Postoperative multiple metastasis of clear cell sarcoma-like tumor of the gastrointestinal tract in adolescent: A case report
2022-06-27WenPengHuangLiMingLiJianBoGao
lNTRODUCTlON
Clear cell sarcoma-like tumor of the gastrointestinal tract (CCSLGT) is a rare malignant mesenchymal soft tissue tumor that can occur in any part of the gastrointestinal tract, mostly in the small intestinal wall, followed by the stomach, colon and peritoneum[1,2]. Zambrano
[3] first reported in 2003 that,because of the characteristic appearance of osteoclast-like giant cells in the tumor, they believed that this type of tumor had some but not all of the characteristics of soft tissue clear cell sarcoma. The etiology and pathogenesis of CCSLGT are not clear. Its genetic feature is
gene rearrangement, which is seen in 81% of cases[4]. Histologically, CCSLGT shows diffuse sheet-like or irregular nest-like arrangement of interstitial tumor cells infiltrating the mucosal and plasma layers of the gastrointestinal wall, with visible pseudopapillary and pseudokryoid mass structures, mucus-like interstitium and focal necrosis, lightly stained or transparent cytoplasm, small or inconspicuous nucleoli, active mitosis, and scattered distribution of osteoblast-like multinucleated giant cells in about 50% of cases[5-7]. Immunohistochemistry was characterized by positive expression of Smur100 protein and SOX-10, but no expression of melanocyte markers such as HMB45 and Melan A. Dense secretory granules were seen in the ultrastructure, but no melanosomes were seen, suggesting neuroendocrine differentiation. CCSLGT is more common in young people and children; the age of onset is 5-81 years; there is no gender difference; the tumor can invade the serosa and even involve the surrounding organs; and the clinical manifestations are not significantly different from those of other gastrointestinal tumors. We here report a case of an adolescent with CCSLGT who developed multiple metastases in mesenteric lymph nodes,liver, lung, bone, left inner thigh, pleura, mediastinum, hilar lymph nodes, and adrenal gland after surgery, and had a poor prognosis with survival of no more than 5 years despite aggressive antitumor therapy. As far as we know, there are few reports in the English-language literature of multiple metastases in adolescent patients with CCSLGT after extensive resection. Clinicians should consider its highly invasive biological behavior and follow-up closely with whole-body imaging.
CASE PRESENTATlON
Chief complaints
A 16-year-old man had dizziness and fatigue without obvious cause 2 mo ago. After strenuous exercise 15 d ago, dizziness was aggravated, with nausea and tinnitus.
2.3.3 剪切波弹性成像(shear wave elastic imaging,SWEI)剪切波弹性成像是基于剪切波速度的测量,通过检测声辐射力激发组织而产生的剪切波的传播进行成像的方法,直接测量的是剪切波速度本身,通过公式计算出目标组织的杨氏模量。它可分为瞬时弹性成像 (TE)、单点剪切波成像(qSWE)、 多 维剪切 波 E 成像 (2D-SWE、3DSWE)。SWE可以有效地避免人为因素的影响,在不施加外力的情况下,通过测量目标组织的剪切波速度来判断组织的硬度[7]。
History of present illness
Laboratory test results at a local hospital showed neutrophils (6.35 × 10
/L, normal level 1.80 × 10
-6.30× 10
/L), erythrocytes (3.91 × 10
/L, normal level 4.80 × 10
-5.80 × 10
/L), platelets (486 × 10
/L,normal level 100 × 10
-300 × 10
/L), high sensitivity C-reactive protein (188.0 mg/L, normal level 0.5-10 mg/L), fecal occult blood test positive, and gastroscopy suggested erosive gastritis. No obvious abnormality was found on colonoscopy. The patient was diagnosed with gastrointestinal bleeding and hemorrhagic anemia. The patient presented with tolerable paroxysmal epigastric pain 10 d prior to hospital visit, but the abdominal pain worsened progressively when eating 10 h previously, and he came to our hospital for medical treatment. He had normal spirit and appetite, poor sleep, and normal defecation and urination, and a weight loss of 3 kg.
History of past illness
The patient was in good health.
Personal and family history
Laboratory test results showed elevated fibrinogen (5.72 g/L, normal level 2-4 g/L), but no obvious abnormality was found in tumor markers.
Physical examination
On admission, he had pressure pain in the wall of the upper abdomen, and no rebound tenderness,bowel sounds at 8 beats/min.
该系统提供了强大的系统报警功能。在基于以上诊断识别出异常信息时,该系统中会产生详细的报警信息,同时根据事先设定好的接收人员,自动将报警以短信形式推送至相关人员手机,操作人员可以通过派单形式下发至巡检人员进行现场巡检,自动记录巡检内容。
Laboratory examinations
The patient had no family history of hereditary diseases.
展览共分六个部分。开篇视频《伟大的变革》,再现改革开放大事要事喜事的《壮美篇章》,聚焦重大时间节点、重大历史事件、重大决策部署的《关键抉择—党中央推进改革开放的战略擘画》,全方位展示巨大成就的《历史巨变》,改革成果惠及百姓的《大国气象》,结语《面向未来》。
Imaging examinations
Abdominal digital radiography did not show any dilated loop of bowel to suggest bowel obstruction(Figure 1). Further contrast-enhanced computed tomography (CT) of the abdomen and pelvis showed obvious localized thickening of the ileal wall in the right lower abdomen, with soft tissue density mass,involving the intestinal wall with a length of approximately 4.1 cm, plain scan CT value of approximately 59 HU (Figure 2A), arterial phase CT value of approximately 78 HU (Figure 2B) and venous phase CT value of approximately 97 cm (Figure 2C), showing moderate uniform progressive enhancement. Multiplanar reformation (MPR) images showed that the mass in the intestinal wall grew inwards. The thickness of the mass was approximately 2.4 cm, and resulted in luminal narrowing.Several enlarged lymph nodes could be seen at the root of the mesentery, and the largest was approximately 2.8 cm in diameter (Figure 2D).
FlNAL DlAGNOSlS
Combined with pathological morphology, immunohistochemistry and gene detection, the tumor was diagnosed as CCSLGT.
TREATMENT
The patient underwent resection of the small intestinal masses. During the operation, a solid and hard protuberant tumor was located in the ileum approximately 15 cm from the ileocecal part. The tumor of about 5 cm × 3.5 cm × 2 cm invaded the whole layer of the intestine; did not invade the surrounding organs; enlarged lymph nodes were seen at the root of the mesentery, with a size about 2 cm × 1 cm;dark red content could be seen in the distal intestine, and old bleeding was considered; and no abnormality was found in the liver and pelvis. The tumor and part of the small intestine were removed at 5 cm from both ends of the lesion, and the mesenteric and perienteric fat lymph nodes were dissected.The postoperative specimens were sent for pathological examination. Under light microscopy, the tumor cells were diffusely arranged and separated by a slender fibrous septum (Figure 3A). Immunohistochemical detection: AE1/AE3 (-), CK7 (focal ±), Smur100 (+) (Figure 3B), MelanA (-), HIB45 (-), CD34(vascular +) (Figure 3C), CD117 (-), Dog-1 (-), CDX-2 (-), Villin (-), CK8/18 (-), LCA (-), CD10 (-), TFE-3(-), SMA (-), desmin (-), MyoD1 (pulp ±), myogenin (pulp ±), NSE (pulp ±), Ki-67 (30% +) (Figure 3D).Fluorescence
hybridization (FISH) detected 100 tumor cells, and the number of positive cells for fluorescent labeling was 46%. Reverse transcription polymerase chain reaction regarding
/
was positive to confirm our FISH experiment. According to the interpretation criteria, this case had
gene breakage (Figure 3E).
OUTCOME AND FOLLOW-UP
The patient was followed up regularly without adjuvant treatment. After 13 mo, he stopped defecation and flatulence and came to our hospital because of intermittent severe abdominal pain. CT examination showed multiple enlarged lymph nodes at the root of the mesentery (Figure 4A). Clinicians considered metastasis and carried out abdominal exploration. Tumors of 6.0 cm × 4.0 cm × 3.0 cm and 1.5 cm × 1.0 cm × 0.5 cm were found at the root of the retroperitoneal small intestine.
The authors declare that they have no competing interests.
At 35 mo after the operation, the patient found a mass on the inside of the left thigh, with hard texture, poor range of motion, traction-like pain in the left thigh, and tension in the posterior lumbar muscles with fluctuating pain, passive posture and limited activity, which lasted for 1 h. The symptoms gradually worsened. Magnetic resonance imaging (MRI) of lumbar vertebrae showed low signal intensity in T12, L1 and L3 vertebrae, slightly high signal intensity in T2-weighted imaging, and high signal intensity in L3 vertebrae on turbo inversion recovery magnitude fat pressing sequence(Figure 4D).



Contrast-enhanced US showed multiple areas of solid inhomogeneous hypoechogenicity adjacent to the superior mesenteric artery with clear boundaries. The larger areas were about 3.6 cm × 2.9 cm, and the enhancement was slow and uneven. Solid inhomogeneous areas of hypoechogenicity of 1.3 cm × 1.2 cm and 2.2 cm × 1.9 cm were seen under the capsule of the right anterior lobe and posterior lobe of the liver, respectively. The boundary was unclear, the arterial phase showed circular enhancement, and the enhancement in the portal vein and delayed phases decreased. Ultrasound-guided lymph node biopsy and radiofrequency ablation of enlarged lymph nodes adjacent to the superior mesenteric artery and radiofrequency ablation of liver space were performed. Postoperative pathology combined with medical history and immunohistochemistry were consistent with CCSLGT superior mesenteric artery paramesenteric lymph node metastasis.
After surgical resection, the specimens were sent for pathological examination, combined with medical history and immunohistochemistry in accordance with CCSLGT mesenteric lymph node metastasis. Ultrasonography (US) 27 mo after the operation showed that the intrahepatic echo was hyperechoic (Figure 4B), and the internal echo was inhomogeneous, with a size of about 1.4 cm × 1.2 cm.There was no obvious blood flow signal on color Doppler flow imaging. Ultrasound-guided percutaneous hepatic space-occupying biopsy and radiofrequency ablation were performed, and the left lobe nodules were ablated with hyperechoic coverage. The postoperative specimens were sent for pathological examination, which was consistent with CCSLGT liver metastasis. CT examination at 32 mo after the operation showed multiple solid and well-defined nodules in both lungs, and a patchy and nodular low-density mass in the liver, with unclear boundary, contrast enhancement in the ring but no obvious enhancement in the center (Figure 4C). The enlarged lymph nodes at the root of the mesentery were enlarged and increased compared with before.
Whole-body
Tc-methylene diphosphonate bone scintigraphy showed increased radiotracer uptake in L3 vertebral body (Figure 5), and bone metastasis was considered. The patient was treated regularly with intensity-modulated radiotherapy. CT showed more lesions in the liver, unclear cystic-solid, lowdensity, space-occupying lesion on the inner side of the left thigh, and uneven circular enhancement(Figure 4E). The maximum dimension was about 3.3 cm × 2.9 cm. Ultrasound-guided puncture biopsy and radiofrequency ablation of the mass in the medial thigh and radiofrequency ablation of the liver were performed. Postoperative pathology combined with morphology, immunohistochemistry and previous medical history were consistent with CCSLGT medial metastasis of the left thigh.
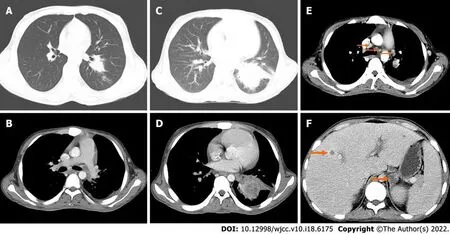
Thirty-nine months after the operation, the patient came to our hospital with recurrent fever, cough and expectoration for > 1 mo. The body temperature fluctuated from 38.0 to 39.5 °C. CT examination showed more multiple small nodules in both lungs than before (Figure 4F).
Forty-three months after the operation, pelvic MRI showed multiple diffuse restricted high signals in the bilateral inguinal area and adjacent iliac vessels, with mild MRI enhancement (Figure 4G). Reexamination by CT showed that the nodule of the left lower lobe was significantly enlarged and the boundary was unclear (Figure 6A). The size of the nodule was 2.5 cm × 3.5 cm, with mild inhomogeneous enhancement, and the left pleural soft tissue nodule showed enhancement (Figure 6B). Bilateral inguinal lymph nodes were enlarged and there was a small amount of fluid density in bilateral pleura and pericardium.

CT examination at 50 mo after the operation showed an irregular mass in the lower lobe of the left lung, which was significantly larger in size than before (Figure 6C) and moderate enhancement(Figure 6D). Other nodules in both lungs were enlarged and increased in number, with multiple mediastinal, left hilar, and axillary lymphadenopathy (Figure 6E). Soft tissue nodules in the left pleura were enlarged, low-density soft tissue masses were seen in the left adrenal gland with a diameter of approximately 2.3 cm, and the boundary was unclear, moderately reinforced in a circular pattern(Figure 6F), with small pleural and pericardial effusion.
The imaging findings of CCSLGT have rarely been reported. CT examination of our patient showed that the peripheral wall of the intestinal canal in the distal part of the right lower abdominal ileum was localized and thickened, the density was uniform, and no calcification or cystic necrosis was found.After MPR, the tumor showed strong invasive growth into the intestine, a clear boundary, obvious narrowing of the intestinal cavity and moderate progressive enhancement, which was different from that of traditional sarcomas. It may be associated with the presence of mucoid stroma in the tumor pathological tissue, which makes the contrast medium enter the tumor tissue slowly. Pathologically, the tumor invaded the whole layer of the intestinal wall, and the peri-intestinal fat was clear on CT images,and no invasion was found.
Research on developmental and motional characteristics of Daaoxi unstable rock along
DlSCUSSlON
The most common clinical manifestations of CCSLGT are abdominal pain, intestinal obstruction,accompanied by varying degrees of anemia, nausea, vomiting, weight loss and fatigue[2-4]. This patient was in good health, had no family history of tumors, and the symptoms were atypical at the beginning,because the primary tumor of the small intestine was rare. After an occult blood test was positive, the patient was examined by gastroscopy and colonoscopy, but not by enteroscopy. He was diagnosed with erosive gastritis with gastrointestinal bleeding, no small intestinal lesions were found, and antitumor treatment was delayed. Later, the patient developed paroxysmal epigastric pain, stopped flatulence and defecation, and no intestinal obstruction was found by digital radiography. Further CT enhancement found a space-occupying soft tissue mass in the ileum. Therefore, patients with gastrointestinal symptoms should be examined by CT, which is beneficial for the detection of lesions in other parts of the body. The median diameter of CCSLGT is 45 mm, ranging from 15 mm to 135 mm. In general, it is multinodular and can be accompanied by hemorrhage, necrosis or cystic changes[4]. The present case was consistent with reports in the literature.

Histologically, tumor cells infiltrate between the walls of the gastrointestinal tract, often into the mucous membrane and serous layer, forming mucosal ulcers. CCSLGT consists of medium-sized tumor cells arranged in flaky or irregular nest-like structures separated by a slender fibrous diaphragm,pseudopapillary, pseudoglandular and pseudochrysanthemum-shaped structures and myxoid stroma,and occasionally pseudoangioma-like structures. Osteoclast-like multinucleated giant cells are scattered in approximately 50% of the cases[5-7]. Mitotic activity is significantly active in these tumors,accompanied by typical focal necrosis[8]. Stockman
[7] reviewed and analyzed 16 cases of CCSLGT,and found that the tumor showed neurodifferentiation potential and expressed neuroendocrine markers, indicating that gastrointestinal CCS originated from neuroectodermal precursor cells and may have lost the ability of melanocyte differentiation. Therefore, a new name was proposed, malignant gastrointestinal neuroectodermal tumor.
At 56 mo after the operation, the patient died of multiple metastases of CCSLGT.
CCSLGT in the small intestine should be differentiated from small intestinal stromal tumor, small intestinal adenocarcinoma and small intestinal lymphoma. Small intestinal stromal tumors often occur in the jejunum, with characteristic expression of CD117. CT shows irregular or circular thickening of the intestinal wall, or manifested as a round or lobulated mass protruding from the intestinal lumen. The enhanced mass or thickened intestinal wall showed mild to moderate enhancement. CT of small intestinal adenocarcinoma shows irregular or circular thickening of the intestinal wall, irregular mucous membrane, or localized soft tissue masses protruding into the intestinal lumen, and mild to moderate enhancement of the mass or thickened intestinal wall. Most small intestinal lymphomas show diffuse uniform thickening of the intestinal wall, the involved intestinal segment is long and some of them show single or multiple polypoid masses protruding into the intestinal cavity, and most of them show mild to moderate homogeneous enhancement.
CCSLGT has highly invasive biological behavior, and local recurrence and distant metastasis readily occur in the later stage. Regional lymph nodes, lungs, bones and liver are the main sites of metastasis[9]. Currently, there is no effective treatment, and the main treatment is surgical resection. Even after treatment, CCSLGT usually relapses in a wide range of metastatic nodules and visceral diseases[10].After extensive surgical resection, metastasis of mesenteric lymph nodes, liver, lung, bone, medial left thigh, pleura, mediastinum, hilar lymph nodes and adrenal gland gradually appeared in the present patient, indicating that CCSLGT metastasizes through lymph nodes and blood. Although our patient received active antitumor therapy, the survival time was < 5 years and his prognosis was poor.Disappointingly, conventional adriamycin-based chemotherapy for other non-small round cell soft tissue sarcomas is ineffective, and there is no report that postoperative radiotherapy and chemotherapy are helpful; therefore, larger prospective studies are needed to determine the best treatment options[11]. Although there are currently no effective treatments for this highly aggressive tumor, future targeted therapies that inhibit the function of the
-
fusion oncogene or its associated downstream pathways may be effective in treating the disease. CT can accurately locate CCSLGT and provide the characteristics of lesion size, shape, internal structure and growth. It is of value in observing invasion of adjacent tissues and organs and lymph nodes, and distant metastasis. Positron emission tomography/CT is recommended for patients with CCSLGT, which can provide functional metabolic information beyond anatomical images and effectively reduce missed lesions.
CONCLUSlON
In summary, Whole abdominal CT enhancement is recommended for patients with gastrointestinal symptoms. CCSLGT is a rare malignant mesenchymal tumor with unique morphological, there is no effective treatment for CCSLGT with systemic multiple metastases
the lymphatic system and bloodstream after surgical resection. immunophenotypic and molecular genetic characteristics. The clinical manifestations are not specific, and the diagnosis depends on immunohistochemistry and gene detection. Currently, there is no effective treatment. Clinicians should consider its highly aggressive biological behavior, follow it closely, and recommend regular postoperative whole-body imaging to reduce missed lesions. The diagnosis of this young patient with CCSLGT was clear. After active antitumor treatment, the metastatic focus
is still progressing, the survival time is short, and the prognosis is poor.
FOOTNOTES
《造纸信息》以为造纸企事业单位及相关行业提供国内外造纸工业信息服务为主要宗旨,汇集行业专家观点、聚焦行业热点问题、展示领军企业风采,及时报道行业政策、企业动态、新技术和新成果,以及全球造纸企业的最新动向,为读者全方位了解造纸行业提供独家参考,为企业提供政策性指导和经营决策信息。
江苏是一个经济大省,又是一个水利大省。江苏的经济社会现代化发展,不仅需要水利提供更高标准的防洪安全保障,还需要提高水资源和水生态环境的基础支撑,以水利的现代化支撑和保障经济社会的现代化发展。
The study was approved by the Institutional Review Board at The First Affiliated Hospital of Zhengzhou University. Participant gave written consent to participate in the study.
1.2.1 汽轮机模型 汽轮发电机模型包括同步机、汽轮机、交流励磁机、热工调速器和多质量扭转轴接口.主要技术参数见表1[7].
Huang WP acquired and analysed of the work, drafted the manuscript, imaging data collection and analysis; Li LM edited the manuscript; Gao JB wrote and reviewed and edited the manuscript; all authors met the requirements for authorship for the submitted version and agreed to its submission.
“文化生态建设必须考虑运用制度的制约来确保有限的资源能够充分地利用”[18]。欲建立和完善福建武术文化生态制度,就要从决策、评价、考核和监管等几方面同时发力,加快实践探索和理论创新,健全指标的评价体系,建立资源的有偿使用和保护制度,真正以制度建设推动文化生态建设。但需明确,文化生态制度建设并非朝夕之功,它要长期地向大众传送文化生态理念,强化文化生态意识,通过大力宣传和教育让文化生态价值观成为社会主流价值观,让建设文化生态成为人们日常生活中的行动指南,着实提高和改善福建武术文化生态建设的“硬环境”。
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Wen-Peng Huang 0000-0002-9104-1494; Li-Ming Li 0000-0002-2910-9742; Jian-Bo Gao 0000-0003-2621-3701.
Ma YJ
(2)给矿粒度、筛网磨损与能耗之间关系。增大破碎粒度尺寸,筛网损耗和皮带的负荷就相应的增加;反之,二者均会降低。根据实际需求调节合适的给矿粒度有利于物耗能耗的最大化。
在实验前,要求学生做好分工,每组6位同学,组内6位同学分别完成实验1~6中的某一个实验(课前分好工,防止课上小组分工不协调,耽误时间),其他同学协助,并仔细记录实验现象。这样,不仅锻炼了每位学生的动手能力,也充分体现了小组协作、互助。实验完成后,组内成员一起挖掘现象背后的本质原因,培养学生宏观辨识与微观探析共同发展的化学核心素养。
A
Ma YJ
1 Taminelli L, Zaman K, Gengler C, Peloponissios N, Bouzourene H, Coindre JM, Hostein I, Guillou L. Primary clear cell sarcoma of the ileum: an uncommon and misleading site.
2005 ; 447 : 772 -777 [PMID: 16021514 DOI:10 .1007 /s00428 -005 -0019 -y]
2 Huang W, Zhang X, Li D, Chen J, Meng K, Wang Y, Lu Z, Zhou X. Osteoclast-rich tumor of the gastrointestinal tract with features resembling those of clear cell sarcoma of soft parts.
2006 ; 448 : 200 -203 [PMID: 16220298 DOI:10 .1007 /s00428 -005 -0051 -y]
3 Zambrano E, Reyes-Mugica M, Franchi A, Rosai J. An osteoclast-rich tumor of the gastrointestinal tract with features resembling clear cell sarcoma of soft parts: reports of 6 cases of a GIST simulator. Int J Surg Pathol 2003 ; 11 : 75 -81[PMID: 12754623 DOI: 10 .1177 /106689690301100202 ]
4 Green C, Spagnolo DV, Robbins PD, Fermoyle S, Wong DD. Clear cell sarcoma of the gastrointestinal tract and malignant gastrointestinal neuroectodermal tumour: distinct or related entities?
2018 ; 50 : 490 -498 [PMID: 29970252 DOI:10 .1016 /j.pathol.2018 .05 .001 ]
5 Askan G, Kombak FE, Seven IE, Basturk O. Clear Cell Sarcoma-Like Tumor of the Gastrointestinal Tract.
2019 ; 50 : 651 -656 [PMID: 29623567 DOI: 10 .1007 /s12029 -018 -0069 -4 ]
6 Wang J, Thway K. Clear cell sarcoma-like tumor of the gastrointestinal tract: an evolving entity.
2015 ; 139 : 407 -412 [PMID: 25724038 DOI: 10 .5858 /arpa.2013 -0547 -RS]
7 Stockman DL, Miettinen M, Suster S, Spagnolo D, Dominguez-Malagon H, Hornick JL, Adsay V, Chou PM, Amanuel B,Vantuinen P, Zambrano EV. Malignant gastrointestinal neuroectodermal tumor: clinicopathologic, immunohistochemical,ultrastructural, and molecular analysis of 16 cases with a reappraisal of clear cell sarcoma-like tumors of the gastrointestinal tract.
2012 ; 36 : 857 -868 [PMID: 22592145 DOI: 10 .1097 /PAS.0 b013 e31824644 ac]
8 Gahanbani Ardakani A, Boyle DJ, Elton C. Gastrointestinal clear cell sarcoma-like tumour of the ascending colon.
2016 ; 98 : e37 -e39 [PMID: 26890846 DOI: 10 .1308 /rcsann.2016 .0073 ]
9 Hisaoka M, Ishida T, Kuo TT, Matsuyama A, Imamura T, Nishida K, Kuroda H, Inayama Y, Oshiro H, Kobayashi H,Nakajima T, Fukuda T, Ae K, Hashimoto H. Clear cell sarcoma of soft tissue: a clinicopathologic, immunohistochemical,and molecular analysis of 33 cases. Am J Surg Pathol 2008 ; 32 : 452 -460 [PMID: 18300804 DOI:10 .1097 /PAS.0 b013 e31814 b18 fb]
10 Thway K, Judson I, Fisher C. Clear cell sarcoma-like tumor of the gastrointestinal tract, presenting as a second malignancy after childhood hepatoblastoma.
2014 ; 2014 : 984369 [PMID: 24715928 DOI: 10 .1155 /2014 /984369 ]
11 Kawai A, Hosono A, Nakayama R, Matsumine A, Matsumoto S, Ueda T, Tsuchiya H, Beppu Y, Morioka H, Yabe H;Japanese Musculoskeletal Oncology Group. Clear cell sarcoma of tendons and aponeuroses: a study of 75 patients.
2007 ; 109 : 109 -116 [PMID: 17133413 DOI: 10 .1002 /cncr.22380 ]
猜你喜欢
杂志排行

World Journal of Clinical Cases的其它文章
- Diabetes mellitus susceptibility with varied diseased phenotypes and its comparison with phenome interactome networks
- Sequential chemotherapy and icotinib as first-line treatment for advanced epidermal growth factor receptor-mutated non-small cell lung cancer
- Impact of preoperative carbohydrate loading on gastric volume in patients with type 2 diabetes
- Disseminated strongyloidiasis in a patient with rheumatoid arthritis: A case report
- CYP27A1 mutation in a case of cerebrotendinous xanthomatosis: A case report
- Efficacy and safety of adalimumab in comparison to infliximab for Crohn's disease: A systematic review and meta-analysis