Extensive myocardial calcification in critically ill patients receiving extracorporeal membrane oxygenation: A case report
2022-06-23MingLiangSuiChangJiangWuYaDiYangDaMeiXiaTianJieXuWeiBingTang
lNTRODUCTlON
In recent years,extracorporeal membrane oxygenation(ECMO)technology has been increasingly used in the treatment of critically ill patients with severe myocarditis,cardiogenic shock,malignant arrhythmia,severe acute respiratory distress syndrome(ARDS),and other critical illnesses[1,2].However,some rare complications have arisen due to ECMO support treatment.We here report a 17-year-old male patient with severe myocarditis who developed acute extensive myocardial calcifications while receiving ECMO support after successful treatment with intravenous arterial extracorporeal membrane oxygenation(VA-ECMO).This patient and 7 other patients retrieved from medical databases were reviewed.Patients’ clinical characteristics,epidemiology,comorbid conditions,diagnostic methods,clinical course and outcomes were collected and analyzed,in order to provide a reference for the clinical diagnosis and treatment of this disease.
The merchant started, and exclaimed: If there were not brotherly affection between us, I would cut off your head for asking me this! If you meant to kill me, retorted the prince, you would still have first to tell me what I want to know
The King, too, was amazed at the sight, but still he couldn t make up his mind to part with his daughter, so when Cola-Mattheo came to remind him of his promise he replied, I have still a third demand to make
CASE PRESENTATlON
Chief complaints
A 17-year-old man was admitted to our department with fever and chest tightness for 2 d.
I was that man. The young mother was, and is, my wife. Now, every May, our own yard is redolent with lilacs. Every Mother s Day our kids gather purple bouquets21. And every year I remember that smile on a lonely old woman s face, and the kindness that put the smile there.
History of present illness
All authors have nothing to disclose for this manuscript.
History of past illness
Kaela s beauty had a firm hold on Alfred; it filled his soul,and held a mastery over him. Beauty beamed from Kaela s every feature, glittered in her eyes, lurked30 in the corners of her mouth, andpervaded every movement of her agile31 fingers. Alfred, the sculptor,saw this. He spoke only to her, thought only of her, and the twobecame one; and so it may be said she spoke much, for he was always talking to her; and he and she were one. Such was the betrothal, and then came the wedding, with bride s-maids and wedding presents, all duly mentioned in the wedding speech. Mamma-in-law had set up Thorwalsden s bust at the end of the table, attired32 in a dressing-gown; it was her fancy that he should be a guest. Songs were sung, and cheers given; for it was a gay wedding, and they were a handsome pair. Pygmalion loved his Galatea, said one of the songs.
Personal and family history
The authors have read the CARE Checklist(2016),and the manuscript was prepared and revised according to the CARE Checklist(2016).
Physical examination
Author contributions: Sui ML designed the study,performed the literature review,drafted the manuscript,
Laboratory examinations
Laboratory examination results were as follows: glutamic oxaloacetic transaminase 1080 U/L,glutamic pyruvate transaminase 1450 U/L,creatine kinase 12 000 U/L,creatine kinase isoenzyme 2880 U/L,lactic dehydrogenase 19300 U/L,serum myoglobin 1400 ng/mL,troponin I 4.01 mg/L,white blood cell count 17.6 × 10
/L,plasma C-reactive protein 33.0 mg/L,serum procalcitonin 0.15 ng/mL,serum urea nitrogen 14.6 mmol/L,and serum creatinine 235 mmol/L.Immunoglobulin G(IgG)was 8 g/L,antinuclear and antismooth muscle antibodies were negative.Anti-Epstein-Barr virus antibodies IgG and IgM were positive.
Imaging examinations
This review showed that myocardial calcifications were mostly detected on chest CT occasionally after days to weeks of ECMO support,and most patients received no specific treatment for cardiac calcifications from the acute phase to the convalescence phase.It was speculated that the persistent myocardial calcifications might reduce elasticity of the myocardium,eventually giving rise to ventricular filling inability or diastolic dysfunction.In this study,restrictive cardiomyopathy was present in three patients who survived.However,there is little data on the long-term effects of these calcifications because few cases have been reported.The development of
life support techno-logies such as ECMO and the widespread use of renal replacement therapy are accompanied by an increasing incidence rate of acute myocardial calcifications as a complication.Therefore,for a small number of patients who have passed the acute phase of rehabilitation,it is necessary to monitor the symptoms of cardiomyopathy secondary to cardiac calcifications,and develop specific treatment and follow-up guidelines.
FlNAL DlAGNOSlS
The initial investigations showed elevated liver enzyme,creatine kinase and creatine kinase isoenzyme levels.Repeat echocardiography 1 d later demonstrated a left ventricular ejection fraction(LVEF)of 35%with moderate diastolic dysfunction,but the left ventricular end diastolic diameter showed no obvious change.Immunoglobulin M and IgG antibodies against Epstein-Barr virus were positive.There was no evidence of coronary artery abnormalities.These findings were consistent with fulminant myocarditis and cardiogenic shock.
Prince Milan and Princess Hyacinthia have just gone on this minute; they stopped for a few minutes in the church to say their prayers, and bade me light this wax candle for you, and give you their love
TREATMENT
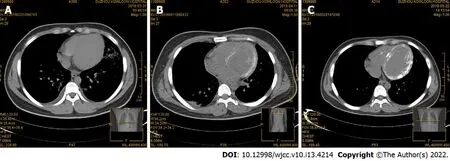
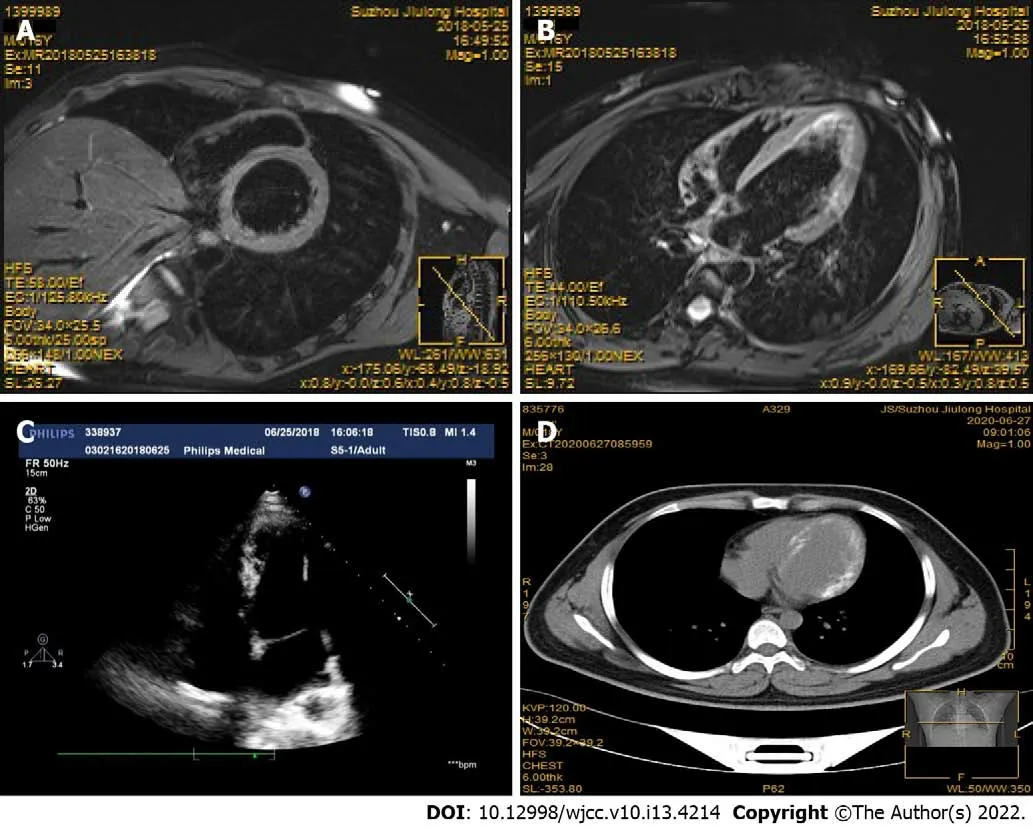
On the day after admission,the patient had a cardiac arrest due to acute left ventricular failure and malignant arrhythmia.He developed acute renal failure following cardiogenic shock.Emergency VAECMO was carried out and bedside continuous renal replacement therapy was performed to optimize fluid management.In addition,comprehensive treatment such as antiviral,myocardial nutrition,arrhythmia prevention and nutritional support were administered.The patient subsequently developed severe hypocalcemia due to cardiogenic shock,rhabdomyolysis,acute renal failure,and received approximately 1300 mg/d of calcium gluconate for the first 5 d.The patient did not receive warfarin or any other vitamin K analogue during hospitalization.There was no evidence of severe sepsis before myocardial calcification was found.An increase in the left ventricular wall density was observed on chest CT 10 d after admission(Figure 1B).Thirty days later,obvious myocardial calcifications were observed on CT images of the left ventricle,and the heart valve and right ventricle were not involved(Figure 1C).Follow-up delayed gadolinium enhanced magnetic resonance imaging(MRI)examination performed 50 d after admission showed high signal intensity in the left ventricular wall without evidence of persistent inflammation,suggesting myocardial fibrosis/scarring resulting from myocardial injury/necrosis(Figure 2A and B).Echocardiography(2 mo after hospital admission)showed a LVEF of 56%,and mild diastolic dysfunction.Echocardiography did not detect myocardial calcifications(Figure 2C).
OUTCOME AND FOLLOW-UP
The patient was discharged with heart function class II on the NYHA classification.Two years later,the patient was still alive with adequate quality of life.Echocardiography showed a LVEF of 60%,and mild diastolic dysfunction.Follow-up chest CT still showed obvious myocardial calcification in the left ventricle(Figure 2D).
DlSCUSSlON
Published medical literature on cardiac calcifications and ECMO were systematically retrieved from PubMed,Cochrane Library,EMBASE,and MEDLINE medical databases up to October 2020.We searched the databases using the following terms(MeSH),including "Calcification" AND "Noncalcification",and used the Boolean operators "AND",“OR”,and the free word "ECMO" in combination.Following elimination of duplicates and redundant articles,a total of 4 articles related to the case report,with 7 cases of ECMO-associated myocardial calcifications,were included for the final review and analysis[3-6].The data on these 7 cases and the present case were collected and analyzed.The medical history,clinical features,comorbidities,diagnostic methods and outcomes of these patients are shown in supplemental digital content(Table 1).
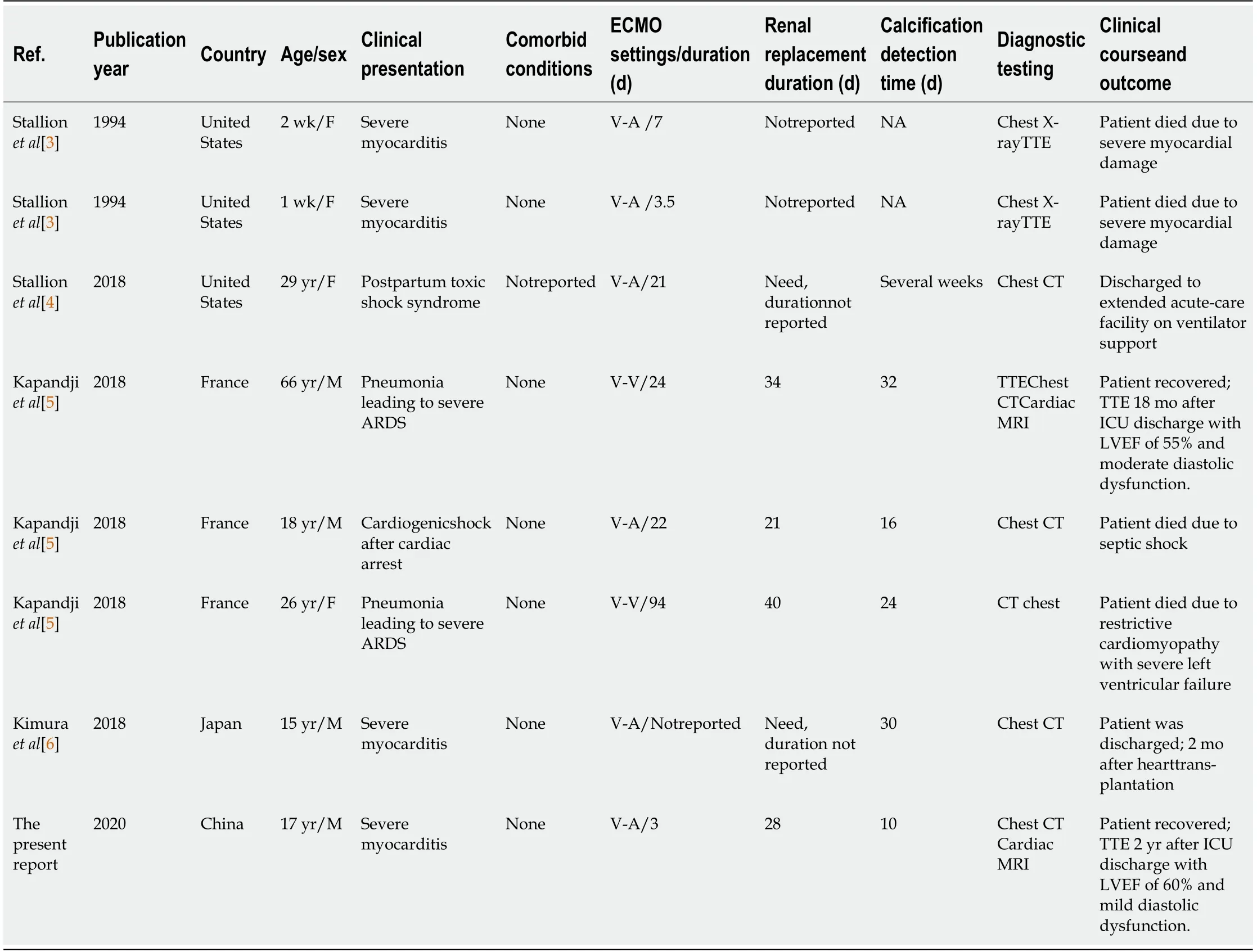
Among the 8 patients in this review,there were 4 males and 4 females,aged from 1 wk to 66 yr.All of the patients were from intensive care units,and the main etiology was sepsis-induced ARDS or severe myocarditis.Six patients(75%)received venoarterial ECMO(VA-ECMO),and two patients(25%)received venovenous ECMO(VV-ECMO).Cardiac calcifications were detected 10 to 32 d after ECMO support.Six patients(75%)required renal replacement and exogenous calcium supplementation in the acute phase of the disease.Four of the eight patients died shortly after the acute phase while in hospital.In a long-term follow-up of the reported cases,one patient was discharged with ventilator support of an extended acute-care facility.Of the two patients followed up for more than 18 mo,one presented with persistent moderate diastolic dysfunction,the other with unrelenting mild diastolic dysfunction,but left ventricular systolic function was normal in both patients.
Complications of extensive cardiac calcifications following ECMO support therapy are rare,and the mechanism may be multifactorial.The decisive contributing factor may be that ECMO treatment prolonged the survival of patients.These patients all received ECMO(especially VA-ECMO)support,did not have myocardial infarction,and were suffering from hemodynamic instability,severe metabolic acidosis,acute renal failure,and required high doses of vasoactive drugs and exogenous calcium supplementation.Possible pathological mechanisms were as follows: First,sepsis or viral infection led to severe myocardial damage,making it easier for calcium to deposit in myocardial ischemia and necrotic areas[7].Second,rhabdomyolysis combined with acute renal failure might result in severe calcium metabolic abnormalities[8].Third,intravenous supplementation of a large amount of exogenous calcium possibly further aggravated calcium deposition in necrotic areas of the myocardium[9].However,the direct role of ECMO support in myocardial calcifications remains to be confirmed.
Chest computed tomography(CT)examination at admission showed no morphological abnormalities in the heart(Figure 1A).
Clinicians should be aware that this rare but rapidly progressing complication may directly affect the clinical outcome of patients receiving ECMO support.Further research is warranted to clarify the exact pathophysiological mechanism of acute myocardial calcifications and their clinical significance in critically ill patients receiving ECMO support.
CONCLUSlON
Multiple causes including prolonged hemodynamic failure,profound acidosis,high vasopressor doses,and acute renal failure may jointly lead to extensive myocardial calcifications.The precise role of ECMO support in the timing and frequency of acute myocardial calcifications deserves further investigation.
FOOTNOTES
On admission,his temperature was 38.5°C,pulse rate was 139 bpm,respiratory rate was 33 breaths/min,and blood pressure was 89/56 mmHg.Heart sounds were scarcely audible.
formulated the data table and reviewed the manuscript;Tang WB performed the literature review,supervision,writing-review and editing;Wu CJ contributed to the data curation,investigation,and writing-original draft;Yang YD and Xu TJ performed the literature review and suggested pertinent modification;Xia DM performed data analysis,reviewed the manuscript;and All authors have read and approved the final manuscript.
The patient had no history of cardiac,renal,or other disorders.
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
The young man was led into the presence of the Iron King, who was seated on a black throne in a hall also hung with black, as a token of mourning for all the relations whom he had put to death
Two days previously,the patient developed fever,chest tightness,and tachypnea.Without treatment,there was gradual aggravation of his symptoms.
The patient had no relevant personal and family history.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
China
With further research, biomaterials modeled based on porcupine quills could provide a new class of adhesive materials, says Robert Langer, the David H. Koch Institute Professor at MIT and a senior author of the study, which appears this week in the Proceedings of the National Academy of Sciences.
Ming-Liang Sui 0000-0002-7857-5758;Chang-Jiang Wu 0000-0002-4887-0131;Ya-Di Yang 0000-0002-4126-450X;Da-Mei Xia 0000-0001-7059-4076;Tian-Jie Xu 0000-0002-1561-6292;Wei-Bing Tang 0000-0002-5736-4257.
Ma YJ
I began to understand what he meant one evening when my mother gave me money to phone a message to my father at the small upholstery shop where he had found temporary work. I went to a pay phone and dialed the number.
A
Ma YJ
1 Paolone S.Extracorporeal Membrane Oxygenation(ECMO)for Lung Injury in Severe Acute Respiratory Distress Syndrome(ARDS): Review of the Literature.
2017;26: 747-762[PMID: 27836935 DOI:10.1177/1054773816677808]
2 Smith M,Vukomanovic A,Brodie D,Thiagarajan R,Rycus P,Buscher H.Duration of veno-arterial extracorporeal life support(VA ECMO)and outcome:An analysis of the Extracorporeal Life Support Organization(ELSO)registry.
2017;21: 45[PMID: 28264702 DOI: 10.1186/s13054-017-1633-1]
3 Stallion A,Rafferty JF,Warner BW,Ziegler MM,Ryckman FC.Myocardial calcification: a predictor of poor outcome for myocarditis treated with extracorporeal life support.
1994;29: 492-494[PMID: 8014800 DOI:10.1016/0022-3468(94)90074-4]
4 Pak S,Safadi Z,Markovic JP,Marein S.Left ventricular calcification following postpartum toxic shock syndrome.
2018;7: 29[DOI: 10.4103/JCPC.JCPC_29_17]
5 Kapandji N,Redheuil A,Fouret P,Hékimian G,Lebreton G,Bréchot N,Luyt CE,Cluzel P,Combes A,Schmidt M.Extensive Myocardial Calcification in Critically Ill Patients.
2018;46: e702-e706[PMID: 29570107 DOI:10.1097/CCM.0000000000003130]
6 Kimura Y,Seguchi O,K Kono A,Matsumoto M,Kumai Y,Kuroda K,Nakajima S,Watanabe T,Matsumoto Y,Fukushima S,Yanase M,Fujita T,Ishibashi-Ueda H,Kobayashi J,Fukushima N.Massive Biventricular Myocardial Calcification in a Patient with Fulminant Myocarditis Requiring Ventricular Assist Device Support.
2019;58: 1283-1286[PMID:30568151 DOI: 10.2169/internalmedicine.2039-18]
7 Monnier-Cholley L,Roux A,Pacanowski J,Arrivé L.Myocardial calcifications following sepsis.
2018;44: 981-982[PMID: 29761215 DOI: 10.1007/s00134-018-5168-y]
8 Wada A,Nakata T,Tsuchihashi K,Aoyama S,Nanba M,Murakami H,Shimamoto K,Iimura O.Massive myocardial calcification of right and left ventricles following acute myocarditis complicated with rhabdomyolysis-induced acute renal failure.
1993;57: 567-572[PMID: 8341004 DOI: 10.1253/jcj.57.567]
9 Llach F,Felsenfeld AJ,Haussler MR.The pathophysiology of altered calcium metabolism in rhabdomyolysis-induced acute renal failure.Interactions of parathyroid hormone,25-hydroxycholecalciferol,and 1,25-dihydroxycholecalciferol.
1981;305: 117-123[PMID: 6894630 DOI: 10.1056/NEJM198107163050301]
杂志排行
World Journal of Clinical Cases的其它文章
- Capillary leak syndrome:A rare cause of acute respiratory distress syndrome
- lmproving outcomes in geriatric surgery:ls there more to the equation?
- Mass brain tissue lost after decompressive craniectomy:A case report
- Primary intracranial extraskeletal myxoid chondrosarcoma:A case report and review of literature
- Spinal canal decompression for hypertrophic neuropathy of the cauda equina with chronic inflammatory demyelinating polyradiculoneuropathy:A case report
- Enigmatic rapid organization of subdural hematoma in a patient with epilepsy:A case report