Clinical efficacy of Tuina manipulations for lumbar disc herniation and its influence on posture-associated indicators
2022-06-23SHENTao申韬YEYong叶勇FANSheng范升LUORong罗容PANJiang潘江TANGWei汤伟
SHEN Tao (申韬), YE Yong (叶勇), FAN Sheng (范升), LUO Rong (罗容), PAN Jiang (潘江), TANG Wei (汤伟)
1 Hunan University of Chinese Medicine, Changsha 410208, China
2 The First Hospital of Hunan University of Chinese Medicine, Changsha 410007, China
Abstract
Keywords: Tuina; Massage; Intervertebral Disc Displacement; Low Back Pain; Pain Measurement; Visual Analog Scale;Posterior Muscle Chain
Lumbar disc herniation (LDH) is a common degenerative vertebral disease and a significant cause of low back pain[1-2]. Chinese LDH expert consensus or guide holds that conservative treatments can help improve clinical symptoms in most LDH patients[3-5], and the success rate of non-surgical treatments reaches 80%-90%[6-7]. Therefore, conservative treatments are currently the leading way to mitigate LDH symptoms[8-9].
Tuina (Chinese therapeutic massage) manipulation owns high repeatability and safety and is easy to operate. Numerous studies from China and abroad have proved its effectiveness in reducing LDH symptoms[10-11].Sinew-bone balance is the physiologic state of the spine[12], and sinew-bone imbalance is a pathologic state of the spine and an essential pathogenic factor in causing vertebral diseases. Further, as a significant concept in LDH treatment, sinew-bone balancing represents the theory of concurrent treatment of bones and tendons in traditional Chinese medicine (TCM) and can help patients to achieve an ideal state of fit bones and flexible tendons. Our previous clinical findings have testified to the effectiveness of sinew-bone balancing manipulation in treating spine-related diseases[13-15].The present study aims to provide clinical evidence for the concept of laying equal emphasis on sinews and bones by observing the clinical efficacy of the sinewbone balancing manipulation in treating LDH.
1 Clinical Materials
1.1 Diagnostic criteria
Referred to the diagnostic criteria in theChina Pain Expert Consensus on the Diagnosis and Treatment of Lumbar Disc Herniation[16]: presented typical symptoms and signs, e.g., low back pain, radiating pain in the lower limb, positive for straight leg raising test, etc.; LDH confirmed by X-ray, CT, or MRI examinations.
1.2 Inclusion criteria
Conformed to the diagnostic criteria for LDH;herniation occurred in only one vertebral segment and was a unilateral type; received no other treatments in the previous two weeks; independently signed the informed consent form and was able to cooperate during treatment following schedule.
1.3 Exclusion criteria
Not suitable for Tuina treatment; severe dermatological diseases or primary organic disorders;fracture or osteoporosis; lumbar diseases that required surgical intervention; incomplete medical data that may affect efficacy or safety rating.
1.4 Rejection criteria
Poor compliance affected efficacy or safety evaluation; those who chose to quit halfway; took other
medications or therapies during the study that may interfere with efficacy or safety evaluation.
1.5 Termination criteria
Those who had severe adverse reactions or there occurred emergencies; the efficacy rating was unavailable due to significant errors with the trial protocol or implementation.
1.6 Statistical methods
The SPSS version 26.0 software was adopted for statistical analysis. Normally-distributed measurement data were expressed as mean ± standard deviation(±s) and checked by thet-test. Count data were processed using Pearson test.P<0.05 indicated statistical significance.
1.7 General data
This trial was approved by the Ethics Committee of the First Hospital of Hunan University of Chinese Medicine (Approval No. HN-LL-KY-2021-011-01). A total of 60 outpatients were recruited from the Tuina Department between January 2019 and October 2020 and numbered 1-60 for random-number-table grouping[17]. Thirty unrepeated numbers smaller than 60 were sought randomly from the random number table, starting with any number out of any row from left to right. The patient whose number matched the sought number would be assigned to the observation group. The rest patients were allocated to the control group. The grouping was also adjusted for balance. The drop-out rate was controlled below 15%, and new members would be recruited to replace the losses according to the randomization and balance principle.During the study, the observation and control groups each had one drop-out case due to a transfer out of town for study. Another drop-out case in the observation group was due to business travel. In the control group, one case was eliminated because of seeking acupuncture treatment, and another eliminated case was due to poor compliance. Hence, we refilled the observation group with two new cases and the control group with three new cases. After the supplement, there were no significant differences in gender, age, or disease duration between the two groups (P>0.05), suggesting comparability. The details are shown in Table 1.

Group n Gender (case) Average age(Male Female images/BZ_7_1311_2835_1350_2881.png±s, year)Disease duration(images/BZ_7_1311_2835_1350_2881.png±s, month)Observation 30 10 20 33.5±6.9 17.1±11.9 Control 30 13 17 35.0±8.2 16.3±12.4 Statistical value 0.6351) -0.7692) 0.2502)P-value 0.426 0.445 0.804
2 Treatment Methods
2.1 Observation group
The observation group received sinew-bone balancing Tuina manipulation for treatment.
2.1.1 Relaxing and adjusting sinew nodules
The physician first applied An-Pressing and Rou-Kneading manipulations with the thumb or palm around the affected lumbar segment for 5 min. The tender points or nodules in soft tissues in this area were treated with thumb Tanbo-Plucking manipulation for 5 min. The superficial-layer soft tissues above the vertebral body and deep-layer soft tissues at the back of the vertebral body should be emphasized. The treatment should go from the superficial to the deep with force increasing gradually, and the patient should have a distending aching sensation (Figure 1).
2.1.2 Three-dimensional spine adjustment
Horizontal-position Bashen-Pulling traction: The patient took a prone position and grasped the edge of the treatment bed. The physician stood by the other end and held the patient’s ankles to lift the legs by 20°,with the knees slightly away from the bed. Then the physician leaned backward to stretch the patient’s legs with force generated by pressing down the feet and the strength of the low back muscles, holding for 2 min(Figure 2).

Figure 1. Relaxing and adjusting sinew nodules

Figure 2. Horizontal-position Bashen-Pulling traction
Coronal-position Anya-Pressing in step with respiration: The herniated lumbar segment received the manipulation. Take the right side of L4as an example(similarly hereinafter). The patient took a prone position with the legs extended back (≤30°). The physician piled his palms on L4, extended the arms, and perpendicularly pressed down with the assistance of body weight.Further, the physician should swiftly press down by the end of the patient’s expiration when the patient is completely relaxed and then release to wait for the patient’s inspiration. It was repeated 5 times (one inspiration plus one expiration as one time). We can also put two pillows under the to-be-treated body region to increase the pressure on the low back(Figure 3).
Sagittal-position correction of the mamillary process:There is a noticeable nodule-like rise at the back of the superior articular process of each thoracic and lumbar vertebra, named the mamillary process. It composes the lambdoidal crest together with the accessory transverse process crest and lumbar vertebral isthmus and locates at the top of this structure (Figure 4)[18-19].The patient lay on his left side, bending the right leg and fixing the right foot at the left popliteal fossa. The physician located the L4-L5interspinous ligament with the right hand and lifted and flexed the patient’s right leg toward the head. When feeling tense in the muscles,the physician can put the patient’s right leg out of bed to “lock” it from the bottom up. Then the physician located the L3-L4interspinous ligament with the left hand and lifted and rotated the patient’s left arm with the right hand. Stop the rotation when feeling tense in the muscles to “lock” it from the top down. The physician placed the pisiform bone of his left hand at the patient’s L4mamillary process and pushed the patient’s right shoulder back to the maximum range of motion (ROM) with the right hand. Finally, the physician exerted a force with the left hand (make the forearm parallel to the bed and perpendicular to the vertebral body), during which a click would indicate the completion of correction. The left and right sides each received the treatment once (Figure 5).
2.2 Control group
The control group received the Tuina treatment introduced in the LDH chapter of theTuina Therapeutics[20], involving loosening, collateralunblocking, stretching, resetting, and sinew-regulating manipulations.
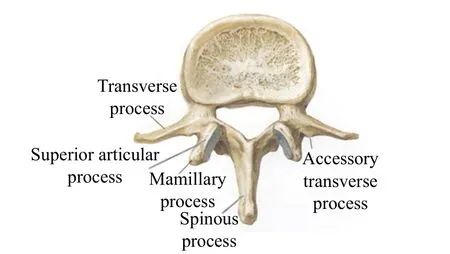

Figure 5. Sagittal-position correction of the mamillary process

Figure 6. Parallelly Ca-Rubbing the spine and erector spinae

Figure 7. Ca-Rubbing the low back transversely

Figure 8. Ca-Rubbing the lumbosacral region diagonally
2.3 Treatment course
The treatment lasted for about 15 min in both groups,performed once a day for five consecutive days. After a 2-day break, the treatment continued for another five consecutive days before evaluation.
3 Therapeutic Efficacy Observation
3.1 Observed items
3.1.1 Pain intensity
We used the visual analog scale (VAS) to score the improvement in pain, with 10 points as the highest score. The higher the score, the more serious the pain.
3.1.2 Lumbar vertebral function
Before and after treatment, we adopted the Japanese Orthopaedic Association (JOA) score to assess lumbar vertebral function. The score ranges from 0 to 29 points,and a lower score indicates more notable dysfunction.
3.1.3 Angle-dependent muscle tension of the posterior muscle chain and postural symmetry[14]
The subject lay on a TBed (TecnoBody, Italy) to receive a test by the latest version of TBed posture evaluation and training system. The patient’s body weight was first recorded at 180°. When the figure remained steady, the angle of the bed was adjusted to 120° to measure and record the patient’s muscle tension. The tension coefficient here was defined as the ratio (K) of the increased body weight measured at 120°(N) plus body weight measured at 180° to the body weight measured at 180° (M), i.e. K=(N+M):M[21]. The higher the muscle tone of the back muscles, the greater the pressure of the body on the TBed, and the higher the tension coefficient.
3.2 Clinical efficacy criteria
The improvement rate of the JOA score was calculated using the Nimodipine method to evaluate clinical efficacy directly.
Improvement rate = (Post-treatment JOA score -Pre-treatment JOA score) ÷ (29 - pre-treatment JOA score) × 100%.
Cured: The chief symptoms and body signs were gone or substantially gone, and the improvement rate was ≥95%.
Markedly effective: The chief symptoms and body signs showed notable improvements, and the improvement rate was ≥70% but <95%.
Effective: The chief symptoms and body signs showed improvements, and the improvement rate was ≥30%but <70%.
Invalid: The improvements in the chief symptoms and body signs were insignificant, and the improvement rate was <30%.
3.3 Results
3.3.1 Comparison of the clinical efficacy
The total effective rate was 86.7% in the observation group, higher than 76.7% in the control group. However,the rank-sum test showed that the between-group difference in the clinical efficacy was statistically insignificant (P>0.05), (Table 2).
3.3.2 Comparison of the VAS score
Before treatment, there was no significant difference in the VAS score between the two groups (P>0.05),suggesting the comparability. After treatment, the VAS scores changed significantly in both groups (P<0.05),and the between-group difference in the VAS score was also statistically significant (P<0.05). It is indicated that the LDH patients in both groups achieve improvements in pain intensity, and the observation group is superior to the control group. Please find the details in Table 3.
3.3.3 Comparison of the JOA score
As shown in Table 4, there was no significant difference in the JOA score between the two groups before treatment (P>0.05), suggesting the comparability.After treatment, the JOA scores changed notably in both groups (P<0.05), and the between-group difference in the JOA score was also statistically significant (P<0.05).It is indicated that the two Tuina treatment protocols both can improve the lumbar vertebral function of the LDH patients, and the observation group is superior to the control group.
3.3.4 Comparison of the angle-dependent muscle tension coefficient
As shown in Table 5, there was no significant difference in the angle-dependent muscle tension coefficient between the two groups before treatment(P>0.05), suggesting the comparability. After treatment,the angle-dependent muscle tension coefficient changed notably in both groups (P<0.05), and the between-group difference was statistically significant(P<0.05). It is suggested that the two Tuina treatment protocols both can markedly improve the angledependent posterior muscle tone of the posterior muscle chain, and the observation group is superior to the control group.

Group n Cured Markedly effective Effective Invalid Total effective rate (%)Observation 30 1 10 15 4 86.7 Control 30 1 6 16 7 76.7 Z-value -1.268 P-value 0.205

Group n Pre-treatment Post-treatment t-value P-value Observation 30 5.65±1.30 1.66±1.14 13.608 0.000 Control 30 5.50±1.23 2.34±1.05 9.728 0.000 t-value 0.700 -2.408 P-value 0.640 0.019

Group n Pre-treatment Post-treatment t-value P-value Observation 30 13.57±2.45 22.27±3.19 -12.285 0.000 Control 30 12.93±2.42 20.50±3.21 -9.437 0.000 t-value 1.008 2.136 P-value 0.317 0.037

t-value P-value 8.750 0.000 5.709 0.000
3.3.5 Comparison of the general postural symmetry of the posterior muscle chain
As shown in Table 6, there was no significant difference in the general postural symmetry of the posterior muscle chain between the two groups before treatment (P>0.05), indicating the comparability. After treatment, the general postural symmetry of the posterior muscle chain changed significantly in both groups (P<0.05), but the between-group difference was statistically insignificant (P>0.05), suggesting that both Tuina treatment protocols can notably improve the general postural symmetry of the posterior muscle chain of the LDH patients, but the between-group difference is unnoticeable.
3.3.6 Comparison of the lumbar postural symmetry of the posterior muscle chain
As shown in Table 7, there was no significant difference in the lumbar postural symmetry of the posterior muscle chain between the two groups before treatment (P>0.05), suggesting the comparability. After treatment, the lumbar postural symmetry of the posterior muscle chain changed significantly in both groups (P<0.05), and the between-group difference was statistically significant (P<0.05), indicating that both Tuina treatment protocols can notably improve the lumbar postural symmetry of the posterior muscle chain of the LDH patients, and the observation group is superior to the control group.

Group n Pre-treatment Post-treatment t-value P-value Observation 30 8.51±2.21 2.02±1.16 13.062 0.000 Control 30 8.81±2.65 2.52±1.39 14.943 0.000 t-value -0.470 -1.511 P-value 0.640 0.136

Group n Pre-treatment Post-treatment t-value P-value Observation 30 2.20±1.12 0.94±0.50 6.135 0.000 Control 30 1.98±0.99 1.43±0.78 6.035 0.000 t-value 0.806 -2.899 P-value 0.424 0.006
4 Discussion
LDH results from multiple factors and should be treated by sticking with syndrome differentiation and targeted-oriented principles. The sinew-bone balancing manipulation involves treatment of three perspectives,soft tissues of the low back, facet joints of the lumbar vertebrae, and lumbar intervertebral discs. Meanwhile,this manipulation varies its intensity, direction, and treatment time with individual tolerance. It is applied in three steps, relaxing and adjusting sinew nodules,three-dimensional adjustment of the spine, and warming and regulating meridians-collaterals, which should be performed consistently and smoothly.
The step of relaxing and adjusting sinew nodules aims to maintain the stability of core lumbar muscle groups and restore the exogenous balance of the spine.Dian-Digital pressing, An-Pressing, and Rou-Kneading can relax and unblock the sinews and collaterals to release lumbar pain. An-Pressing and Rou-Kneading with a hollow palm can reduce muscle cramps in the lumbosacral region and improve the biomechanical state of the lumbar vertebrae and the patient’s quality of life[22]. Research shows that the Rou-Kneading manipulation can down-regulate the neurokinin-1 receptor expression in the dorsal horn of the spinal cord based on a rat model of chronic constriction injury of the sciatic nerve, so as to recover the electric field and potential in the dorsal horn, restrict central sensitization,and ease pain[23]. The three-dimensional adjustment of the spine develops based on a three-dimensional unstable spine model and targets the coronal, sagittal,and transversal planes to restore a three-dimensional mechanical balance through specific vertebral adjustment manipulations. The horizontal-position Bashen-Pulling traction follows the idea of separation first before reunion and releases the peripheral articular capsules and ligaments of the misplaced lumbar vertebral segments to get ready for joint reduction. The manipulation of coronal-position Anya-Pressing in step with respiration can enlarge the intervertebral space,produce negative pressure, and tense the posterior ligaments to help with the restoration of the nucleus pulposus. The manipulation of sagittal-position correction of the mamillary process can adjust the misplaced segments, recover the normal vertebral sequence, rebuild the load-bearing force line of the lumbar spine, and offer nerves and blood vessels a proper space. In a word, the whole spine-adjustment therapy can activate the meridian Qi in the Governor Vessel, elevate Yang Qi, correct the topical muscle tone,and rebuild the biomechanical balance of the misplaced joints[24]. Besides, the warming and regulating meridians-collaterals manipulation can improve the topical microcirculation, boost the absorption of inflammatory substances, and release muscle tension and cramps to reduce pain[25]. With gentle stimulation and production of heat, the Ca-Rubbing manipulation mainly acts on the skin surface to activate Qi and blood and warm and unblock meridians and collaterals[26].
This study found no significant between-group difference in the clinical efficacy or the general postural symmetry of the posterior muscle chain after treatment.This is reasonable as the two Tuina protocols both emphasize soft tissues and can effectively relax the back muscles and reduce muscle tone. However, after treatment, the observation group showed advantages in the angle-dependent muscle tension coefficient and the lumbar postural symmetry of the posterior muscle chain. This may rely on the three-dimensional adjustment of the spine, one step of the sinew-bone balancing manipulation, which can strengthen the effect in improving the lumbar postural symmetry and angle-dependent muscle tension coefficient of the posterior muscle chain.
To conclude, the sinew-bone balancing manipulation can reduce pain and improve lumbar vertebral function in LDH patients and thus deserves a promotion. Further,it can also effectively regulate the angle-dependent muscle tension coefficient and lumbar postural symmetry of the posterior muscle chain of LDH patients.Measurement of the angle-dependent muscle tension of the posterior muscle chain with TBed can be taken as one quantitative means to objectively evaluate treatment results for LDH, which requires further large-scale multi-dimensional research.
Conflict of Interest
There is no potential conflict of interest in this article.
Acknowledgments
This work was supported by Traditional Chinese Medicine Science Research Planning Key Project of Hunan Province (湖南省中医药科研计划项目重点课题, No.201907); Innovative Research and Development Project of Development and Reform Commission of Hunan Province[湖南省发改委创新研发项目, No. 2019(127)]; Hunan Province High-level Health Talents “225” Project Training Project [湖南省高层次卫生人才“225”工程培养项目, No.2019(196)].
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received: 29 March 2021/Accepted: 28 July 2021
猜你喜欢
杂志排行
Journal of Acupuncture and Tuina Science的其它文章
- Meta-analysis of acupuncture intervening exercise-induced fatigue
- Clinical efficacy of electroacupuncture in controlling myopia in children and its influence on retinal blood flow
- Clinical study on warm needling moxibustion plus isokinetic muscle strength training in treating knee osteoarthritis
- Clinical study of warm needling moxibustion plus intra-articular injection of sodium hyaluronate for hip involvement in ankylosing spondylitis
- Clinical study of warm needling moxibustion combined with entecavir in the treatment of compensated cirrhosis due to chronic hepatitis B
- Clinical observation on moxibustion at Baihui (GV20)plus Tuina for children with postnasal drip syndrome