Multiple stress fractures of unilateral femur:A case report
2022-06-23MaoTingTangChunFengLiuJinLianLiuSaijilafuZhenWang
lNTRODUCTlON
Stress fractures of the femoral neck are not common in clinical practice.They were first reported by Ernst[1]in 1936 and account for about 11% of all stress fractures[2].Additionally,simultaneous stress fractures of the femoral neck and proximal femur of the unilateral femur are even more rare and have not been reported in the literature.This article introduces a case of unilateral femoral neck and proximal femur stress fractures that were diagnosed and treated in our department,analyzes the causes,and reviews the literature to provide references for the diagnosis and treatment of these injuries.
CASE PRESENTATlON
Chief complaints
The patient was a 62-year-old female who was admitted to our hospital mainly due to pain in the right hip for 4 mo and worsening pain in the right thigh for 1 mo.At 4 mo before admission,the patient had no history of trauma.Initially,the pain in the right hip and groin slightly improved after rest but worsened after exercise.The symptoms recurred.In the month prior to admission,the patient felt pain in the right thigh,which had prompted her to visit our clinic.
History of present illness
The patient had undergone an open reduction and internal fixation for a fracture of the left proximal femur 1 year prior(Figure 1A),to address the injury sustained in a traffic accident.Due to the delayed union of the left femoral fracture,the patient supported the right limb with crutches on the ground to perform functional exercises.
So now there was only the youngest at home, and when the other two never came he also begged for a ship that he might go in search of his lost brothers

History of past illness
The patient had no history of osteoporosis or other trauma,no metabolic diseases(
,diabetes or kidney disease),no immune diseases(
,rheumatism),did not smoke tobacco or drink alcohol,and had no history of hormone and bisphosphonate usage.
After the holiday, poor George decided to buy another leather pair. Before boarding the subway, he stepped into Value Mart again to see if by any chance his gloves had been returned to the lost and found office. What colour are they? the woman in the office asked again. Black, he gave the same answer. She looked into her drawer and drew out a pair of men s leather gloves. Are they??
Personal and family history
There are many classifications of femoral stress fractures,which guide treatment strategies.Stress fractures are divided into fatigue fractures and insufficiency fractures.Insufficiency stress fractures usually have abnormal bone quality and structure,resulting in fractures that cannot withstand conventional stress.Fatigue fractures are caused by normal bone under long-term repeated stress stimulation,resulting in decreased bone production and increased bone resorption.Blickenstaff and Morris[18]divided femoral neck stress fractures into three types.Type I fractures are periosteal reactions or callus formation on the medial side of the femoral neck,with no obvious fracture lines.Type II is a visible femoral neck fracture line with no significant displacement of the fracture end.Type III is a completely displaced femoral neck fracture.According to the mechanism underlying femoral neck stress fractures,Fullerton and Snowdy[19]divided them into the following three types: Tension fracture,pressure fracture,and displacement fracture.Tension fractures occur outside and above the femoral neck,and the fracture ends are often displaced.Compression fractures are mostly fractures in the lower part of the femoral neck,which are stable fractures and are not prone to displacement of the fracture end.
Physical examination
No obvious deformity of the left hip,local redness,pigmentation,nor swollen blood vessels were observed.Tenderness at the midpoint of the left groin,tenderness on the lateral side of the femur,missing inguinal lymph nodes,positive percussion test,good passive movement of the right hip joint,and good distal blood supply were found.
Laboratory examinations
Blood biochemistry was normal.Urinalysis was unremarkable.Electrocardiogram,chest X-ray,arterial blood gas,and levels of bone turnover markers and vitamin D were normal.Specific findings from laboratory tests were serum calcium level of 2.26 mmol/L(range: 2.02-2.7 mmol/L),parathyroid hormone level of 42 pg/mL(range: 15-65 pg/mL)and 25-hidroxyvitamin D level of 13.83 μg/L(range:11.1-42.9 μg/L).
Imaging examinations
X-ray of the right hip in the anterior-posterior and lateral views showed right femoral neck and proximal femur cortical discontinuity,and varus deformity of the right hip joint(Figures 1B and 2).Computed tomography(CT)of the right hip showed that the upper cortex of the left femoral neck was discontinuous,and the fractured end was displaced(Figure 3).Bone mineral density(lumbar spine and proximal femur)was normal(T value: 0.36).
FlNAL DlAGNOSlS
It was early spring and nearing dusk as the maitre d escorted us to a table by a window, with a view of the river. And the table was beautifully set, with a smoke-gray tablecloth2 accented by bright red napkins, lemon slices in the long?stemmed water glasses, fresh flowers -the works.
The king was wild with anger at hearing these words, but he was also very tired; so he only laughed, and answered that he hoped there would be a way out of THAT fate anyhow
TREATMENT
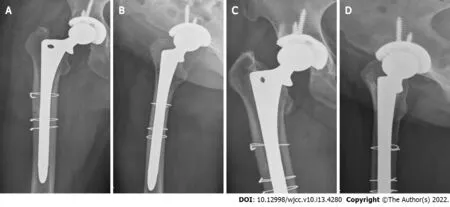
According to the classification,the stress fracture of the femoral neck in the patient was a tension fracture,with obvious displacement of the fracture end and varus deformity of the hip,which had surgical indications.Considering that the patient was an elderly female,we performed total hip arthroplasty(THA).Because of the stress fractures of the proximal femur,we chose a longer femoral prosthesis(
extended stem),and the fracture end was first fixed with a wire to prevent intraoperative fractures when the femoral stem prosthesis would be subsequently installed(Figure 4A and B).After the patient was admitted to the hospital,the examination was completed and there was no contraindication to the operation.
OUTCOME AND FOLLOW-UP
After the operation,the patient was able to move around immediately.Follow-up X-rays(after 3 mo)showed that the stress fracture of the proximal femur had mostly healed(Figure 4C and D).


DlSCUSSlON
Stress fractures were first reported in the middle of the 19
century.Femoral neck stress fractures are not common and are generally found in populations including military recruits,ballet dancers,and distance runners.Stress fractures are not easy to diagnose early,as they are difficult to see on X-rays immediately following the injury.Delayed diagnosis often results in fracture displacement,nonunion,and femoral head necrosis.Here,we reported a case of simultaneous unilateral femoral neck and proximal femur stress fractures.There have been previous reports of bilateral femoral neck stress fractures[3-7],but to the best of our knowledge,this is the first report on unilateral femoral stress fractures.
Pathogenesis
The pathogenesis of stress fractures remains a subject of debate.At present,there are two theories.One is that repeated stress stimulation leads to accelerated bone remodeling and bone resorption is greater than bone formation,leading to stress fractures.The other is that loss of muscle function around the injured area leads to abnormal bone bearing,causing the fracture.The simultaneous action of internal and external factors cause stress fractures[8];however,other factors are also involved,such as genetic factors,endocrine and metabolic diseases,vitamin D deficiency,osteoporosis,sex-related factors,ethnicity,and mental factors[4,5,9].
The patient in this case report shifted her body weight to the right lower limb because of the fracture of the left proximal femur,which is considered to be the main cause of right femoral neck stress fractures.Patel
[10]reported a case of an elderly patient with a bilateral femoral neck stress fracture.The right femoral neck pressure fracture occurred first,and the left tension fracture occurred after 3 mo.We considered the mechanism similar to that in our patient,who had stress fractures in the femoral neck and proximal femur of the unilateral femur.It is an extremely rare case,and the order of occurrence of stress fractures in the femoral neck and proximal femur is difficult to determine.The patient complained of pain in the right inguinal area and hip for 4 mo,and pain in the proximal thigh for nearly 1 mo.According to her medical history,the femoral neck stress fracture occurred first,followed by the proximal femoral stress fracture.
The cause of stress fractures of the proximal femur was initially thought to be caused by muscle fatigue.The muscle fatigue injury theory refers to the fact that bone stress is correlated with the functional state of the muscle joints,and the muscle-joint unit acts as a stress attenuator.Tensile stress caused by uncoordinated muscle contraction and muscle fatigue loss to protect the bones is the cause of stress fractures.After repeated weight bearing,the patient’s right hip abductors fatigue,resulting in accelerated bone reconstruction at the proximal and lateral sides of the femoral neck,leading to tension fractures above the femoral neck.The pain gradually improves after rest,as the weight on it has been reduced.
The thought arises, perhaps, from the arrogance of men, said thehusband. It seems a great pride to believe that we shall live forever, that we shall be as gods! Were not these the words of theserpent, the father of lies?
It was my usual response. My mother s first husband was not a kind man and his verbal and physical abuse forced her and her two children to find a safe place. He showed up on her doorstep one day with roses. She let him in and he beat her with those roses and took advantage of her. Nine months later she gave birth to a 9 lb. 13 oz. baby girl -- me.
There have also been reports in the literature that the difference in angle of the femoral neck shaft and curvature of the femoral shaft affects the distribution of lateral femur tension,leading to concentrated stress distribution in the proximal one-third of the femur and the occurrence of stress fractures of the proximal femur[14,15].Our literature review also found cases of bilateral hip varus deformity in patients with bilateral femoral neck stress fracture[16].Although the authors did not discuss it,hip varus deformity is another cause of stress fractures.It has also been reported that most patients with femoral neck stress fractures have radiographic signs of acetabular impingement[17].However,further research is needed to confirm whether these signs are correlated with stress fracture.
Classification
The patient weighed 60 kg and had a height of 165 cm.Her body mass index was 22 kg/m
.She reported having no bad personal habits nor customs,as well as no family history of cardiovascular,respiratory or gastrointestinal diseases.
The authors have read the CARE Checklist(2016),and the manuscript was prepared and revised according to the CARE Checklist(2016).
Radiographic evaluation
22.Two or three months: Note the cat s patience and ability to engineer and act upon a long term plan. He gains the king s familiarity and trust before acting upon the next stage of his scheme. Deliberate patience is an important skill in a confidence game or swindle such as this one.Return to place in story.
The early diagnosis of femoral stress fractures is difficult.Most patients go to the doctor mainly because of hip and groin discomfort,which worsens after fatigue and can be relieved by rest.Radiography is the first choice for early examination but there are usually no abnormal findings.The radiographical sensitivity is about 10%,and the missed diagnosis rate is 75%[16,23].Early diagnosis mainly relies on magnetic resonance imaging(MRI)and bone scan,with sensitivities of 100% and 85%,respectively.MRI shows the early edema reaction of the femoral neck,with visible or invisible fracture lines.After the stress fracture occurs,radiographs and CT show clear fracture lines,with or without sclerosis of the fracture end and callus formation.Although MRI is considered the gold standard for diagnosing stress fractures,if MRI exams for hip pain are routinely used,they will not only lead to a waste of medical resources but the expensive costs will increase the burden on patients and lead to conflicts between doctors and patients.For patients with pain and discomfort in the groin area and thigh and recent repetitive stress irritation,stress fractures should be suspected.If necessary,in addition to normal radiography,MRI or bone scan should be considered.
Treatment strategy
The classification of femoral neck stress fractures guides the treatment options.The most important thing in the treatment of femoral neck stress fractures is early diagnosis,which can prevent displacement of the fracture end caused by delayed or missed diagnosis,leading to further adverse complications.For non-displaced femoral neck fractures and proximal femoral fractures,a conservative treatment approach can be used(
,bed rest,local treatment)in addition to regular radiograph review.Generally,these fractures can be treated;for example,shock wave therapy can be used to treat stress fractures by promoting fracture healing[24,25].Displaced femoral neck stress fractures usually require surgical intervention.For younger patients,physicians can choose hollow nail internal fixation and nonweight bearing functional exercises.For elderly patients with fracture end displacement,THA can be used.Displaced proximal femoral fractures are mostly treated with femoral intramedullary nails.This patient had a tension fracture of the femoral neck,with obvious displacement of the fracture end and varus deformity of the hip.Considering the patient’s age,the first choice was THA.The patient had a stress fracture of the proximal femur on the same side,but there was no significant displacement of the fractured end.Therefore,the prosthesis of the femoral end used an extended stem.Simultaneously,we pre-installed a wire fixation to prevent fracture displacement during the subsequent reaming and installing of the prosthesis.
CONCLUSlON
Although femoral stress fractures are not common,patients with a history of exercise,or hip joint,groin or thigh pain should be vigilant,and femoral stress fractures should be considered.X-ray examination should be performed routinely,and if necessary,MRI exams to achieve early diagnosis and avoid adverse consequences caused by delayed diagnosis.
Stress fracture of the right femoral neck and proximal femur and postoperative fracture of the left proximal femur.
After a fracture of the right femoral neck,the fractured end is hardened and coxa varus deformity occurs.After varus deformity of the hip,the right hip muscles and lateral hip muscles are further misused,leading to the disappearance of lateral tension resistance and loss of the protective effect on the bone,which further lead to stress fractures of the lateral cortex of the proximal femur.Therefore,varus deformity of the hip provides an anatomical basis for the occurrence of stress fractures of the proximal femur.When walking and running,femoral neck stress is about 3-5 times the body weight.When there is hip varus,the stress on it further increases.Consistent with earlier reports in the literature,there is a significant correlation between hip varus deformity and stress fractures of the proximal femur[11-13].
FOOTNOTES
Tang MT reviewed the literature and contributed to drafting the manuscript;Liu CF reviewed the literature and followed up with the patient;Liu JL reviewed the literature and performed the operation;Saijilafu made important intellectual contributions to the revision of the manuscript for publication;Wang Z reviewed the literature and helped revise the manuscript;all authors issued final approval for the version to be submitted.
Suzhou Gusu Health Talent Program Training Program,No.GSWS2020121.
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
The authors declare that they have no conflict of interest.
According to the literature[3],early diagnosis plays a key role in the treatment of femoral stress fractures,especially femoral neck stress fractures,and can prevent femoral head necrosis,nonunion,and hip deformities caused by misdiagnosis and delayed diagnosis.Patel
[10]also proposed that early diagnosis is very important for the treatment of femoral neck stress fractures,and sometimes more radical treatments can be applied clinically to prevent serious adverse complications caused by fracture progression.Although early diagnosis is extremely important for femoral neck stress fractures,clinically,the early missed diagnosis rate of femoral neck stress fractures has reached 75%[16].A systematic review of the literature on 48 cases of femoral head stress fractures among exercisers found that the average delay in diagnosis is 57 d.
Stress fractures of the proximal femur are not common,and are usually called atypical femoral fractures.In recent years,it has been reported that atypical fractures of the proximal femur may be caused by the inhibition of bone transformation caused by long-term use of bisphosphonates.However,it has also been postulated that the abnormal morphology of the femur is a main reason for proximal femur stress fractures[20-22].
What’s the matter? English ladies and gentlemen always use nice perfume3 to keep a good mind. By the way, I never use perfume but I like sniffing4() from them, I have my own idea about the perfume using: Everybody used perfume but me, so everybody could smell the perfume, so they would think I used too.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
She was a strange child, quiet and thoughtful;7 and while her sisters would be delighted with the wonderful things which they obtained from the wrecks15 of vessels17, she cared for nothing but her pretty red flowers, like the sun, excepting a beautiful marble statue
China
Mao-Ting Tang 0000-0002-8853-7907;Chun-Feng Liu 0000-0003-3031-9699;Jin-Lian Liu 0000-0002-9421-7328;Saijilafu 0000-0003-2290-9808;Zhen Wang 0000-0002-6301-9767.
Youth Member of the Orthopaedic Committee of Suzhou Medical Association,No.20180903.
Fan JR
A
Fan JR
1 Ernst J.Stress Fracture of the Neck of the Femur.
1964;4: 71-83[PMID: 14106400 DOI:10.1097/00005373-196401000-00005]
2 Lodge CJ,Sha S,Yousef ASE,MacEachern C.Stress fractures in the young adult hip.
2020;95-100[DOI:10.1016/j.mporth.2020.01.006]
3 Morinaga S,Ueshima K,Maruhashi Y,Hashimoto N,Watanabe S,Nakamura T.Bilateral Stress Fractures of the Femoral Neck after Total Knee Arthroplasty: Importance of Early Diagnosis.
2020;2020: 3091693[PMID:32089926 DOI: 10.1155/2020/3091693]
4 Vedoya SP,Montero A,Del Sel H.Bilateral concomitant femoral neck stress fracture in a sedentary patient with anorexia nervosa.
2020;27: 100302[PMID: 32322651 DOI: 10.1016/j.tcr.2020.100302]
5 Fukui K,Kaneuji A,Hirata H,Tsujioka JI,Shioya A,Yamada S,Kawahara N.Bilateral spontaneous simultaneous femoral neck occult fracture in a middle-aged man due to osteoporosis and vitamin D deficiency osteomalacia: A case report and literature review.
2019;60: 358-362[PMID: 31295706 DOI: 10.1016/j.ijscr.2019.06.058]
6 Moerenhout K,Gkagkalis G,Laflamme GY,Rouleau DM,Leduc S,Benoit B.Total Hip Arthroplasty for Bilateral Femoral Neck Stress Fracture: A Case Report and Review of the Literature.
2019;2019: 2720736[PMID:31929910 DOI: 10.1155/2019/2720736]
7 Santoso A,Joo SD,Lee DH,Seol YJ,Park KS,Yoon TR.Bilateral Femoral Neck Stress Fracture Presented with Unilateral Symptoms in a Shipman Laborer: A Case Report.
2017;29: 77-80[PMID: 28316966 DOI:10.5371/hp.2017.29.1.77]
8 Astur DC,Zanatta F,Arliani GG,Moraes ER,Pochini Ade C,Ejnisman B.Stress fractures: definition,diagnosis and treatment.
2016;51: 3-10[PMID: 26962487 DOI: 10.1016/j.rboe.2015.12.008]
9 Hernigou J,Koulischer S,Maes R.Bilateral Simultaneous Femoral Neck Stress Fracture Despite Clinical Recovery from Anorexia Nervosa: A Case Report.
2017;7: e12[PMID: 29244693 DOI: 10.2106/JBJS.CC.16.00047]
10 Patel KM,Handal BA,Payne WK.Early diagnosis of femoral neck stress fractures may decrease incidence of bilateral progression and surgical interventions: A case report and literature review.
2018;53: 189-192[PMID:30412917 DOI: 10.1016/j.ijscr.2018.10.050]
11 Sariyilmaz K,Ozkunt O,Sungur M,Dikici F,Yazicioglu O.Osteomalacia and coxa vara.An unusual co-existence for femoral neck stress fracture.
2015;16: 137-140[PMID: 26454499 DOI: 10.1016/j.ijscr.2015.09.034]
12 Hagen JE,Miller AN,Ott SM,Gardner M,Morshed S,Jeray K,Alton TB,Ren D,Abblitt WP,Krieg JC.Association of atypical femoral fractures with bisphosphonate use by patients with varus hip geometry.
2014;96:1905-1909[PMID: 25410509 DOI: 10.2106/JBJS.N.00075]
13 Kim DK,Kim TH.Femoral neck shaft angle in relation to the location of femoral stress fracture in young military recruits:femoral head
femoral neck stress fracture.
2021;50: 1163-1168[PMID: 33145605 DOI:10.1007/s00256-020-03661-z]
14 Oh Y,Fujita K,Wakabayashi Y,Kurosa Y,Okawa A.Location of atypical femoral fracture can be determined by tensile stress distribution influenced by femoral bowing and neck-shaft angle: a CT-based nonlinear finite element analysis model for the assessment of femoral shaft loading stress.
2017;48: 2736-2743[PMID: 28982480 DOI:10.1016/j.injury.2017.09.023]
15 Haider IT,Schneider P,Michalski A,Edwards WB.Influence of geometry on proximal femoral shaft strains: Implications for atypical femoral fracture.
2018;110: 295-303[PMID: 29482067 DOI: 10.1016/j.bone.2018.02.015]
16 Oliveira US,Labronici PJ,João Neto A,Nishimi AY,Pires RE,Silva LH.Bilateral stress fracture of femoral neck in nonathlete - case report.
2016;51: 735-738[PMID: 28050549 DOI: 10.1016/j.rboe.2016.10.013]
17 Goldin M,Anderson CN,Fredericson M,Safran MR,Stevens KJ.Femoral Neck Stress Fractures and Imaging Features of Femoroacetabular Impingement.
2015;7: 584-592[PMID: 25591871 DOI: 10.1016/j.pmrj.2014.12.008]
18 Blickenstaff LD,Morris JM.Fatigue fracture of the femoral neck.
1966;48: 1031-1047[PMID:5917693 DOI: 10.2106/00004623-196648060-00001]
19 Fullerton LR Jr,Snowdy HA.Femoral neck stress fractures.
1988;16: 365-377[PMID: 3189661 DOI:10.1177/036354658801600411]
20 Schilcher J,Michaëlsson K,Aspenberg P.Bisphosphonate use and atypical fractures of the femoral shaft.
2011;364: 1728-1737[PMID: 21542743 DOI: 10.1056/NEJMoa1010650]
21 Shane E,Burr D,Abrahamsen B,Adler RA,Brown TD,Cheung AM,Cosman F,Curtis JR,Dell R,Dempster DW,Ebeling PR,Einhorn TA,Genant HK,Geusens P,Klaushofer K,Lane JM,McKiernan F,McKinney R,Ng A,Nieves J,O'Keefe R,Papapoulos S,Howe TS,van der Meulen MC,Weinstein RS,Whyte MP.Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American Society for Bone and Mineral Research.
2014;29: 1-23[PMID: 23712442 DOI: 10.1002/jbmr.1998]
22 Oh Y,Yamamoto K,Hashimoto J,Fujita K,Yoshii T,Fukushima K,Kurosa Y,Wakabayashi Y,Kitagawa M,Okawa A.Biological activity is not suppressed in mid-shaft stress fracture of the bowed femoral shaft unlike in "typical" atypical subtrochanteric femoral fracture: A proposed theory of atypical femoral fracture subtypes.
2020;137: 115453[PMID:32470545 DOI: 10.1016/j.bone.2020.115453]
23 Provencher MT,Baldwin AJ,Gorman JD,Gould MT,Shin AY.Atypical tensile-sided femoral neck stress fractures: the value of magnetic resonance imaging.
2004;32: 1528-1534[PMID: 15310582 DOI:10.1177/0363546503262195]
24 Shima Y,Engebretsen L,Iwasa J,Kitaoka K,Tomita K.Use of bisphosphonates for the treatment of stress fractures in athletes.
2009;17: 542-550[PMID: 19048230 DOI: 10.1007/s00167-008-0673-0]
25 Leal C,D'Agostino C,Gomez Garcia S,Fernandez A.Current concepts of shockwave therapy in stress fractures.
2015;24: 195-200[PMID: 26318502 DOI: 10.1016/j.ijsu.2015.07.723]
杂志排行

World Journal of Clinical Cases的其它文章
- Capillary leak syndrome:A rare cause of acute respiratory distress syndrome
- lmproving outcomes in geriatric surgery:ls there more to the equation?
- Mass brain tissue lost after decompressive craniectomy:A case report
- Primary intracranial extraskeletal myxoid chondrosarcoma:A case report and review of literature
- Spinal canal decompression for hypertrophic neuropathy of the cauda equina with chronic inflammatory demyelinating polyradiculoneuropathy:A case report
- Enigmatic rapid organization of subdural hematoma in a patient with epilepsy:A case report