Meta-analysis of acupuncture intervening exercise-induced fatigue
2022-06-23NIUXinrui牛芯蕊YANGKun杨琨LIYongjie李永杰WANGXiaoling王晓玲WANGTao汪涛SHILiping史丽萍
NIU Xinrui (牛芯蕊), YANG Kun (杨琨), LI Yongjie (李永杰), WANG Xiaoling (王晓玲), WANG Tao (汪涛),SHI Liping (史丽萍)
1 Tianjin University of Traditional Chinese Medicine, Tianjin 301617, China 2 Henan Medical Technician College, Kaifeng 475000, China
3 Wuhan Sports University, Wuhan 430079, China
Abstract
Keywords: Acupuncture Therapy; Fatigue; Creatine Kinase; Lactic Acid; Lactate Dehydrogenases; Randomized Controlled Trials; Meta-analysis; Systematic Review
In competitive sports, prolonged overload training will cause overproduction of free radicals and an increase of metabolites in professional athletes,subsequently leading to internal environment disorders[1]. Exercise-induced fatigue (EIF) is defined as the body failing to maintain a certain or expected level of exercise intensity[2], manifesting as declined athletic ability, aching muscles, and the perception of tiredness,coupled with hypoglycemia[3]. It is also revealed that EIF is a result of the interaction of central neurotransmitters[4], presenting increased levels of physiological indicators such as creatine kinase (CK) and blood urea nitrogen (BUN)[5]. In the sporting context,either before a contest or during routine training, EIF will affect the training result, hinder athletes’performance, and place great pressure on the athletes[6]. Hence, seeking an effective and reasonable method to reduce EIF is a worthwhile endeavor for enhancing the sportsmen’s competitive ability and benefiting their physical and mental health.
As a crucial part of traditional Chinese medicine(TCM), acupuncture can treat diseases through unblocking meridians, regulating Qi and blood, and balancing Yin and Yang[7]. In TCM, EIF belongs to deficiency, consumption, or depletion[8]. Despite the variety in causes and symptoms, EIF is mainly associated with dysfunctions of Zang-Fu organs and consumption of Qi and blood[9]. Previous research has confirmed the effects of acupuncture in activating and redistributing neurotransmitters by stimulating muscles and nerves[10]to regulate endocrine, immune, and metabolic systems and release fatigue[11]. Acupuncture is known as convenient and easy-to-operate, safe and reliable, low cost, and free of analeptics[12], so it has been more and more widely applied in rehabilitation. However,controversy still exists due to small sample sizes and a lack of methodological standardization in most studies.Therefore, we conducted a meta-analysis to systematically evaluate the influence of acupuncture on EIF with the expectation to provide evidence for intervening EIF with acupuncture.
1 Materials and Methods
1.1 Inclusion and exclusion criteria
1.1.1 Studies We targeted the randomized controlled trials (RCTs)studying acupuncture treatment of EIF.
1.1.2 Participants
EIF in the participants was induced by a specific method listed in the original citations (for instance,Harvard step test or Bruce protocol); participant’s age and gender were unlimited; without sports injuries of lower extremities or cardiovascular diseases; willing to cooperate and consent informed.
1.1.3 Intervention measures
The treatment groups only received acupuncture treatment; the control groups were blank controls,receiving no interventions.
1.1.4 Outcome measures
Fatigue: The fatigue component in the rating of perceived exertion (RPE) and profile of mood states(POMS).
Physiological indicators: Hemoglobin (Hb), blood lactic acid (BLA), lactate dehydrogenase (LDH), CK, and BUN.
1.1.5 Exclusion criteria
Multiple publications; those whose data could not be extracted; those missing the main outcome measures;those whose full texts were not available.
1.2 Retrieval strategy
We conducted a systematic search on the computer for citations pertinent to acupuncture treatment of EIF in Chinese or English from Scopus, Springer Link, Web of Science, PubMed, Cochrane Library, China National Knowledge Infrastructure (CNKI), Wanfang Academic Journal Full-text Database (Wanfang), Chongqing VIP Database (CQVIP), and China Biology Medicine Disc(CBM) from the inception till August 2020 with the integrated use of keywords and free terms. The references of the included citations were retrieved when necessary.
The Chinese search terms included acupuncture,acupuncture-moxibustion, and exercise-induced fatigue.The query was (taking CNKI as an example):(SU=Acupuncture OR SU=Acupuncture therapy OR SU=Acupuncture-moxibustion) AND (SU=Exerciseinduced fatigue OR SU=Fatigue after exercise OR SU=Fatigue).
The English search terms included acupuncture,acupuncture-moxibustion, electroacupuncture, electroacupuncture, and exercise-induced fatigue. The query was (taking PubMed as an example): (Acupuncture[Title/Abstract] OR Acupuncture-moxibustion [Title/
Abstract] OR Electroacupuncture [Title/Abstract] OR Electro-acupuncture [Title/Abstract] OR Needling[Title/Abstract]) AND (Sports fatigue [Title/Abstract] OR Exercise-induced fatigue [Title/Abstract] OR Fatigue[Title/Abstract]).
1.3 Study screening and data extraction
Two independent reviewers (NIU X R and YANG K)screened all possible citations. Disagreements were settled by group discussions. The Endnote X7 software was used to filter out duplicates. Whether the citation met the inclusion criteria or not was confirmed based on titles and abstracts. Those failing to provide the necessary information in the titles and abstracts were confirmed by the full text. After screening, Excel was adopted to display the extracted data of the included studies, including the first author, year of publication,country of the study, quality assessment, sample size,gender, age, interventions, points, treatment frequency,follow-up duration, and outcome measures. Of which,the outcomes offered the terminal values after the intervention (consisting of mean value, standard deviation, and sample size) instead of the differences before and after the intervention.
1.4 Quality assessment
Two independent reviewers assessed the methodological quality of each included study using the standard of Cochrane systematic review handbook[13-14].After the assessment, the reviewers exchanged their review results and comments. Disagreements were solved by group discussion.
1.5 Statistical analysis
RevMan 5.3 was adopted for statistical analysis. The outcomes in this research were all continuous data.Results assessed by the same measures were expressed as weighted mean difference (WMD); if not, they were displayed as standard mean difference (SMD). The 95%confidence interval (CI) was used, along withP<0.05 indicating statistical significance[15]. Heterogeneity was checked across the included studies.P>0.100 andI2<50% suggested insignificant homogeneity, and then a fixed-effects meta-analysis would be performed. On the contrary, if significant between-study heterogeneity was found, the contributing factors would be traced and removed before a random-effects analysis was performed. If the factors could not be removed,a sub-group or sensitivity analysis was conducted to trace the source of heterogeneity.
2 Results
2.1 Retrieval results
The initial search provided 1 909 citations. After Endnote 7.0 filtered out 922 duplicates, there were 987 citations to be screened. Based on the information from titles and abstracts, 27 studies were kept, of which 16 studies were removed after review of the full text.Finally, 11 studies were included[16-26]. The included studies were all performed by Chinese authors,involving 531 participants. The screening process is shown in Figure 1.
2.2 Basic characteristics of the included studies
The 11 studies were published between 2004 and 2020[16-26], written in Chinese and based in China,involving a total of 531 participants. The treatment groups adopted acupuncture as the intervention method, and the control groups were all blank controls.Table 1 provides the basic characteristics of the studies in detail.
2.3 Methodological quality assessment
Two independent reviewers evaluated the 11 studies.Eight studies described the way of random generation,and three mentioned allocation concealment. However,the included studies failed to report blinding performance, to the participants or the research staff,such as the outcome assessors. All the included studies were evaluated as low attrition risk as no outcome data were missing. In addition, the included studies were assessed as unclear risk of selective reporting and other biases. The risk of bias assessment is shown in Figure 2-Figure 3 and Table 2.
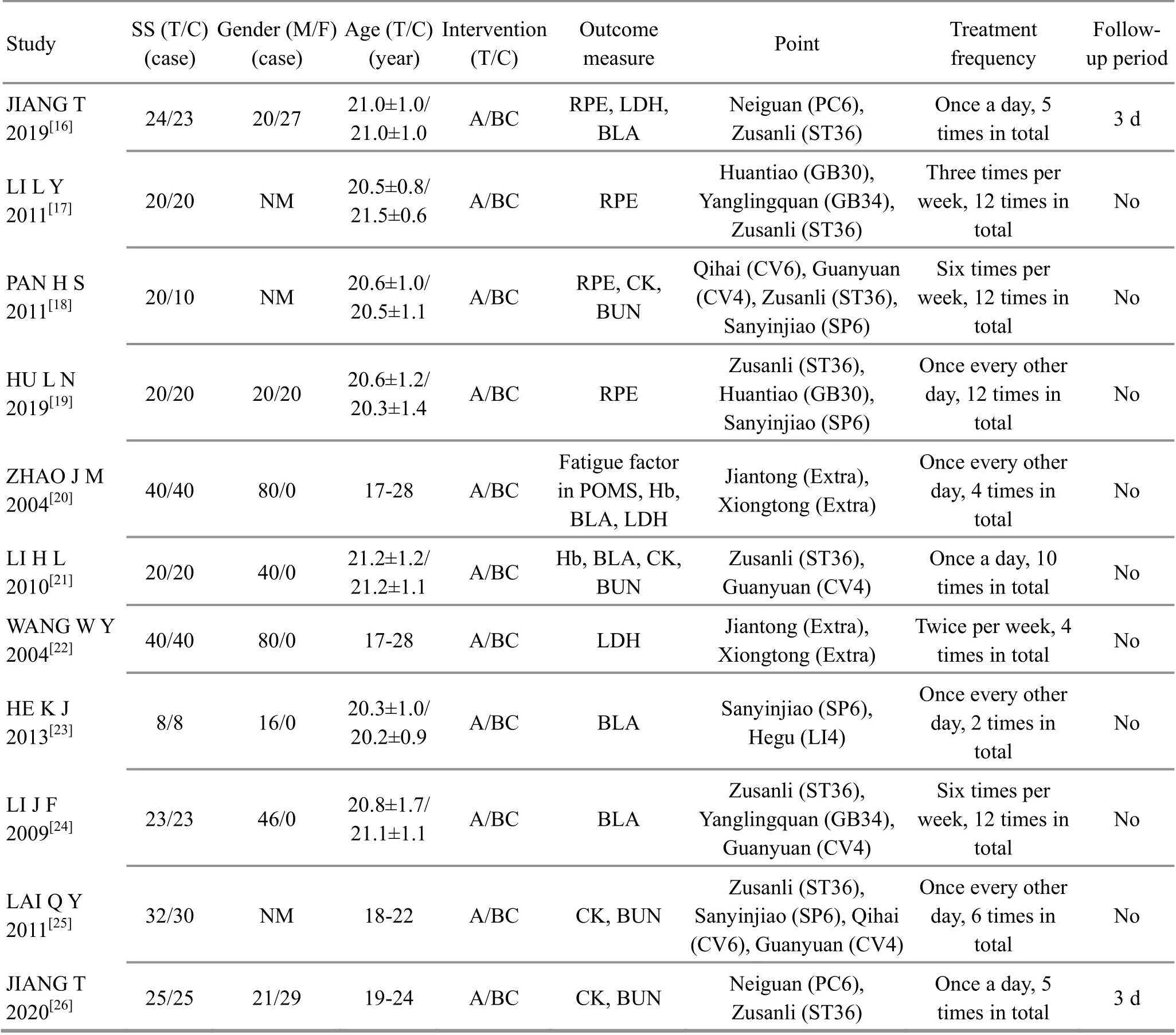
Study SS (T/C)(case)Gender (M/F)(case)Age (T/C)(year)Intervention(T/C)Outcome measure Point Treatment frequency Followup period JIANG T 2019[16] 24/23 20/27 21.0±1.0/21.0±1.0 A/BC RPE, LDH,BLA Neiguan (PC6),Zusanli (ST36)Once a day, 5 times in total 3 d LI L Y 2011[17] 20/20 NM 20.5±0.8/21.5±0.6 A/BC RPE PAN H S 2011[18] 20/10 NM 20.6±1.0/20.5±1.1 A/BC RPE, CK,BUN 2019[19] 20/20 20/20 20.6±1.2/20.3±1.4 A/BC RPE HU L N Huantiao (GB30),Yanglingquan (GB34),Zusanli (ST36)Qihai (CV6), Guanyuan(CV4), Zusanli (ST36),Sanyinjiao (SP6)Zusanli (ST36),Huantiao (GB30),Sanyinjiao (SP6)Three times per week, 12 times in total Six times per week, 12 times in total Once every other day, 12 times in total No No No ZHAO J M 2004[20] 40/40 80/0 17-28 A/BC Fatigue factor in POMS, Hb,BLA, LDH Jiantong (Extra),Xiongtong (Extra)Once every other day, 4 times in total No LI H L 2010[21] 20/20 40/0 21.2±1.2/21.2±1.1 A/BC Hb, BLA, CK,BUN Zusanli (ST36),Guanyuan (CV4)Once a day, 10 times in total No WANG W Y 2004[22] 40/40 80/0 17-28 A/BC LDH Jiantong (Extra),Xiongtong (Extra)Twice per week, 4 times in total No HE K J 2013[23] 8/8 16/0 20.3±1.0/20.2±0.9 A/BC BLA Sanyinjiao (SP6),Hegu (LI4)Once every other day, 2 times in total No 2009[24] 23/23 46/0 20.8±1.7/21.1±1.1 A/BC BLA LI J F LAI Q Y 2011[25] 32/30 NM 18-22 A/BC CK, BUN Zusanli (ST36),Yanglingquan (GB34),Guanyuan (CV4)Six times per week, 12 times in total Zusanli (ST36),Sanyinjiao (SP6), Qihai(CV6), Guanyuan (CV4)Once every other day, 6 times in total No No JIANG T 2020[26] 25/25 21/29 19-24 A/BC CK, BUN Neiguan (PC6),Zusanli (ST36)Once a day, 5 times in total 3 d

Figure 2. Ratio of risk of bias in the included studies

Figure 3. Assessment of risk of bias in the included studies
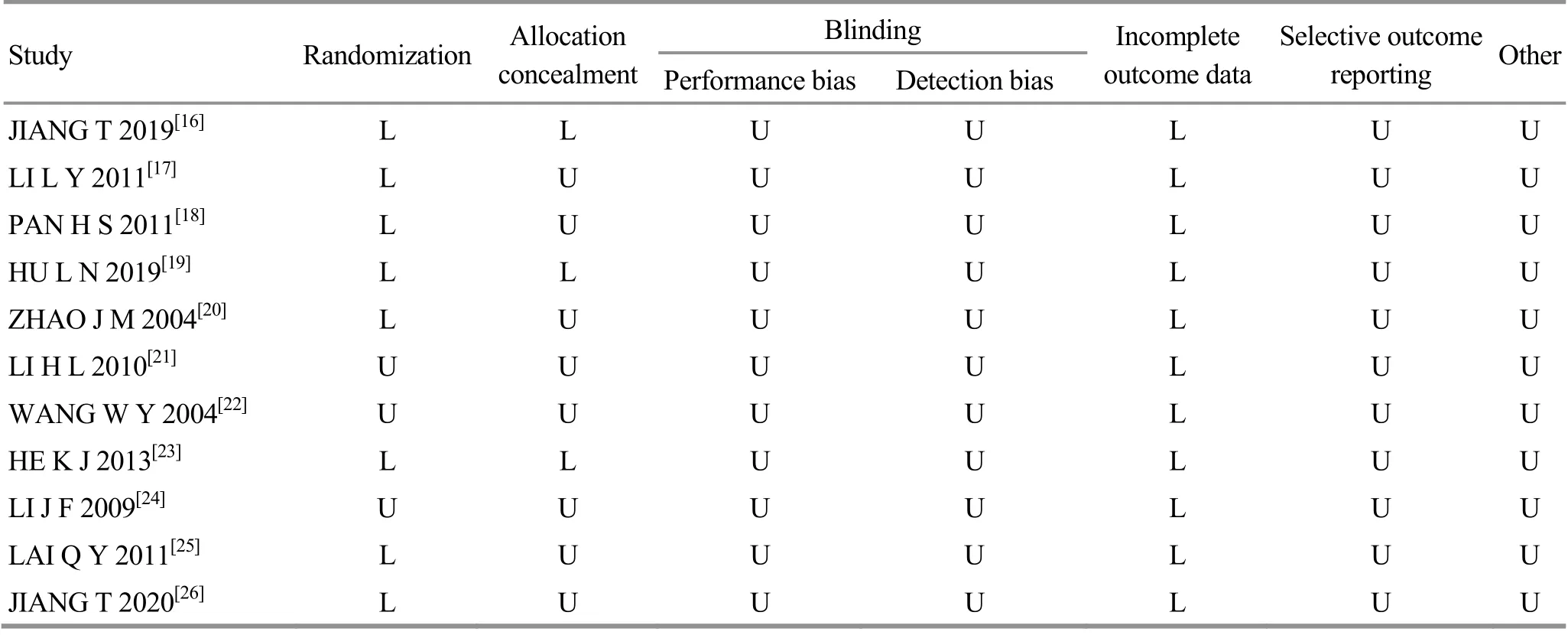
Study Randomization Allocation concealment Blinding Incomplete outcome data Performance bias Detection bias Selective outcome reporting Other JIANG T 2019[16] L L U U L U U LI L Y 2011[17] L U U U L U U PAN H S 2011[18] L U U U L U U HU L N 2019[19] L L U U L U U ZHAO J M 2004[20] L U U U L U U LI H L 2010[21] U U U U L U U WANG W Y 2004[22] U U U U L U U HE K J 2013[23] L L U U L U U LI J F 2009[24] U U U U L U U LAI Q Y 2011[25] L U U U L U U JIANG T 2020[26] L U U U L U U
2.4 Meta-analysis results
2.4.1 Perceived exertion
Five studies[16-20]analyzed the impact of acupuncture on the perceived exertion in EIF, involving a total of 237 participants. The Chi-square test showed a significant amount of between-study heterogeneity (I2=91%,P<0.001). Hence, a random-effects model was used for synthesis and analysis, finding that acupuncture had notable strength in releasing the perceived exertion compared with the control groups [SMD=-3.08, 95%CI(-4.35, -1.81),P<0.001]. The details are shown in Figure 4.
The Chi-square test showed that the removal of HU L N,et al[19]reduced the heterogeneity (I2=32%,P=0.220).The meta-analysis results indicated that acupuncture still held the advantage in releasing the perceived exertion compared with the control groups, and the difference was statistically significant [SMD=-2.12,95%CI (-2.56, -1.68),P<0.001]. The details are shown in Figure 5. Therefore, it is reasonable to speculate that this study[19]should be the source of heterogeneity.
2.4.2 Hb
Two studies[20-21]assessed the effect of acupuncture on the Hb content in EIF, involving a total of 120 participants. The Chi-square test found that the between-study heterogeneity was insignificant (I2=0%,P=1.000). Then we used a fixed-effects model for synthesis and analysis, discovering that acupuncture won out the control groups in increasing the Hb content,and the difference was statistically significant[WMD=3.89, 95%CI (1.37, 6.42),P=0.003]. The details are shown in Figure 6.

Figure 4. Meta-analysis of the effect on perceived exertion: acupuncture versus control
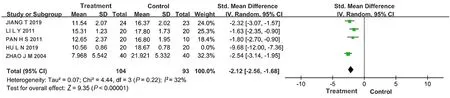
Figure 5. Meta-analysis of the effect on perceived exertion after the removal of HU L N 2019: acupuncture versus control

Figure 6. Meta-analysis of the effect on hemoglobin: acupuncture versus control
2.4.3 LDH
Three studies[16,20,22]measured the LDH content in acupuncture treatment of EIF, involving a total of 147 participants. The Chi-square test found an insignificant amount of between-study heterogeneity (I2=3%,P=0.360). Thus, a fixed-effects model was applied for synthesis and analysis and found that acupuncture down-regulated the LDH content more significantly than the control groups [WMD=-10.63, 95%CI (-17.67,-3.59),P=0.003]. The details are shown in Figure 7.
2.4.4 BLA
Five studies[16,20-21,23-24]analyzed the effect of acupuncture on the BLA content in EIF, involving a total of 229 subjects. The Chi-square test showed significant between-study heterogeneity (I2=95%,P<0.001). As shown in Figure 8, a random-effects model was used for data synthesis and analysis, noting that acupuncture produced a more significant effect in down-regulating the BLA content than the control groups [SMD=-2.65,95%CI (-4.47, -0.83),P=0.004].
A sub-group analysis was conducted based on the intervention times. The heterogeneity was insignificant across the groups with intervention times <5 (I2=15%,P=0.280). The results also revealed that acupuncture produced a more significant effect in down-regulating the BLA content than the control groups [SMD=-0.62,95%CI (-1.10, -0.13),P=0.010]. The heterogeneity was also insignificant across the groups with intervention times ≥5 (I2=44%,P=0.170). The results still confirmed that acupuncture was superior to the control groups in down-regulating the BLA content [SMD=-4.13, 95%CI(-4.96, -3.30),P<0.001]. Besides, there was a significant difference comparing the effect size between these two sub-groups (P<0.001), and the sub-group with intervention times ≥5 had a larger effect size.
2.4.5 CK
Four studies[18,21,25-26]detected the CK content in acupuncture treatment of EIF, involving a total of 182 participants. The Chi-square test showed insignificant heterogeneity across the studies (I2=42%,P=0.160). As shown in Figure 9, a fixed-effects model was adopted for data synthesis and analysis, discovering that acupuncture was more effective in down-regulating the CK content than the control groups [SMD=-0.79, 95%CI(-1.10,-0.48),P<0.001].
2.4.6 BUN
Four studies[18,21,25-26]analyzed the effect of acupuncture on the BUN content in EIF, involving a total of 182 subjects. The Chi-square test indicated that the between-study heterogeneity was insignificant (I2=47%,P=0.130). As shown in Figure 10, a fixed-effects model was used for data synthesis and analysis, suggesting that acupuncture produced a more significant effect in down-regulating the BUN content than the control groups [WMD=-1.47, 95%CI (-1.84, -1.11),P<0.001].
2.4.7 Follow-up
Two studies[16,26]conducted follow-ups. The results showed that the perceived exertion was gone entirely during the follow-up period in the acupuncture groups.However, the control group still presented aching muscles and exertion to a different extent.

Figure 7. Meta-analysis of the effect on lactate dehydrogenase: acupuncture versus control

Figure 8. Meta-analysis of the effect on blood lacyic acid: acupuncture versus control
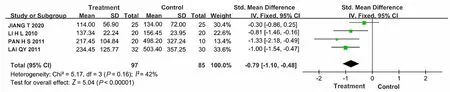
Figure 9. Meta-analysis of the effect on serum creatine kinase: acupuncture versus control
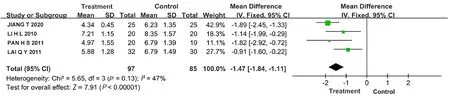
Figure 10. Meta-analysis of the effect on blood urea nitrogen: acupuncture versus control
2.5 Sensitivity analysis
Table 3 displays the results of sensitivity analyses. In the analysis of LDH, JIANG T,et al[16]weighted 68.5%.After this study was removed, the meta-analysis result suggested that there was no significant difference in down-regulating the LDH level between the acupuncture and control groups [WMD=-3.00, 95%CI(-15.55, 9.55),P=0.640]. Therefore, we need more studies to provide a more reliable result. The removal of the other two studies did not cause significant change to the analysis result.
In the analysis of CK, the sensitivity analysis revealed an insignificant change in effect size but a notable change in heterogeneity, which also reminds us to treat the analysis result with caution.
3 Discussion
3.1 Effects of acupuncture on the outcome measures in EIF
3.1.1 Effect of acupuncture on the perceived exertion in EIF
EIF belongs to the scope of deficiency syndrome in TCM. It is a temporary decline of physiological function that occurs when training intensity exceeds the body’s tolerance[27]. EIF mainly manifests as subjective weakness, achy muscles, reduced athletic capacity,etc.[28]It is usually a physiological reaction experienced by numerous athletes when receiving prolonged and high-intensity training to improve their performance[29].However, it is an uncomfortable experience and may bring tremendous mental pressure, subsequently affecting the training schedule and competing performance. Therefore, a proper assessment of perceived fatigue can help scientifically predict the improvement and prognosis of fatigue after acupuncture and provide reliable evidence for scheduling training. The current study results showed that the acupuncture groups experienced more significant relief of perceived exertion than the control groups, suggesting acupuncture’s effectiveness in reducing perceived exertion in EIF. EIF is plausibly linked to the central inhibition resulting from the interaction of central neurotransmitters[30]. Acupuncture may stimulate, excite, and redistribute the disordered neurotransmitters after exercises and finally help relieve fatigue[31]. The analysis of perceived exertion displayed a large amount of heterogeneity (I2=91%). The removal of HU L N,et al[19]lowered the heterogeneity (I2=32%),which means that this study may cause heterogeneity.When taking a close look at this study, we found that its participants took more intensive exercises and higher-frequency treatments than other studies, which may cause heterogeneity. Besides, the methodological bias between these studies can be another concern for potential heterogeneity, not to mention the variety in the scales adopted in the recruited studies. Therefore,we used the effect model SMD for data synthesis and analysis. However, SMD can only reflect the difference in measurement but not the difference among the participants, though it can unify the measurement unit.Hence, the analysis result still needs to be treated with caution. The heterogeneity and limitations all note a need for more high-quality studies.
3.1.2 Effects of acupuncture on the physiological indicators in EIF
This review analyzed five parameters, including Hb,LDH, BLA, serum CK, and BUN. After high-intensity physical activities, the Hb content will go down while the BLA and LDH contents will increase notably in the muscles, demonstrating different degrees of muscle ache and exhaustion[32]. It is indicated that the changes in these parameters are meaningful to the relief of muscle ache and fatigue. The meta-analysis found that the acupuncture groups had a higher Hb level than the control groups, together with lower BLA and LDH levels.The BLA level showed a more significant decrease in the studies with intervention frequency ≥5 times. The result tells us that high-frequency acupuncture interventions can more effectively restore body function. The effectiveness may be associated with the stress reactions after acupuncture[33]. When the responsible receptors receive the stimulation, they will act and pass the impulses to nervous centers at different levels[34]and then transmit them to the sympathetic nervous center after integration[35]. Meanwhile, the heart contracts more powerfully, the metabolism increases,and the reserve Hb is mobilized to help with the body’s tolerance[36]. The accelerated BLA metabolism also reduced the accumulation of lactic acid during strenuous physical activities[37], so the body can get rid of acidosis more quickly.
CK is a crucial indicator for evaluating muscle injuries,and it can effectively assess the tendency of muscle microdamage[38]. The CK content increases notably when muscle damage occurs. The BUN content also changes with activity intensities. An increased BUN content usually indicates excessive exercise intensity.The current review found significantly lower CK and BUN levels in the acupuncture groups compared with the control groups, suggesting that acupuncture can effectively improve muscle microdamage caused by strenuous exercises. The effectiveness may be related to the following hypothesis. Acupuncture stimulates neural stem cells to promote the synthesis of proteins and down-regulate the over-produced reactive oxygen species[39], improving muscle damage and maintaining cellular homeostasis. However, the sensitivity analysis suggested instability in the study results about CK and LDH, so it also needs to be treated with caution. More high-quality studies are required to provide stronger evidence.
3.2 Selection of points
As an essential part of TCM, acupuncture has been well-known for its preventive treatment effects[40],which means to treat the human body by unblocking meridians and regulating Qi and blood based on disease and syndrome differentiation before a disease develops or aggravates[41]. To treat EIF, points for supplement and cultivation are often selected.
Of the recruited studies, the most commonly used points were Zusanli (ST36), Guanyuan (CV4), and Sanyinjiao (SP6). As the major point, Zusanli (ST36) can cultivate the primordial and consolidate the foundation with its effect to regulate the stomach Qi and dry and dissolve dampness resulting from spleen dysfunction[42].It was discovered that this point can effectively downregulate the serum CK and BUN levels and subsequently mitigate muscle damage and boost the recovery of the body[43]. Evidence also showed that acupuncture at Zusanli (ST36) can enhance the production of adenosine triphosphate (ATP) and the level of Hb, thus strengthening the exercise endurance, relieving fatigue,and improving the internal environment of the body[44-46]. To sum up, Zusanli (ST36) can produce satisfactory efficacy in reducing fatigue and improving muscle microdamage and athletic capacity. Additionally,Guanyuan (CV4) and Sanyinjiao (SP6) were often used as adjunct points to treat EIF. Guanyuan (CV4) can tonify the lower Jiao and strengthen Yang to cultivate the primordial[47]. It was reported that acupuncture at Zusanli (ST36) and Guanyuan (CV4) at the same time could lower the burden on the heart and help manage EIF[48]. Sanyinjiao (SP6) can regulate the Qi of the Liver,Spleen, and Kidney Meridians, and it can reinforce the spleen, supplement blood, regulate liver function, and tonify the kidney. LIU H P,et al[49]found that acupuncture at Sanyinjiao (SP6) and Zusanli (ST36) can significantly enhance the activity of antioxidant enzymes on the mitochondrial membrane, remove free radicals, and maintain the balance between antioxidation and oxidation. However, due to the limited number of studies, we cannot offer the optimal point pairs in the current research.
3.3 Limitations
Findings in this study need to be interpreted considering limitations. Firstly, the included studies mainly varied in methodological quality, which may harm the conclusion of the meta-analysis. Secondly, the study was limited by language since only the Chinese and English databases were searched. Thirdly, we did not assess the publication bias due to the number of included studies. Fourthly, the grey databases were not searched. Fifthly, the results were expressed as SMD for synthesis and analysis due to the diversity in measurement tools. Sixthly, the sensitivity analysis suggested certain instability in the results. Therefore,the findings in this study should be treated with caution.
In general, acupuncture can effectively improve the perceived fatigue and muscle microdamage in EIF,accelerate the body’s recovery from exhaustion, and enhance athletic capacity. Furthermore, acupuncture is convenient to perform, and it is safe, low-cost, and does not require much for the treatment environment. Thus,this method can be an assistant approach for preventing EIF in athletes. Nevertheless, due to the limitations regarding the number of recruited studies,low rating of methodological quality, and differences in acupuncture methods, the findings provided by this study need to be interpreted with caution. Meanwhile,we expect more high-quality and large-scale RCTs to provide stronger evidence on this issue.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
This work was supported by National Natural Science Foundation of China (国家自然科学基金项目, No.81273892, No. 81503401, No. 81673732); 2011 Chinese Medicine Industry Research Project (2011 年中医药行业科研专项课题, No. 201107006); School Level Project of Preventive Treatment of Diseases in Tianjin University of Traditional Chinese Medicine in 2018 (2018 年天津中医药大学治未病校级课题, No. XJ201801).
Received: 3 September 2020/Accepted: 26 March 2021
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Effects of electroacupuncture pretreatment on motor function and cerebral blood flow in MCAO model rats
- Effect of moxibustion on N-methyl-D-aspartate receptor subtype 2B expression in hippocampus of rheumatoid arthritis model rats
- Effects of scalp acupuncture plus acupuncture exercise therapy on walking ability in children with spastic cerebral palsy
- Therapeutic efficacy and safety rating of Tui-Pushing chest-back manipulation for children with cough variant asthma
- Clinical observation on moxibustion at Baihui (GV20)plus Tuina for children with postnasal drip syndrome
- Clinical study of warm needling moxibustion combined with entecavir in the treatment of compensated cirrhosis due to chronic hepatitis B