.At this time,more studies with longer follow up are needed to see if similar rates of fibrosis progression occur with early administration of antiviral therapy post-transplantation.
In terms of long-term graft and patient survival with HCV+ organs,the current literature is controversial depending on the type and success rate of HCV treatment regimens.With the advent of DAAs,recent studies from single-center experiences and large population-based databases such as UNOS and scientific registry of transplant recipients studying recipients with HCV+ and HCV- liver donors showed similar outcomes between the groups which are encouraging[18-20].But it must be highlighted as there is no standardized protocol currently,these studies included recipients initiated on preemptive or prophylactic or both the treatment regimens.
With increasing wait-list mortality,higher mortality in patients with higher MELD(> 35 scores),and newer DAAs medications reaching clinical efficacy of nearly 96% it may be worth considering offering HCV+ donor organs to selected HCV- recipients where the risk-benefit outweighs the ethical considerations[21].
The data included in our study is from a large population-based study from an accepted UNOS database which includes a heterogeneous population from across the United States.Our study demonstrates that there is no statistically significant difference in the survival rates in HCV positive donors and negative recipients and HCV negative donors and recipients.In contrast to prior studies,which looked at the short-term outcomes such as survival rate at discharge,rejection rate prior to discharge,and 1-year mortality: Ours is the first study that shows that the survival rates were comparable in all group up to 3 years.Furthermore,the mean MELD score of the recipients in the group 3 was 21,suggesting that HCV+ donors can be used in recipients with high MELD score.Moreover,HCV positive organs were utilized in complicated cases with prolonged ischemia times and blood loss,showing tolerance to ischemia.This study supports the feasibility of expanding the general donor poolviathe utilization of HCV positive organs for both HCV positive and negative recipients.
Due to the limitations of the data,we could not evaluate the reduction in time from listing to transplant,we can conclude that addition of HCV positive donor should decrease the organ shortage and reduce morbidity and mortality of all patients on the transplant list.
Although the outcomes of using hepatitis C positive donors are encouraging,there are some limitations of our study.The number of patients in group 3 were less,253 out of total 24512 patient(1.03%).Even though we had estimates of survival rates up to 3 years(and longer for a small set of patients),long-term outcomes are still unknown.Additionally,it is still not clear whether preemptive or prophylactic HCV regimens are needed,and the length of HCV surveillance needed post-LT.Though the mean age of the donors were comparable in all groups,the medical co-morbidities of donors were unknown.In contrast to the study by Ballarinet al[22]this study was limited by the paucity of data on viral load and graft histology of both donors and recipients which may influence post LT outcomes.We also did not have information regarding the treatment status of HCV positive donors.
CONCLUSlON
In summary,due to the mismatch in need and availability of donor organs and high mortality rate on the transplant waiting list,newer strategies are needed.DAA regimens have proved to be highly effective to treat HCV,even post-transplant and immunosuppressed patients.Effectiveness of these regimens can be exemplified by similar survival rates of HCV positive donor and negative recipients in comparison to HCV negative donors and recipients.Our study shows that HCV positive organs can be transplanted to recipients,irrespective of their HCV status.However,more studies are needed to confirm our findings.
ARTlCLE HlGHLlGHTS
Research background
Due to the mismatch in need and availability of donor organs and high mortality rate on the transplant waiting list,newer strategies are needed.In the era prior to direct acting anti-virals(DAAs),recurrence of hepatitis C virus(HCV)in post liver transplantations(LT)patients leading to decreased graft survival had greatly influenced the under-utilization of these organs,especially in HCV negative recipients.With the high sustained virologic response rate with DAAs both pre and post LT,this pool of organs can be utilized leading to more organ availability and decreased in mortality rate on transplant.
Research motivation
There is limited data evaluating outcomes of hepatitis C positive donor organs to HCV negative recipients in LT.
Research objectives
The aim of this study is perform a comparative analysis on odds of survival between the HCV positive donors and negative recipients as compared to HCV negative donors and recipients United Network for Organ Sharing(UNOS)database.
Research methods
We included patients in UNOS database who underwent deceased donor LT over a period of three year.Data analysis was performed using SAS 9.4 software.Survival rates amongst groups were analyzed with help of Kaplan Meier log rank test.
Research results
Our study shows similar chance of survival of recipient,irrespective of HCV status of the donor.
Research conclusions
Our study shows that HCV positive organs can be transplanted to recipients,irrespective of their HCV status due to the advent of DAA regimen.
Research perspectives
More studies are needed to confirm findings of this study.
FOOTNOTES
Author contributions:Dhaliwal A analysis and interpretation of data,drafting the article;Dhindsa B drafting the article;Ramai D acquisition of data;Sayles H analysis and interpretation of data;Chandan S critical revision;Rangray R critical revision,final approval.
lnstitutional review board statement:No IRB approval needed as this is a database study.
Conflict-of-interest statement:The authors deny any conflict of interest.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:United States
ORClD number:Amaninder Dhaliwal 0000-0002-9761-437X;Banreet Dhindsa 0000-0002-9858-0941;Daryl Ramai 0000-0002-2460-7806;Harlan Sayles 0000-0002-4082-8289;Saurabh Chandan 0000-0002-2661-6693;Rajani Rangray 0000-0003-0913-8164.
S-Editor:Fan JR
L-Editor:A
P-Editor:Fan JR
杂志排行

World Journal of Hepatology的其它文章
- Role of hepatitis Β virus in development of hepatocellular carcinoma:Focus on covalently closed circular DNA
- Emerging curative-intent minimally-invasive therapies for hepatocellular carcinoma
- Saving time and effort: Βest practice for adapting existing patientreported outcome measures in hepatology
- Loco-regional treatment of hepatocellular carcinoma:Role of contrast-enhanced ultrasonography
- Βenign focal liver lesions:The role of magnetic resonance imaging
- Pediatric acute viral hepatitis with atypical variants:Clinical dilemmas and natural history