Spontaneous healing after conservative treatment of isolated grade IV pancreatic duct disruption caused by trauma: A case report
2022-06-27MingZhenMeiYuFengRenYiPingMouYuanYuWangWeiWeiJinChaoLuQiCongzhu
Ming-Zhen Mei, Yu-Feng Ren,Yi-Ping Mou, Yuan-Yu Wang, Wei-Wei Jin, Chao Lu, Qi-Cong zhu
Abstract
Key Words: Trauma; Pancreatic ducts; Conservative treatment; Drainage; Case report
lNTRODUCTlON
Trauma is a common cause of pancreatic duct disruption. Surgical treatment is recommended in current clinical guidelines for adult pancreatic injury because, compared with surgical treatment, non-surgical treatments have higher risks of serious complications or even death[1,2]. In this study, we report a case of pancreatic duct disruption in the head and neck caused by trauma that was treated conservatively and which healed spontaneously.
CASE PRESENTATlON
Chief complaints
A 22-year-old female patient was admitted to Tiantai People’s Hospital of Zhejiang Province on 13 July 2020 after 1-hour duration of abdominal pain and distension following trauma.
History of present illness
The patient experienced sudden-onset persistent and unbearable abdominal pain, radiating to the lower back, with abdominal distension and nausea, and without vomiting, coma, dizziness, headache, chest tightness, shortness of breath, bloody vomiting, or hemoptysis. The trauma resulted from impact with bicycle handlebars on the upper abdomen during an electrical bicycle accident 1 h earlier.
She had no other complaints. Her sleep and appetite were normal, and her excretion and egestion were both normal.
History of past illness
The patient had an unremarkable medical history.
Personal and family history
The patient grew up in her locality, denied any contact with contaminated water or radiation exposure,and did not smoke or consume alcohol. She had no gestational history, and her annual menstruation cycle was 13/year (q 4-6 wk/duration: 20-30 d).
Physical examination
Physical examination findings on admission: body temperature: 37.2 ℃, respiratory rate: 20 breaths/min, blood pressure: 118/63 mmHg, and heart rate: 103 beats/min. The patient had a clear mind, low mood, flat and soft abdomen, tenderness in the upper abdomen, no obvious rebound pain,bowel sounds: 2/min, and no shifting dullness. No other significant abnormalities were observed.
Laboratory examinations
Serum amylase concentration: 1258 U/L (upper limit of normal: 135 U/L), white blood cell count: 17.8 ×109/L, neutrophils: 82%, red blood cell count: 4.51 × 1012/L, hemoglobin: 143 g/L, platelet count: 211 ×109/L, C-reactive protein: < 0.499 mg/L, and procalcitonin: < 0.02 ng/mL; liver and kidney function was normal, the levels of plasma lactate was normal.

Figure 1 Contrast-enhanced abdominal computed tomography, which shows a morphologically smooth pancreatic neck/head with small lamellar high-density shadows at the anterior edge, with no significant enhancement.
Imaging examinations
Abdominal computed tomography (CT): The pancreatic head/neck was full in shape, and small lamellar high-density shadows were seen at the anterior edge, with a CT value of 64 HU. There was no edema and thickening of bilateral anterior renal fascia and no peritoneal or retroperitoneal effusion. The lesion was not significantly enhanced during contrast-enhanced CT, and some surrounding low-density exudative shadows were observed (Figure 1).
FlNAL DlAGNOSlS
The diagnosis was “traumatic pancreatic rupture”.
TREATMENT
The patient was informed that her condition was critical, and there were indications for emergency surgery; however, the patient’s symptoms were not severe, her vital signs were stable, and signs of peritonitis were not obvious. Therefore, conservative treatment could be considered, with the possibility of emergency surgery if necessary. The patient was then treated with fasting, gastrointestinal decompression, acid control, digestive enzyme inhibition, anti-inflammation, and fluid replacement.After treatment, her abdominal pain was relieved. Abdominal CT on 14 July 2020 revealed lamellar high-density shadows in the pancreatic head and neck, with no significant increase in fluid collection,and with obvious exudative shadows around the pancreas; fluid accumulation was evident in the abdominal cavity. Conservative treatment was continued, and the patient’s condition gradually improved. A naso-intestinal tube was placed for enteral feeding on 20 July 2020, which was welltolerated. Repeat ultrasonography on 23 July 2020 revealed local fluid collection in the neck of the pancreas measuring approximately 60 mm × 46 mm × 38 mm and no obvious fluid accumulation in the abdominal cavity. Therefore, catheter drainage of the peripancreatic fluid collection was performed, and approximately 300 mL of pale bloody fluid was removed. Repeat abdominal CT on 24 July 2020 revealed local dissection of the pancreatic head/neck, encapsulated effusion in the form of a pseudocyst measuring 17 mm × 31 mm, and a small amount of fluid in the abdominopelvic cavity (Figure 2). The patient was transferred to Zhejiang Provincial People's Hospital for follow-up treatment on 27 July 2020,during which inflammatory indices were normal, and serum total amylase reached a maximum of 932 U/L (upper limit of normal: 135 U/L), with no significant fluid exiting the drain. Abdominal CT was repeated and revealed that the pancreatic head/neck was morphologically swollen, with increased surrounding encapsulated fluid. Ultrasound-guided peripancreatic catheter drainage by transperitoneal was performed again, and 300 mL of clear pancreatic fluid was removed. The serum amylase concentration decreased to normal after this drainage. On 24 August 2020, puncture pancreatography visualized the distal pancreatic duct. On 25 August 2020, endoscopic retrograde cholangiopancreatography (ERCP) was performed to place a pancreatic duct stent. The pancreatic duct in the pancreatic head was circular in shape and was not connected with the pancreatic duct in the pancreatic body/tail.Therefore, the pancreatic duct stent could not be placed.
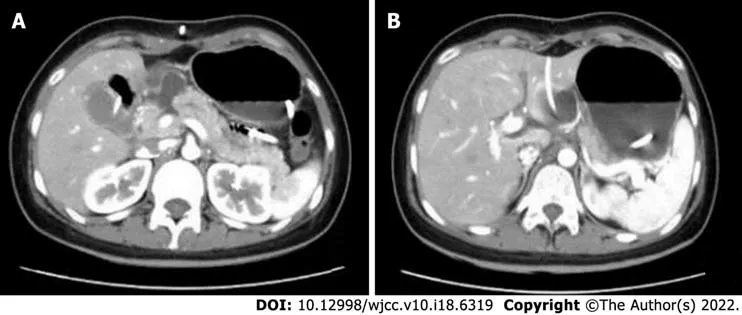
Figure 2 Abdominal computed tomography. A: Localized rupture of the pancreatic head/neck; B: A pseudocyst, drained with a catheter.

Figure 3 Magnetic resonance cholangiopancreatography showing a slightly dilated pancreatic duct in the pancreatic tail.
OUTCOME AND FOLLOW-UP
The main pancreatic duct was not dilated by transpuncture tube angiography, and there was no obvious liquid dark areas around the pancreas; therefore, the puncture drain was removed. Re-examination on 10 November 2020 revealed that the patient had no discomfort and no abnormalities on physical examination. The serum amylase concentration was 44 U/L. Magnetic resonance cholangiopancreatography (MRCP) suggested slightly dilated pancreatic ducts in the pancreatic tail (Figure 3).
DlSCUSSlON
The pancreas is a retroperitoneal organ with a deep and hidden location, and pancreatic injury occurs in only 0.4%-6.0% of abdominal trauma cases[1]. The pancreas is located in front of the first and second lumbar vertebrae; therefore, injury is often caused by direct action on the spine owing to crushing force from the upper abdomen, mostly sustained in the pancreatic body. Approximately 39% of pancreatic injuries are associated with pancreatic duct disruption[2]. Isolated pancreatic injury is even more rare,comprising less than 3% of cases[3].
The level of serum amylase has little significance for the early diagnosis of pancreatic trauma. Serum amylase cannot be increased in about 40% of patients, and it can also be increased in non-pancreatic injury and intestinal injury[4]. Adamsonet al[5] conducted a retrospective study on 1821 patients with trauma. The level of serum amylase or lipase increased in 116 patients, and only 8 patients finally identified pancreatic trauma. The significance of serum amylase or lipase in the diagnosis of pancreatic trauma is limited, and it also depends on the necessary imaging examination. Currently, CT is the firstline technique for evaluating pancreatic injury. CT is easy to perform, and its high imaging quality, clear display of the pancreatic contours and peripancreatic bleeding, and the option for multiplanar reconstruction, can achieve a diagnostic accuracy rate of > 80%. However, there are limitations in the diagnosis of pancreatic duct disruption, and the accuracy rate needs to be improved by dynamic review[6]. In this case, we performed dynamic CT review to clarify the presence of pancreatic duct disruption.According to the American Association for the Surgery of Trauma (AAST) classification of pancreaticinjuries, injuries involving the pancreatic duct are classified as grade III or IV injuries, as outlined in Table 1[7]. For hemodynamically stable patients, MRCP can be performed when further clarification of pancreatic duct integrity is needed during follow-up treatment. MRCP has the advantages of being noninvasive and providing accurate pancreatic duct imaging. In this case, complete rupture of pancreatic neck was well established by computed tomography (Figure 2A), so we did not perform MRCP. ERCP can lead to a series of complications, such as bleeding, perforation, and iatrogenic pancreatitis, and is more often used for treatment. This patient’s admission serum amylase concentration was significantly elevated, and the diagnosis of pancreatic duct disruption was confirmed when the elevated amylase finding was combined with the dynamic CT review.

Table 1 American Association for the Surgery of pancreatic trauma for the pancreas
The management of pancreatic injuries is controversial and based on small retrospective studies.There are no randomized studies addressing this issue. Based on the available class III evidence, the Eastern Association for the Surgery of Trauma recommended drainage for Grade 1 and Grade 2 injuries and resection with drainage for Grade 3 or higher[8]. Siboniet al[3] study found nonoperative management of minor isolated pancreatic injuries is associated with lower mortality and shorter hospital stay than operative management. However, in severe trauma, nonoperative management is associated with higher mortality and longer hospital stays than operative management[3].
Mohseniet al[9] research showed pancreatic resection for the treatment of grade III and IV penetrating pancreatic injury is not associated with a significant decrease in mortality but is associated with a significant increase in hospital length of stay. Drainage alone of the pancreatic bed may be a viable option, even for high-grade injuries[9]. For traumatic pancreatic injury, the optimal treatment strategy can be formulated only when the patient’s vital signs, abdominal signs, degree of pancreatic injury, and the presence of surrounding organ injury are considered comprehensively.
Recently, the use of endoscopic stenting of the pancreatic duct for the successful treatment of pancreatic duct disruption has been increasingly reported[10]. In a recently published report showing patients with pancreatic trauma who had received pancreatic stents undergoing ERCP 0-15 d after the trauma, the stents were removed after 4-8 wk and at follow-up between 6-24 mo. Endoscopic stent treatment may avoid emergency pancreatic resection and should always be considered in the management of patients with traumatic pancreatic duct injury[11]. When the patient is admitted to our hospital, the condition of this case was stable, so we did not chose pancreatic duct stent implantation.Compared with pancreatic resection, which is highly invasive and affects patients’ quality of life,endoscopic treatment is undoubtedly a new treatment strategy and is gradually gaining more attention.
CONCLUSlON
In this case, after 2 mo of conservative treatment with duct drainage, the pancreatic duct healed spontaneously with no significant complications. This case provides a new consideration for clinical practice: In isolated pancreatic injury with rupture of the pancreatic duct in the head and neck, conservative treatment under close observation is feasible. In young and fit populations with stable hemodynamics, no signs of peritonitis, and no obvious active bleeding on abdominal CT, conservative treatment can be considered first, combined with dynamic CT review and fluid drainage. Endoscopic pancreatic duct stenting can then be considered if appropriate because, in some cases, the pancreatic duct can heal spontaneously.
FOOTNOTES
Author contributions:Mei MZ and Ren YF have contributed equally to this work; Mei MZ and Ren YF made substantial contributions to acquisition of data, analysis, and interpretation of data; Mou YP, Wang YY, Jin WW, Lu C, and Zhu QC made substantial contributions to the conception, acquisition of data, analysis, and interpretation of data; all authors have been involved in drafting the manuscript and revising it critically for important intellectual content; All authors read and approved the final manuscript and take public responsibility for appropriate portions of the content and agree to be accountable for all aspects of work.
Supported byTraditional Chinese medicine Science and Technology Project of Zhejiang Province, No. 2020ZB029.
lnformed consent statement:Written informed consent was obtained from the patient for the publication of this case report and the accompanying images.
Conflict-of-interest statement:The authors declare that they have no competing interests.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Ming-Zhen Mei 0000-0003-0673-5748; Yu-Feng Ren 0000-0003-4605-2271; Yi-Ping Mou 0000-0002-0778-6022; Yuan-Yu Wang 0000-0001-8462-7211; Wei-Wei Jin 0000-0002-2974-9598; Chao Lu 0000-0003-0050-1086; Qi-Cong Zhu 0000-0003-3281-7288.
S-Editor:Gong ZM
L-Editor:Filipodia
P-Editor:Gong ZM
杂志排行

World Journal of Clinical Cases的其它文章
- Diabetes mellitus susceptibility with varied diseased phenotypes and its comparison with phenome interactome networks
- Sequential chemotherapy and icotinib as first-line treatment for advanced epidermal growth factor receptor-mutated non-small cell lung cancer
- Impact of preoperative carbohydrate loading on gastric volume in patients with type 2 diabetes
- Disseminated strongyloidiasis in a patient with rheumatoid arthritis: A case report
- CYP27A1 mutation in a case of cerebrotendinous xanthomatosis: A case report
- Postoperative multiple metastasis of clear cell sarcoma-like tumor of the gastrointestinal tract in adolescent: A case report