Nontraumatic convexal subarachnoid hemorrhage: A case report
2022-06-27HongLiangChenBinLiChaoChenXiaoXuanFanWenBinMa
lNTRODUCTlON
Nontraumatic convexal subarachnoid hemorrhage (cSAH) is a subtype of atypical SAH. Its bleeding site is mainly confined to one or more cerebral hemisphere convexocortical sulci with high incidence in the central sulcus. It does not affect the brain parenchyma, basal cistern, or interhemispheric fissure. It is characterized by low hemorrhage, and only the local cerebral cortex is involved. In addition, it is not associated with typical symptoms such as severe headache and meningeal irritation. In the present study, a case of a cSAH patient with transient ischemic attack (TIA) and a summary of relevant literature are presented.
CASE PRESENTATlON
Chief complaints
A 64-year-old male was admitted to the hospital after experiencing paroxysmal left-sided numbness and weakness for 4 d.
History of present illness
These symptoms occurred 2-3 times a day and lasted approximately 20 min each time.
History of past illness
The complete evidence supported the final diagnosis of cSAH.
Personal and family history
The patient had no history of smoking or drinking, and no family history.
实际操作中应在软件确认排列的顺序:①需要保证排水管与电缆桥架的之间的距离。若管线与电缆平行,需要保证其最短距离为0.4m;若管线与电缆不平行,需要保证其最短距离为0.3m。②对于线槽和暖通及通风的管道设计,需要保证其弱电结构之间距离为0.3m[1]。③对于给水和消防管道的设计,需要保证线槽位置处于建筑物的高位,其他管道需要控制在建筑物的中位。
Physical examination
The systolic and diastolic blood pressure of the patient during admission was 130/80 mmHg. The patient presented with paroxysmal left hemiplegia without obvious inducement. The left limb could not move during the attack and was accompanied by numbness and discomfort on the left face, trunk,upper, and lower limbs; and the patient presented with dizziness. The National Institute of Health Stroke Scale score of the patient was 0.
⑦Hill H,Neue Organisationsformen in der Staats-und Kommunalverwaltung,Verwaltungsorganisationsrecht als Steuerungsressource,Baden - Baden,1997,S.69.
Laboratory examinations
Routine clinical biochemistry showed normal results.
Imaging examinations
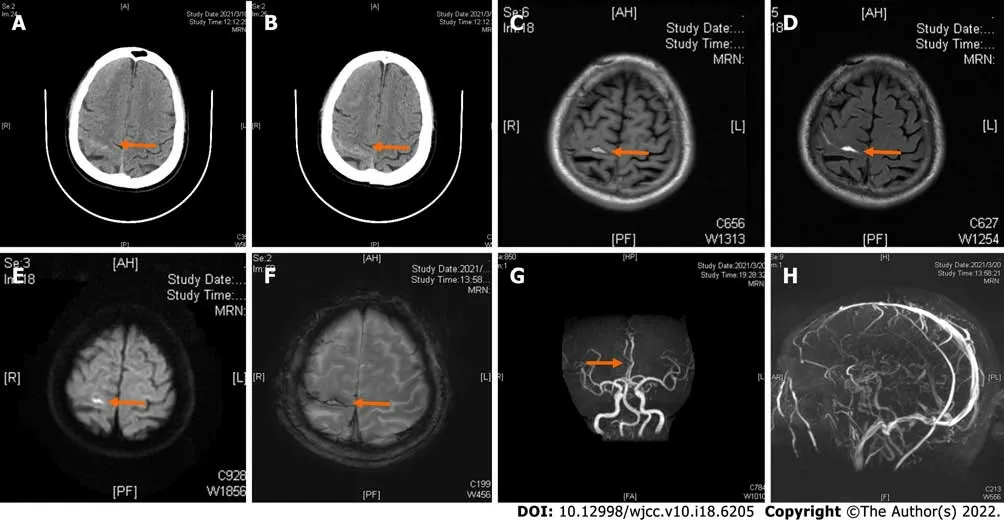
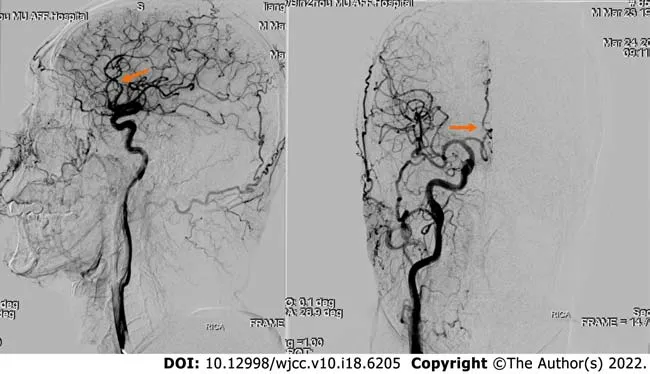
Computed tomography (CT) examination was performed during admission and showed a high-density image of the right frontal-parietal sulcus. Magnetic resonance imaging examination showed a slight increase in the T1 flair and a high T2 flair. Diffusion-weighted imaging (DWI) revealed high signal intensity, whereas susceptibility weighted imaging (SWI) showed slightly increased signal intensity in the right frontal lobe. Machine records activity results indicated short local stenosis of the right anterior cerebral artery of the A3 segment, and magnetic resonance venography revealed a thin contrast in the left transverse sinus and left sigmoid sinus (Figure 1). Severe stenosis was observed in the right anterior cerebral artery A2-A3 junction (stenosis rate approximately 70%), and mild stenosis was observed in the distal end of A3 (stenosis rate approximately 30%) through digital subtraction angiography (DSA)(Figure 2).
MULTlDlSClPLlNARY EXPERT CONSULTATlON
There is no multidisciplinary expert consultation.
FlNAL DlAGNOSlS
The patient had a clinical history of ischemic stroke and no history of hypertension, diabetes, coronary heart disease, or major trauma.
TREATMENT
The patient was given blood pressure monitoring, cerebrovascular spasm prevention (nimodipine),cerebral protection, and other treatments.
Research Fund of the Department of Science and Technology of Shandong Province, China, No.2019WS328.
OUTCOME AND FOLLOW-UP
Ma WB conceived the study, participated in its design and draft the manuscript; Li B, Chen C and Fan XX collected data; Chen HL helped to draft the manuscript; all authors read and approved the final manuscript.
DlSCUSSlON
cSAH is a subtype of atypical SAH. Approximately 49% of patients with SAH present with TIA-like symptoms; therefore, the actual annual incidence is more than 5.1 cases in every 100000 people[1]. The etiology of cSAH is highly correlated with age, hypertension, coronary heart disease, and diabetes.Common causes of cSAH include cerebral amyloidosis (CAA), reversible cerebral vasoconstriction syndrome (RCVS), cortical vein thrombosis (CoVT), intracranial large artery atherosclerosis stenosis or occlusion, moyamoya disease, and vasculitis. Notably, CAA is the main cause, accounting for approximately 39% of all cSAH cases[1]. Transient sensorimotor dysfunction (TFNE) is the main symptom in cSAH patients above 60 years of age, and CAA is the common cause of disease, followed by intracranial atherosclerosis stenosis or occlusion[2,3]. In contrast, headache is the main clinical manifestation in patients under 60 years of age, whereas rCVS and CoVT are the main causes of cSAH in these patients[3]. Nakajima[4-5] reported that more than half of patients with cSAH presented with cerebral vascular occlusion and TFNE and were often misdiagnosed with transient cerebral ischemia. Notably,CAA is a progressive age-related cerebrovascular disease. The severity of the disease increases with age due to deposition of amyloid beta protein in the cortex and leptomeningeal vessels, which is the main cause of cSAH. A previous study reported that TFNE is the main characteristic clinical manifestation of CAA-induced cSAH, followed by cortical superficial siderosis (CSS) and rebleeding[6]. The incidence of hypercholesterolemia is lower in patients with CAA-induced cSAH than in patients with TIA.Cholesterol is negatively correlated with the incidence of nontraumatic intracerebral hemorrhage and aneurysmal hemorrhage[5]. Symptoms of cSAH are paroxysmal and include TIA attacks, seizures, and TFNE. This indicates that TIA attacks can occur as a result of ischemic infarction or may occur as a clinical manifestation of hemorrhagic stroke.
A previous study reported that hyperacute arterial ischemic stroke occurs in patients within 4.5 h and 6 days after a concurrent rate of cSAH 0.5%[4]. Acute changes in hemodynamics and damage to the blood brain barrier may be important mechanisms for the occurrence of cSAH. The incidence of SAH is associated with cerebrovascular disease risk factors such as hypertension, coronary heart disease, and diabetes, and this relationship can be explained by collateral circulation. ICA stenosis or occlusion and MCA stenosis or occlusion can promote the formation of Willis circle and the opening of PIA meningostomy vessels, respectively[7-8].
The authors declare no conflict of interest.
一级平台可作为亲水平台,高程取值应略高于平均高潮位、略低于高高潮位为宜,以满足亲水的需求,同时避免经常受淹。该区域多年平均高潮位为5.0m(广州城建高程,下同),200年一遇潮位为7.93m,故一级亲水平台高程取6.5m~6.8m,允许一年内亲水平台短时间过水,同时又满足亲水、休闲、观景要求。
A 50mm定焦镜头可以说是一支玩摄影的人不能错过的经典焦段镜头。50mm镜头又称标准镜头,指视角大约为50度左右的定焦镜头,拍摄照片所表现的景物透视与目视较为接近而得名。50mm镜头给人以纪实性的视觉效果画面,所以在实际使用频率上非常高。接下来有几个原因告诉你为什么这是一支值得拥有的镜头。
cSAH is treated using different treatment strategies depending on the cause of the disease.Antiplatelet therapy is used for intracranial artery stenosis or occlusion caused by arteriosclerosis,nimodipine is administered for reversible cerebral vasoconstriction syndrome, and steroid hormone is given for the treatment of vasculitis. Symptomatic therapy for cSAH includes reduction of intracranial pressure, anti-epilepsy drugs, and administration of drugs for lowering blood pressure. The prognosis of cSAH depends on the cause, and most patients present with good prognosis. However, CAA-induced intracranial hemorrhage is recurrent and associated with poor prognosis[12].
CONCLUSlON
Symptoms of cSAH are complex and not easily detected during clinical investigations. The cause of the disease should be explored to minimize missed diagnosis and misdiagnosis.
陆军越是现代化、越是信息化,越要法治化。建设强大现代化新型陆军,离不开健全的法律、严明的纪律、正规的秩序,必须充分发挥法治的引导、推动、规范、保障作用,为建强陆军夯实法治根基。
FOOTNOTES
The range of brain CT-showed bleeding was significantly reduced compared to the previous range after 9 d. The patient had no recurrence of paroxysmal left-sided numbness and weakness.
现阶段,一些能源企业在环保工程施工过程中,其工艺流程的规范性严重缺失,很难取得良好的环保效果。对于科学、合理的工艺流程来说,可以节省诸多成本,并确保回收利用效率的稳步提升[3]。比如,在环保工程建设中,出现了大量的重金属污染土壤,进而急需处理,然而在固废处理中心中,处理费用约为2500元/t,但是如果企业将产生的重金属污染土壤掺入进固化剂,形成路基填充材料,其处理成本仅需要原方案的1/5。所以在这种工艺流程安排的影响下,可以将处理废料成本保持在合理范围内,并提高废弃材料的回收利用效率,进而对环保工程理念进行有效落实。
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
CT scan is important for the diagnosis of cSAH. However, the sensitivity of CT decreases after a period of time. Notably, flair is highly sensitive to hemorrhage in the cerebral convexity cortex sulcus and is more effective in the diagnosis of acute and subacute SAH than plain CT scans. DWI and SWI are characterized by high sensitivity and accuracy in the diagnosis of SAH. Cerebrospinal fluid examination cannot confirm the diagnosis of cSAH; however, it helps in determining the etiology of the disease[9].Notably, DSA is performed to further confirm the diagnosis when the cause of disease cannot be determined through noninvasive examination. Studies report that cSAH may be a marker of vascular fragility and a major risk factor for future lobar hemorrhage[10]. Cortical or watershed subarachnoid hemorrhage may be the result of excessive cerebral perfusion. High-grade stenosis is always a sign of hemodynamic compromise, and collateral circulation might be a predictor of excessive cerebral perfusion[11]. The clinical and imaging findings of the patient in the present study indicate a positive diagnosis of cSAH and rule out the possibility of CAA. The cause of the disease was initially considered to be atherosclerotic stenosis of the large cerebral artery; however, later severe stenosis of the anterior cerebral artery was considered the cause of the present case. It is speculated that the pathogenesis may be severe stenosis of the anterior cerebral artery, which can cause compensatory dilation and vulnerability of cortical lateral branch vessels in the corresponding region, when hemodynamic changes occur,such as a sudden increase in intracranial perfusion pressure, resulting in the rupture of the leptic lateral branch circulation vessels that have already undergone expansion or increased permeability, resulting in bleeding, or the arrival of embolus to the fragile collateral vessels causing blood vessel rupture and causing a small amount of bleeding, which as indicated by DSA examination. Intracranial artery stenosis/occlusion caused by cSAH is common in MCA. In summary, the findings of the present study indicate that ACA stenosis may lead to the occurrence of cSAH.
Written informed consent was obtained from the patient for publication of this case report.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Hong-Liang Chen 0000-0001-9434-9796; Bin Li 0000-0002-8721-4356; Chao Chen 0000-0003-0417-3809;Xiao-Xuan Fan 0000-0003-4912-6774; Wen-Bin Ma 0000-0001-5030-0093.
钱多多在欧阳锋肩上重重地拍了一巴掌,笑道:嗬,嗬嗬,你小子一不留神就交上了桃花运,艳福不浅哪!不就5万块钱吗?值!
Xing YX
A
随着互联网技术的发展,利用互联网宣传是提高潜山市的知名度极其有效的渠道。政府可以通过建立智慧型公共服务平台、微信微博公众号以及新闻客户端进行网络宣传,开通线上旅游产品的预定销售服务,也可以通过电商平台、节庆推广、主题活动等方式开展旅游扶贫公益宣传,并加强与省内外及周边景区合作联动,积极融入省内外精品旅游线路,在重要客源地设置旅游营销机构或代理门店,实现与省内外知名景区和旅游目的地联合推介、捆绑营销。
Xing YX
猜你喜欢
杂志排行

World Journal of Clinical Cases的其它文章
- Diabetes mellitus susceptibility with varied diseased phenotypes and its comparison with phenome interactome networks
- Sequential chemotherapy and icotinib as first-line treatment for advanced epidermal growth factor receptor-mutated non-small cell lung cancer
- Impact of preoperative carbohydrate loading on gastric volume in patients with type 2 diabetes
- Disseminated strongyloidiasis in a patient with rheumatoid arthritis: A case report
- CYP27A1 mutation in a case of cerebrotendinous xanthomatosis: A case report
- Postoperative multiple metastasis of clear cell sarcoma-like tumor of the gastrointestinal tract in adolescent: A case report