Bilateral superficial cervical plexus block for parathyroidectomy during pregnancy:A case report
2022-06-23JunYoungChungYoSeobLeeSeungYeonPyeonSangAhHanHyubHuh
lNTRODUCTlON
The use of general anesthesia for non-obstetric surgery in pregnant women is associated with maternal hazards such as the potential for a difficult airway,aspiration,hypoxemia,and concern for long-term neonatal neurocognitive effects[1,2].Cervical plexus blocks have been used in various head and neck surgeries to provide adequate anesthesia and analgesia for patients who cannot receive general anesthesia due to their comorbidities.While successful peripheral nerve blocks have been previously described in pregnant patients,the use of superficial cervical plexus block for parathyroidectomy has not been reported[3].However,superficial cervical plexus block(SCPB)is a difficult technique because it is performed in a narrow space in the neck region that contains many sensitive structures,multiple fascial layers,and complicated innervation[4].Therefore,it can result in many complications,such as phrenic nerve palsy,airway obstruction,Horner's syndrome,and local anesthetic systemic toxicity(LAST).Here,we report a successful bilateral SCPB using ultrasonography in a pregnant woman at 11 wk of gestation scheduled for parathyroidectomy.
CASE PRESENTATlON
Chief complaints
A 31-year-old nulliparous woman was at 11 wk of gestation and admitted to our hospital for parathyroidectomy with gestational hypertension.
History of present illness
When she was at 5 wk of gestational age in this pregnancy,her blood pressure was high at 160/100 mmHg with mild tachycardia of 110/min.A detailed workup,including laboratory tests,was conducted to identify the secondary cause of hypertension.
When she got to the outskirts24 of the town, led by the light of the moon, she met a fox, who offered to accompany her, an offer which Grannonia gladly accepted, saying You are most heartily25 welcome, for I don t know my way at all about the neighbourhood
And true to his word, that little elf began to do Patrick s homework. Except there was one glitch4. The elf didn t always know what to do and he needed help. Help me! Help me! he d say. And Patrick would have to help -- in whatever way.
History of past illness
The patient had a history of intrauterine fetal death with unknown etiology at 16 wk of gestation 1 year prior.The patient was diagnosed with gestational hypertension at that time,but she had not been evaluated for hypertension,and her blood pressure was not controlled by medication.
It s good to be alive, and there are people out there who want your love. Get out and do something with the family. Spend time with the people who love you while you still can. Visit, ride bikes, stroll the beach, walk the dog, get some pictures, go out for coffee and pie, or go to church.
Personal and family history
The patient had no abnormal specific personal or family history of other diseases.
Physical examination
Chung JY,Lee YS and Huh H were the patient’s anesthesiologists,performed bilateral superficial cervical plexus block and contributed to manuscript preparation;Pyeon SY was the patient’s Gynecologist,performed the analyses and interpretation and contributed to manuscript drafting;Han SA was the patient’s surgeon,performed parathyroidectomy and drafted the manuscript;Huh H reviewed and edited the manuscript;all authors issued the final approval for the version to be submitted.
Laboratory examinations
Her blood test results showed that the serum calcium level was elevated to 12.9 mg/dL(reference range: 8.8-10.6),and the parathyroid hormone level was elevated to 157 pg/mL(reference range: 15.0-65.0).And the serum 25-hydroxy vitamin D(25(OH)D)level was decreased to 16.0 ng/mL(reference range: 25-80)and the serum Phosphorus level was decreased to 1.9 mg/dL(reference range: 2.5-4.5).Other laboratory test results,including complete blood cell count(CBC),electrolyte and glucose levels,and renal and hepatic function,were within normal limits.
Imaging examinations
The final diagnosis of the present case is the parathyroid adenoma on the upper posterior of the left thyroid gland.
FlNAL DlAGNOSlS
To identify the potential causes of hypercalcemia due to hyperparathyroidism,a neck ultrasound was conducted.It revealed a 0.8 cm × 1.5 cm sized oval,hypoechoic mass in the upper posterior of the left thyroid gland,which was compatible with parathyroid adenoma.Because the patient was pregnant,99 mTc sestamibi scintigraphy for localization was contraindicated.Therefore,fine-needle aspiration(FNA)with parathyroid hormone(PTH)analysis was performed for confirmation of diagnosis.The PTH measured in the aspiration sample was 2802.0 pg/mL.Pathologic examination of FNA sample presented some giant cells and neutrophils and a few bland-looking follicular cells,which was insufficient for the confirmation of parathyroid adenoma.However,ultrasonographic findings and elevated PTH level of FNA sample highly supported the diagnosis of a parathyroid adenoma.Therefore,it was concluded clinically that her hypercalcemia was caused by parathyroid adenomainduced primary hyperparathyroidism(PHPT).
TREATMENT
As part of a multidisciplinary team specializing in maternal-fetal medicine,endocrinology surgeons and medical endocrinologists decided to surgically remove the parathyroid adenoma after the first-trimester when organogenesis of the embryo is completed because hyperparathyroidism and hypercalcemia are associated with poor perinatal outcomes such as miscarriage,stillbirth,preeclampsia,preterm birth,and postpartum hypercalcemic crisis[5,6].The patient was educated on calcium restriction and hydration to control hypercalcemia until the scheduled operation because she did not want to receive any medical treatment due to fetal safety concerns.However,there were no changes in the serum calcium levels after several weeks of conservative treatment.Therefore,the multidisciplinary team planned the surgery at 11 wk of gestational age(the first-trimester).Anesthesiologists planned SCPB without general anesthesia,considering that the patient was in the first-trimester and due to concerns regarding the toxicity of the anesthetic to the fetus.Parathyroidectomy under SCPB was scheduled for March 12,2020.The anesthesiologist visited the patient before surgery.In her preoperative laboratory test,there was no active lung lesion on chest radiography,and electrocardiography showed normal sinus rhythm.CBC,electrolyte,and glucose levels were within normal limits except calcium 14.02 mg/dL),PTH(139 pg/mL),and phosphorus(1.9 mg/dL).No other systematic abnormalities were observed.In the operating theater,the patient was monitored using three-lead electrocardiography,pulse oximetry and non-invasive blood pressure measurements.Her initial blood pressure was 164/118 mmHg,and heart rate was 85 beats
min(bpm).A peripheral vein was opened,and peripheral oxygen saturation was found to be 99% with room air.With the patient in a semi-sitting supine position,she turned her head contralateral to the procedural side.A 22-gauge needle was inserted once in a lateral-to-medial direction beneath the prevertebral fascia under ultrasound on both sides(Figure 1).After negative aspiration,0.75% of ropivacaine 8 mL was injected for SCPB(16 mL in total).As soon as SCPB was performed,the patient complained about slight hoarseness,and her blood pressure and heart rate increased to 200/120 mmHg and 120-140 bpm,respectively.There was no difficulty in respiration,and saturation was 100%under nasal cannula oxygenation 2 L/min.The tubing of the invasive blood pressure monitor was placed
the left radial artery to monitor her blood pressure in real-time,and blood samples were collected for PTH level testing immediately.

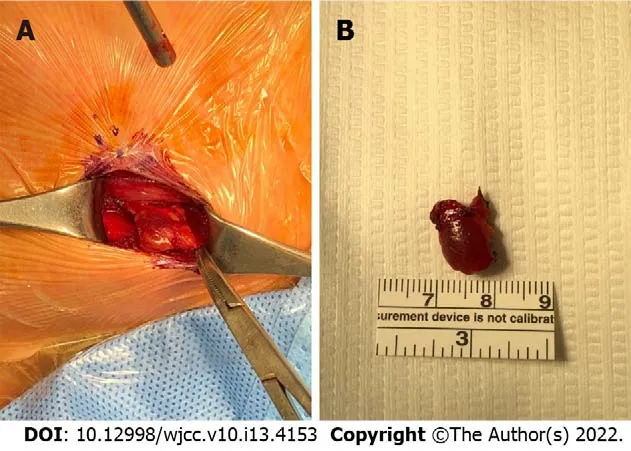
Anesthesiologists used nicardipine 1 mg twice,but her systolic blood pressure remained between 170 and 180 mmHg during surgery.After 15 min,satisfactory analgesic and anesthetic effects were achieved,and her vital signs were stabilized.Then,a parathyroidectomy was performed by the surgeon(Figure 2).The parathyroid adenoma confirmed by ultrasound and FNA was identified by ultrasound during the operation,and the adenoma was excised by making an incision directly above it.The PTH level,performed 10 min after parathyroidectomy,was 21.8 pg/mL and fell below 50% of the PTH level just before surgery(157 pg/mL)and was within the normal range.Because this finding supported that the remaining parathyroid glands secrete parathyroid hormone at a normal level,it was judged that all parathyroid adenomas in the patient's body were successfully resected.The patient was under anesthesia for 119 min,and the surgery was completed within 70 min.In total,350 mL of Hartman solution was used,and blood loss was scanty.The patient did not complain about post-surgery pain,and her hoarseness improved in the post-anesthesia care unit.As soon as the patient arrived at the ward,the obstetrician checked the status of the fetus,and there were no abnormal signs.The laboratory test results at this time shows a calcium concentration of 12.7 mg/dL,phosphorus concentration of 1.6 mg/dL,and magnesium concentration of 1.5 mg/dL.The patient was released from the hospital on postoperative day 2.
OUTCOME AND FOLLOW-UP
A follow-up examination on postoperative day 8 showed a calcium concentration of 9.4 mg/dL,PTH concentration of 43.6 pg/mL,potassium concentration of 3.7 mEq/L,sodium concentration of 134 mEq/dL,and chloride concentration of 102 mEq/dL,which returned to normal values.At this time,the patient was 12 wk and 2 d pregnant,and the fetus was healthy with a heart rate of 166 bpm.Figure 3 shows the fluctuations in the blood calcium concentration during the patient’s hospital stay.Since then,her blood pressure was stabilized to 120/80 mmHg during pregnancy,and a healthy male neonate of 2910 g was delivered vaginally at 38 wk of gestation with an Apgar score of 8/9 at 1/5 min.Her calcium level was 8.87 mg/dL on postpartum day 1,and her postpartum period was uneventful.
I was one member of the milling masses that began to filter through Park s as, day by day, the wax lettering on the front window changed from 20% OFF EVERYTHING to 30%, 40%, and on and on, like the death of a thousand cuts until the only things left were the light sockets5 and doorknobs.

DlSCUSSlON
But then there came a whirlwind and sent all the feathers flying, and swept them along the floor into a heap, where they lay as if they were trampled5 together
PHPT during pregnancy can be managed conservatively with oral or IV hydration with or without diuresis,a low calcium diet,and vitamin D supplementation[9].Medical treatments,including calcitonin and cinacalcet,are not used in pregnancy due to limited safety data.In addition,the use of bisphosphonate therapy should be avoided due to the risk of adverse effects on fetal skeletal development[10].There are several reasons why patients receive surgery and do not receive medical treatment.Due to radioactive exposure to the fetus,99 mTC sestamibi scanning and computed tomography(CT)use is restricted.FNA biopsy was performed for this patient to diagnose hypercalcemia,which revealed parathyroid adenoma.Multidisciplinary teams with close cooperation between surgeons,anesthesiologists,endocrinologists,and obstetricians are critical in caring for this unique group of patients.The first question is whether to select conservative or surgical treatment.Previous studies have reported that parathyroidectomy may be a cure for severe hypercalcemia when conservative treatments fail[11].In our case,the patient had no apparent PHPT symptoms,but her blood calcium concentration remained at 12.7 mg/dL after 2 wk of conservative treatment including hydration and calcium restriction.She also had a history of a termination of pregnancy.Besides,the patient refused medical treatment.Therefore,parathyroidectomy was considered as the treatment option after conservative treatment.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
For PHPT-related surgery,options for anesthesia include general anesthesia,cervical plexus block,or a combination of the two.Lesion localization and diagnosis in patients with PHPT depend mostly on neck ultrasound,with a sensitivity of 69% and specificity of 94%,respectively,because CT and 99 mTc radioisotope application has radiation-associated risks.However,the performance is highly dependent on the experience of the operators.We found that the left upper gland had parathyroid adenoma by FNA,and the surgeon decided to perform minimal invasive parathyroidectomy rather than traditional exploration.Due to insufficient information regarding the effect of anesthetics on early pregnancy,anesthesiologists decided to administer SCPB instead of general anesthesia.Vincent Chan
[13]suggested that a volume of 5-10 mL of local anesthesia is usually sufficient for ultra-guided cervical plexus block.Therefore,bilateral SCPB was performed with 8 mL of 0.75% ropivacaine for each side.
As soon as the block was placed,two events occurred.First,the patient reported vocal cord dysfunction with hoarseness.Although transitory,this side effect may have serious implications in patients with asymptomatic vocal cord paralysis.The patient underwent a vocal cord function test before surgery,although she had no history of vocal cord dysfunction or previous neck surgery,and the result was normal.SCPB can cause complications such as Horner's syndrome,partial brachial plexus block,and nerve blocks of phrenic and recurrent laryngeal types.These can occur as inadvertent complications of local anesthetic(LA)that spreads deeply following superficial injection[14].Nash
[15]reported that the deep cervical fascia's investing layer in the neck's anterior triangle was almost non-existent,which suggests that the fat and connective tissues that surround the structures of the neurovascular neck provide a means of direct communication between the prevertebral layer beneath the deep cervical fascia and the subcutaneous tissue.Another author suggested that it was unnecessary to use more than 5 mL of LA,and the use of larger volumes could promote a deeper spread of LA
the abovementioned anatomic pathways[16].We used 8 mL of 0.75% ropivacaine on each side(total: 16 mL),which explains why,in our case,the patient experienced hoarseness.An awareness that complications similar to those associated with deep cervical plexus blocks may also be associated with SCPB is important.
Furthermore,the patient had an elevated heart rate.Her initial heart rate was 85/min,but her heart rate increased to 136/min with hypertension after block replacement.This may be due to the LAST of ropivacaine.LAST is a potentially life-threatening adverse event correlated with increasingly prevalent LA utilization,with an incidence currently estimated as 0.03%[17].LAST is due to central nervous system(CNS)toxicity,including sensory and visual changes,muscular activation,seizure,and cardiovascular system(CVS)toxicity.The patient presented only CVS features,such as hypertension and tachycardia.Because pregnant women have reduced a1-acid glycoprotein concentrations in the plasma and increased cardiac output,accelerated perfusion of injection sites,rapid absorption of LA,and higher peaks of free LA concentrations can result[18].Therefore,reduced doses of peripheral and central neuraxial LAs are recommended.Intravenous lipid emulsion therapy was administered for LAST,but we did not use it because the patient did not present with CNS symptoms,and she was 11 wks pregnant.Tachycardia was resolved in the post-anesthesia care unit,but hypertension remained because the patient had hypertension as an underlying disease.
And when Little Two-eyes thought that Little Three-eyes was sound asleep, she said her rhyme, Little goat, bleat, Little table, appear, and ate and drank to her heart s content, and then made the table go away again, by saying, Little goat, bleat, Little table, away
CONCLUSlON
The authors would like to thank the patient for her generous release of her clinical information for this paper.
PHPT occurs in approximately 0.5% to 1.4% during pregnancy[7].PHPT is the most common cause of pregnancy-related hypercalcemia.Hypercalcemic symptoms including nausea,fatigue,constipation,depression,renal impairment,and cardiac arrhythmia occurs in 20% of patients.Rates of relevant complications are as high as 67% and 80% among pregnant women and their infants,respectively[8].Maternal complications include nephrolithiasis,pancreatitis,hyperemesis gravidarum,preeclampsia,and hypercalcemic crises.In addition,fetal complications include intrauterine growth restriction,preterm delivery,and a three to five times increased risk of miscarriage.There is also a direct relationship between serum calcium levels > 2.85 mmol/L(11.4 mg/dL)[6].
ACKNOWLEDGEMENTS
PHPT during pregnancy is rare and complicated,and needs personalized management according to the gestational age,severity of hypercalcemia,and evaluation of the tradeoff between the risks and benefits.Pregnant patients with severe PHPT,such as our case,should have their calcium concentration lowered before surgery,firstly.And then the parathyroidectomy in mid-pregnancy is currently the primary treatment option for pregnant patients with PHPT.However,due to miscarriage risk,the range of blood calcium concentrations at which surgery is an option remains under discussion.Therefore our case suggests that SCPB can be an anesthetic option for parathyroidectomy during the first trimester of pregnancy.
FOOTNOTES
Physical examination showed no positive signs.
Proper timing of surgery could reduce risks for pregnant patients and their fetuses,which is especially important for pregnant patients with PHPT.Generally,fetal organ development may be affected if surgery is performed during early pregnancy,and premature birth may result if surgery is performed late in pregnancy.Therefore,for pregnant patients with PHPT,the primary window for surgery is during mid-pregnancy(13-27 wk gestational age)[11].Norman
[12]reported a pregnancy loss rate of 48%,and the loss mainly occurred at 12.2 ± 4.5 wk,ranging from the late period of early pregnancy to the early period of mid-pregnancy.However,since her blood calcium concentration remained at 12.7 mg/dL despite 2 wk of conservative treatment,our patient underwent surgery at 11 wk of pregnancy,which was considered early pregnancy.And the surgery was successful with SCPB.Her postoperative blood calcium concentration returned to normal one week after surgery.Our case is remarkable because a delay in surgery to mid-pregnancy might have caused a miscarriage,and we used only SCPB instead of deep cervical plexus block and general anesthesia.
The authors declare that they have no conflict of interest related to this manuscript.
The authors have read the CARE Checklist(2016),and the manuscript was prepared and revised according to the CARE Checklist(2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
South Korea
Jun-Young Chung 0000-0002-3517-249X;Yo Seob Lee 0000-0001-6829-5536;Seung Yeon Pyeon 0000-0001-8601-1701;Sang-Ah Han 0000-0001-6629-955X;Hyub Huh 0000-0002-2321-1148.
I do not care where I go, answered the young man; what do you think? The girl replied that she would like to go somewhere right at the other end of the island, and build a house, far away from the huts of the fishing-folk
Li X
A
I wish with all my heart that I could put a delicate ribbon on a gayly wrapped package and give you a something to express my appreciation18 and affection. But I have nothing to give you that would surpass the most precious gift I have ever had to offer and which you already so graciously accepted months ago-the one you have held close to your heart, laughed with and probably cried with, applauded and scolded, lifted and encouraged, molded and shaped-my child.
Li X
1 Reitman E,Flood P.Anaesthetic considerations for non-obstetric surgery during pregnancy.
2011;107 Suppl 1: i72-i78[PMID: 22156272 DOI: 10.1093/bja/aer343]
2 Flood P.Fetal anesthesia and brain development.
2011;114: 479-480[PMID: 21278569 DOI:10.1097/ALN.0b013e318209aa8c]
3 Vloka JD,Hadzic A,Drobnik L.Nerve blocks in the pregnant patient.In: Birnbach D,Gatt PS,Data S,editors.Textbook of obstetric anesthesia.Philadelphia,PA: Churchill Livingstone,2000: 693–706
4 Kim JS,Ko JS,Bang S,Kim H,Lee SY.Cervical plexus block.
2018;71: 274-288[PMID:29969890 DOI: 10.4097/kja.d.18.00143]
5 Nash E,Ranka P,Tarigopula G,Rashid T.Primary hyperparathyroidism in pregnancy leading to hypercalcaemic crisis and uraemic encephalopathy.
2015;2015[PMID: 25819820 DOI: 10.1136/bcr-2014-208829]
6 McCarthy A,Howarth S,Khoo S,Hale J,Oddy S,Halsall D,Fish B,Mariathasan S,Andrews K,Oyibo SO,Samyraju M,Gajewska-Knapik K,Park SM,Wood D,Moran C,Casey RT.Management of primary hyperparathyroidism in pregnancy:a case series.
2019;2019[PMID: 31096181 DOI: 10.1530/EDM-19-0039]
7 Adami S,Marcocci C,Gatti D.Epidemiology of primary hyperparathyroidism in Europe.
2002;17 Suppl 2: N18-N23[PMID: 12412773]
8 Schnatz PF,Curry SL.Primary hyperparathyroidism in pregnancy: evidence-based management.
2002;57: 365-376[PMID: 12140371 DOI: 10.1097/00006254-200206000-00022]
9 Diaz-Soto G,Linglart A,Sénat MV,Kamenicky P,Chanson P.Primary hyperparathyroidism in pregnancy.
2013;44: 591-597[PMID: 23670708 DOI: 10.1007/s12020-013-9980-4]
10 Djokanovic N,Klieger-Grossmann C,Koren G.Does treatment with bisphosphonates endanger the human pregnancy?
2008;30: 1146-1148[PMID: 19175968 DOI: 10.1016/S1701-2163(16)34026-9]
11 Dochez V,Ducarme G.Primary hyperparathyroidism during pregnancy.
2015;291: 259-263[PMID:25367603 DOI: 10.1007/s00404-014-3526-8]
12 Norman J,Politz D,Politz L.Hyperparathyroidism during pregnancy and the effect of rising calcium on pregnancy loss: a call for earlier intervention.
2009;71: 104-109[PMID: 19138316 DOI:10.1111/j.1365-2265.2008.03495.x]
13 Bendtsen TF,Abbas S,Chan V.Ultrasound-Guided Cervical Plexus Block.In: Hadzic A.eds.Hadzic's Textbook of Regional Anesthesia and Acute Pain Management,2e.McGraw Hill;2017
14 Alzahrani T,Alnajjar M,Algarni AD,Al-Ahaideb A.Delayed Horner's syndrome following ultrasound- guided interscalene brachial plexus block.
2014;8: 121-123[PMID: 24665252 DOI: 10.4103/1658-354X.125972]
15 Nash L,Nicholson HD,Zhang M.Does the investing layer of the deep cervical fascia exist?
2005;103:962-968[PMID: 16249670 DOI: 10.1097/00000542-200511000-00010]
16 Flores S,Riguzzi C,Herring AA,Nagdev A.Horner's Syndrome after Superficial Cervical Plexus Block.
2015;16: 428-431[PMID: 25987922 DOI: 10.5811/westjem.2015.2.25336]
17 El-Boghdadly K,Pawa A,Chin KJ.Local anesthetic systemic toxicity: current perspectives.
2018;11:35-44[PMID: 30122981 DOI: 10.2147/LRA.S154512]
18 Rosenberg PH,Veering BT,Urmey WF.Maximum recommended doses of local anesthetics: a multifactorial concept.
2004;29: 564-75;discussion 524[PMID: 15635516 DOI: 10.1016/j.rapm.2004.08.003]
杂志排行
World Journal of Clinical Cases的其它文章
- Capillary leak syndrome:A rare cause of acute respiratory distress syndrome
- lmproving outcomes in geriatric surgery:ls there more to the equation?
- Mass brain tissue lost after decompressive craniectomy:A case report
- Primary intracranial extraskeletal myxoid chondrosarcoma:A case report and review of literature
- Spinal canal decompression for hypertrophic neuropathy of the cauda equina with chronic inflammatory demyelinating polyradiculoneuropathy:A case report
- Enigmatic rapid organization of subdural hematoma in a patient with epilepsy:A case report