Coexistence of meningioma and other intracranial benign tumors in non-neurofibromatosis type 2 patients:A case report and review of literature
2022-06-23TianHaoHuRunWangHaiYunWangYiFuSongJuanHanYuZiXunWangYuZhouDuanTingLiuShengHan
lNTRODUCTlON
Meningioma is the most frequent intracranial benign tumor,accounting for 37.1% of tumors overall[1].However,the concomitant occurrence of meningioma and other intracranial benign tumors is extremely rare[2].Only a few coexisting meningioma and other intracranial benign tumor cases have been reported in previous publications,such as pituitary adenoma[3,4],craniopharyngioma[5]and vestibular schwannoma[6-9].It is well-recognized that the occurrence of multiple nervous system tumors in the same patient is a characteristic of neurofibromatosis type 2(NF2)[8].Patients are diagnosed with NF2 when they meet the Manchester criteria(Supplementary Table 1)[10,11].However,clinical and pathological features of non-NF2 patients with collision-tumors remain unclear.Here we report the clinical presentation,radiological features,surgical management and outcomes in our series of 5 non-NF2 patients with concomitant meningioma and other intracranial benign tumors,including one subependymoma,which was reported for the first time,and four pituitary adenomas.In addition,we also reviewed the available literature.
CASE PRESENTATlON
Chief complaints
A 45-year-old female patient presented with a sudden night epileptic seizure 10 d prior.
A 40-year-old female patient presented with dizziness and headache for 1 mo.
A 48-year-old male patient presented with frontal and bilateral temporal headache for 1 mo.
A 52-year-old female patient presented with left progressive blurred vision for 6 mo and headaches for 2 mo.
A 29-year-old female patient presented with menstrual disorder for 2 years and intermittent headache for 3 mo.
So the Prince was appointed Imperial Swineherd. He had a dirty little roomclose by the pigsty11; and there he sat the whole day, and worked. By theevening he had made a pretty little kitchen-pot. Little bells were hung allround it; and when the pot was boiling, these bells tinkled12 in the mostcharming manner, and played the old melody,
History of present illness
The patient suffered a sudden epileptic seizure 10 d ago at night,which lasted for a few minutes.
The patient had dizziness and headaches for 1 mo.
The patient had a headache for 1 mo.The headache took place at night and affected his sleep.
I dissolved in laughter that no one else understood. Suddenly, my tension and anxiety disappeared, and I knew that when those kids got back home, their mother would be hearing a lot about how Karen doesn t do it that way. She had my sympathy and respect.
At such an unexpected sight many men would have turned and run for their lives; but the little soldier, though he was so small, had a true soldier s heart
The patient had progressive vision loss in the left eye for 6 mo.She suffered from headache from 2 mo.
The patient had menstrual disorder for 2 years.She developed amenorrhea and intermittent headaches 3 mo ago.
History of past illness
All patients had no history of specific illnesses.
But Big Lion kept all the choice bits for himself, and only gave away the little scraps30 that he did not care about eating; and the little hare grew very angry, and determined31 to have his revenge
From this time on no one asked the Cat to stand godmother; but when the winter came and there was nothing to be got outside, the Mouse remembered their provision and said, Come, Cat, we will go to our pot of fat which we have stored away; it will taste very good
Personal and family history
To the best of our knowledge,we present the first case of concomitant meningioma and intracranial subependymoma.Subependymomas are rare,benign,slow-growing tumors and represent only 0.2% to 0.7% of intracranial tumors[13-16].These tumors most often arise in the fourth ventricle(50%-60%)and the lateral ventricles(30%-40%)[14,15].Most patients present with hydrocephalus as a consequence of ventricular obstruction or less commonly focal neurological dysfunction and seizures caused by mass effects[14,17].The main purpose of surgery is to maximize the removal of the tumor[18].In the published case series,there were satisfactory postoperative mortality and morbidity rates from supratentorial subependymomas[13-18].In our case 1,resection of the left parietal meningioma and supratentorial subependymoma was accomplished
a single procedure.In a recent long-term outcome study of subependymoma,no patients exhibited a deterioration of performance status or tumor recurrence at medium to long-term follow-up[16].As with the single subependymoma,the patient in our case also had a good prognosis after operation,and there was no evidence of recurrence at the last follow-up.Although the extremely rare coexistence of meningioma and subependymoma in our case may be an incidental event,the intrinsic relationship of these two tumors might require future investigation.
Physical examination
Neurological examination of the patient found no positive signs.
There was only slight sensation in her left eye when she was admitted.
Laboratory examinations
Preoperative endocrine examination showed no abnormal changes.
Endocrine examination indicated that prolactin levels were moderately elevated(61.19 ng/mL).
Preoperative endocrine examination showed that prolactin levels were slightly elevated(59.17 ng/mL).
Imaging examinations
Brain computed tomography at the local hospital suggested an intracranial space-occupying lesion in the left parietal lobe.Brain contrast-enhanced magnetic resonance imaging(MRI)showed a well-circumscribed mass(3.6 cm × 2.7 cm × 2.7 cm)in the left parietal parafalcine and a mass(1.9 cm ×1.2 cm × 1.1 cm)in the left lateral ventricle.
MRI showed a mass(3.0 cm × 2.3 cm × 2.5 cm)in the right middle cranial fossa and a mass(0.5 cm × 0.5 cm × 0.5 cm)in the sellar region.
Until now,our understanding of the coexistence of meningioma and pituitary adenoma is based on occasional case reports[2-4,12,19-54].We reviewed all the reported cases that were available to us,and the information was summarized in Table 2.The mean age of patients was 54.6 years(range: 26-82 years),and there were 39 women and 14 men among the published cases(female:male = 2.79:1).Our 4 cases also showed a female tendency(female:male = 3:1),and the mean age was 42.8 years(range: 29-52 years).A preference for parasellar,suprasellar and sphenoid ridge localization was found with 27 reported cases(50.94%)[2-4,20-23,25,26,30,32-37,42,47-49,51,54].Consistently,the meningioma of our cases was in the petroclival,sellar and sphenoid wing regions.
There was a well-circumscribed mass(3.5 cm × 3.2 cm × 2.7 cm)surrounded with brain edema in the left sphenoid ridge and a mass(2.8 cm × 2.5 cm × 2.5 cm)encasing the internal carotid artery in the sellar and suprasellar regions,as determined by radiological examination.
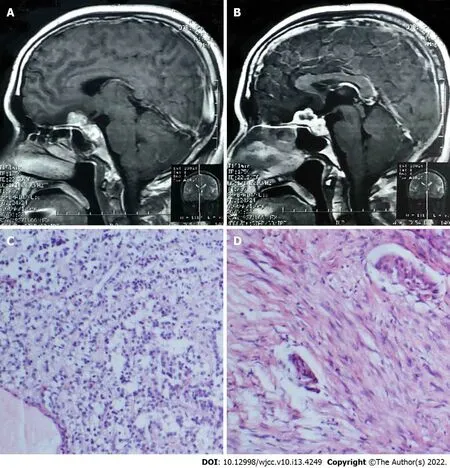
MRI showed a mass(5.7 cm × 3.3 cm)encasing the internal carotid artery located in the left petroclival region and a mass(maximum diameter 1.0 cm)located in the sellar region.
FlNAL DlAGNOSlS
the LiaoNing Revitalization Talents Program,No.XLYC1807253;and the National Natural Science Foundation of China,No.81772653.
Traditionally,the treatment of these two coexisting tumors required one craniotomy[30,31,33]or two separate operations using two different approaches[2,32,35,39].Prevedello
[42]performed a single endoscopic expanded endonasal approach in patients with coexisting tuberculum sellae meningiomas and pituitary adenoma.In our opinion,surgical strategies should be decided according to the characteristics of the coexisting tumors(
,location,size and adjacent neurovascular structures)and the clinical features of individual patients(
,symptoms and systemic conditions).Like the single pituitary adenoma,the patient with coexisting meningioma and pituitary adenoma had a favorable prognosis using the retrospective case reports.Postoperative endocrine reexamination should be periodically monitored at the endocrinology outpatient department,especially in patients with postoperative hormone imbalance after surgery.However,as this study is a retrospective analysis and the case numbers are limited,we cannot draw strong conclusions.
Harry met every train for the next three or four days. Of course, the railroad5 lines made a routine6 checkup and the police looked into the case. But nobody was any real help. I could see that they all figured that May had simply played a trick on2 him. But I never believed that, somehow.。,,。。,,。
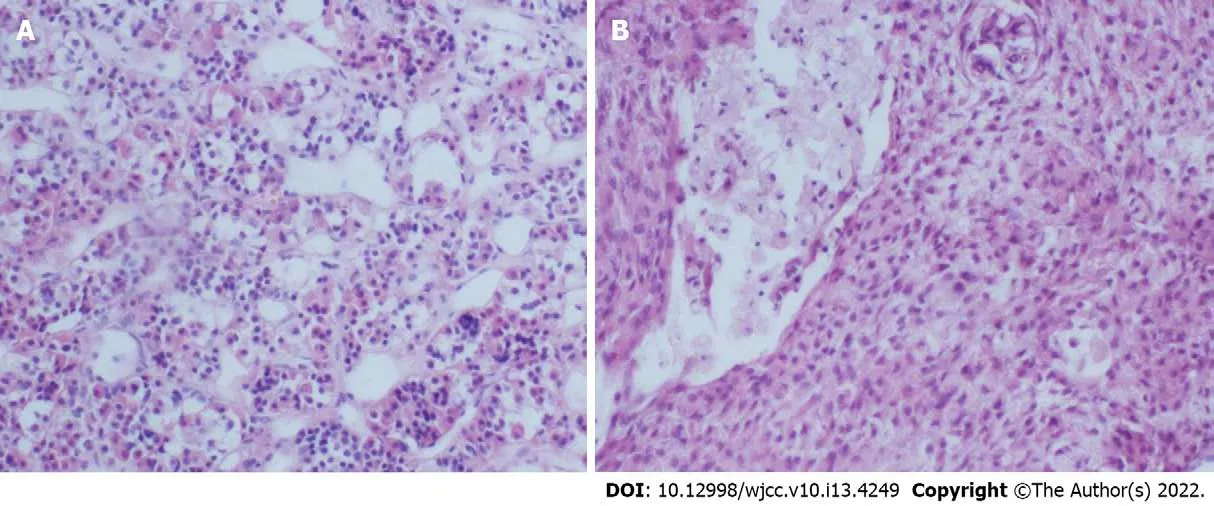
Histopathological examination showed a meningioma and non-functioning pituitary adenoma(Figure 3).
Histopathological examination showed a meningioma and non-functioning pituitary adenoma(Figure 4).
Postoperative histopathological examination showed a meningioma and non-functioning pituitary adenoma(Figure 5).



TREATMENT
After this discovery,she underwent craniotomy,and the two neoplasms were removed in one session.
First,endonasal transsphenoidal surgery was performed for resection of the intrasellar mass.Then,the right middle cranial fossa mass was removed(Simpson grade II)by transcranial surgery.
My father will then get very angry, and as the king must answer for what his fool does he will sentence him, even although he has paid his debt, either to answer three questions or to lose his life
The patient underwent transcranial resection for the two tumors through the right transpterional approach.
A single transcranial procedure was performed for removal of the sphenoid ridge mass(Simpson grade II)and sellar region mass.The pituitary tumor underwent subtotal resection.
The patient underwent craniotomy for the two tumors.The petroclival tumor was hard in consistency and rich in blood supply with internal carotid artery encasement.The tumor was also close to cranial nerves II-VI and compressed the brain stem.A subtotal resection was performed(Simpson grade IV)for the petroclival tumor.Then the intrasellar tumor was removed.
OUTCOME AND FOLLOW-UP
Between January 2011 and January 2019,2922 consecutive patients were diagnosed with meningioma in our institution.There were 5 meningioma patients(0.17%)with different intracranial benign tumors,and none of them were diagnosed with NF2.They had no history of previous irradiation.Clinical data were obtained and analyzed through retrospective medical history reviews,neuroimaging information,histopathological examination and follow-up.This retrospective study was approved by the institutional review board.Written consent was obtained from each patient for the use of their clinical data for research.
Some researchers have tried to explore the association between meningiomas and pituitary tumors.The early reports suggested that this phenomenon was related to history of irradiation for pituitary tumors[2].However,many cases with no history of radiotherapy were reported as well[24,27,29,48,49],including our cases.Therefore,Curto
[40]suggested that the coexistence of meningioma and pituitary adenoma was a coincidental phenomenon.However,there was a higher proportion of involvement of chromosome 14 and 22 in estrogen receptor positive de novo meningiomas[56].Similar genetic changes shared by two unrelated tumors found on the same chromosome may explain their coexistence[12].
They didn t hear the two people coming down the path. Dad had one arm around the girl, whose bright face was like a doll s. But they heard her when she laughed, right close by the porch. Dad didn t say anything, but the girl came forward and spoke5 to Granddad prettily6: I won t be here when you leave in the morning, so I came over to say good-bye.

The patient was followed up for 27 mo with no evidence of recurrent disease.
The patient was followed up for 24 mo,and she was in good health.
He was treated by hormone replacement therapy because of postoperative hypopituitarism.The patient was followed up for 23 mo.He took LT4 regularly and is currently in good health.
But she was not really in earnest, for her curiosity never left her a moment s peace by day or night, and she teazed and worried her husband to such a pitch, that at length he quite lost patience and blurted7 out that it all came from a wonderful golden fish which he had caught and set free again
Four months after the surgery,MRI reexamination revealed the growth of residual pituitary tumor.Subsequently,she underwent radiotherapy.The patient was in good health at the 24-mo follow-up.
As of this writing,the patient had been in stable condition for 96 mo.
DlSCUSSlON
The coexistence of meningioma and other intracranial benign tumors is a rare phenomenon that nevertheless deserves our attention.The most frequent coexistence of simultaneous benign tumors is pituitary adenoma with meningioma and schwannoma with meningioma[12].The co-occurrence of meningioma and schwannoma is more likely to occur in patients with NF2,which has been well described previously.However,the clinical characteristics of non-NF2 patients with coexisting tumors are largely unknown.
Finally she took a quarter from her jar and banged it on the glass counter. That did it! And what do you want? the pharmacist asked in an annoyed tone of voice. I m talking to my brother from Chicago whom I haven t seen in ages, he said without waiting for a reply to his question.
All patients had no special personal and family history.
Brain MRI showed lesions located in the planum sphenoidale and sellar regions.
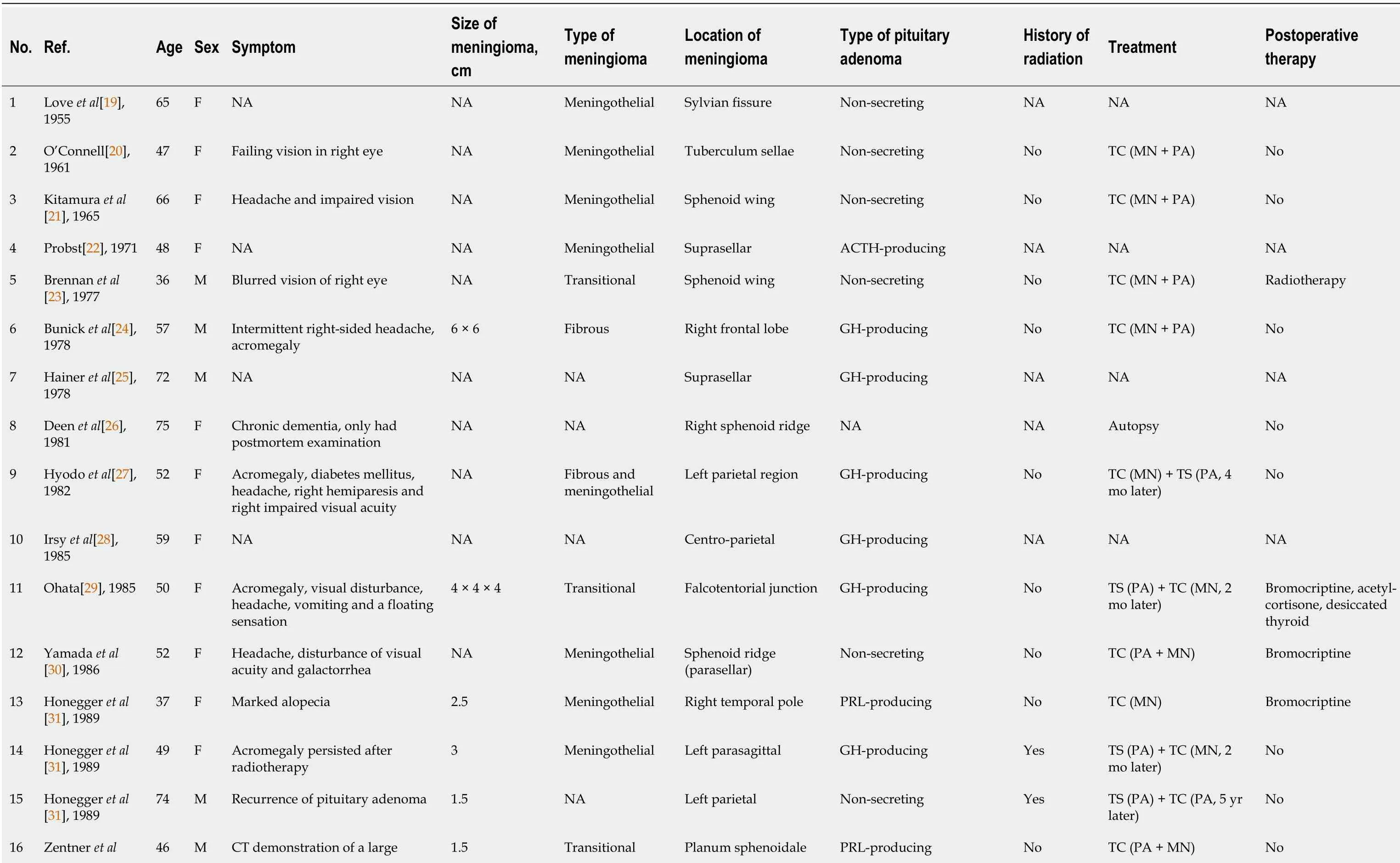



The most common type of pituitary adenoma with coexisting meningioma among reported cases was a non-secreting tumor(21/53,39.62%)followed by growth hormone-producing tumor(17/53,32.08%).In this paper,all 4 cases were non-functioning pituitary adenoma,representing the most common type.Although prolactinomas are the most frequent pituitary adenomas in general,the higher prevalence ofacromegaly in patients with coexisting meningioma has led some authors to propose an association between growth hormone-producing adenomas and meningioma[29,34,40,42,49].They suggested that persistently elevated growth hormone might stimulate arachnoid cap cells to play a role in the development of meningioma[24,39,51].A recent study suggested that patients with acromegaly were at increased risk of meningioma[55].
There were 4 female patients(80%)and 1 male patient(20%)with concomitant meningioma and other intracranial benign tumors.The mean age was 42.8 years(range: 29-79 years).The coexisting tumors included subependymoma in 1 case(20%)and pituitary adenoma in 4 cases(80%,four non-functional pituitary adenomas).The mean follow-up time was 38.8 mo(range: 23-96 mo).The clinical information of these cases is summarized in Table 1.
Moreover,due to the indolence of benign tumors,a significant portion of this coexisting tumor population may remain undiagnosed[12].MRI is useful for the diagnosis of the coexistence of two intracranial tumors but has limited significance for adjacent pituitary adenoma and meningioma[4].Histological results are necessary for diagnosis because other preoperative findings cannot support accurate diagnosis[54].For example,some reported cases were coexisting sellar meningioma and pituitary adenoma[4,42,47-49,54].Because of the close location of the two tumors,it is difficult to produce an accurate diagnosis by preoperative imaging,as in our case 3.It deserves special attention because the two different types of tumors were not definitely diagnosed before surgery but later when the pathologist’s results were obtained.The patient in case 3 developed hypopituitarism after the operation,and this complication was also reported in other similar cases[47,49].
Histopathological examination showed a meningioma and non-functioning pituitary adenoma(Figure 2).
CONCLUSlON
The simultaneous occurrence of meningioma and other intracranial benign tumors is a rare clinical event,and histological examination is necessary for their accurate diagnosis.Neurosurgeons should select the appropriate surgical strategy according to the clinical features of individual patients,which may provide the patient with a more favorable prognosis.
FOOTNOTES
Hu TH,Wang R,Duan YZ,Liu T and Han S performed the data acquisition and prepared the figures;Hu TH,Wang HY and Song YF prepared the manuscript and followed up the patients;Yu JH and Wang ZX performed histopathology examination of the patients;Hu TH and Han S designed the report;All authors contributed to the article and approved the submitted version.
Postoperative histopathological examination showed meningioma and subependymoma(Figure 1).
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
The authors declare that they have no conflicts of interest.
The authors have read the CARE Checklist(2016),and the manuscript was prepared and revised according to the CARE Checklist(2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: http://creativecommons.org/Licenses/by-nc/4.0/
China
Tian-Hao Hu 0000-0002-3865-9746;Run Wang 0000-0001-6127-4257;Hai-Yun Wang 0000-0003-3476-5848;Yi-Fu Song 0000-0002-0122-540X;Juan-Han Yu 0000-0001-7570-6284;Zi-Xun Wang 0000-0002-5652-9996;Yu-Zhou Duan 0000-0001-6476-2248;Ting Liu 0000-0001-6827-6028;Sheng Han 0000-0001-6991-0529.
Neurosurgery Society of Chinese Medical Association,Youth committee.
Liu JH
This time the dove knew better, and she answered boldly, Indeed, I shall do nothing of the sort, though her heart beat wildly with fear when she saw the jackal preparing for a spring
Filipodia
I tell you what, said the donkey, I am going to Bremen, and shall be town-musician there; go with me and engage yourself also as a musician. I will play the lute3, and you shall beat the kettledrum. 8
15.But just right; and she liked it so well that she ate it all up: Note that the smallest bear suffers the most from Goldilocks intrusion. She eats all his breakfast, breaks his chair, and sleeps in his bed. The other bears only suffer minor40 inconveniences in comparison. For this reason, the baby bear often becomes the protagonist of the story, the character that readers, especially children, relate to the best.Return to place in story.
Liu JH
1 Ostrom QT,Gittleman H,Truitt G,Boscia A,Kruchko C,Barnholtz-Sloan JS.CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2011-2015.
2018;20: iv1-iv86[PMID: 30445539 DOI: 10.1093/neuonc/noy131]
2 Partington MD,Davis DH.Radiation-induced meningioma after treatment for pituitary adenoma: case report and literature review.
1990;26: 329-331[PMID: 2407971 DOI: 10.1097/00006123-199002000-00025]
3 Amirjamshidi A,Mortazavi SA,Shirani M,Saeedinia S,Hanif H.'Coexisting pituitary adenoma and suprasellar meningioma-a coincidence or causation effect: report of two cases and review of the literature'.
2017;2017: rjx039[PMID: 28560021 DOI: 10.1093/jscr/rjx039]
4 de Vries F,Lobatto DJ,Zamanipoor Najafabadi AH,Kleijwegt MC,Verstegen MJT,Schutte PJ,Biermasz NR,van Furth WR.Unexpected concomitant pituitary adenoma and suprasellar meningioma:A case report and review of the literature.
2019;1-5[PMID: 31204511 DOI: 10.1080/02688697.2018.1556782]
5 Della Puppa A,Del Moro G,Tosatto L,Manara R,Orvieto E,Gardiman MP,Scienza R.Co-localisation of meningioma and craniopharyngioma mimicking a single skull base tumour in an elderly patient.
2011;102: 167-170[PMID: 20617364 DOI: 10.1007/s11060-010-0300-z]
6 Chen AF,Samy RN,Gantz BJ.Cerebellopontine angle tumor composed of Schwann and meningeal proliferations.
2001;127: 1385-1389[PMID: 11701080 DOI: 10.1001/archotol.127.11.1385]
7 Grauvogel J,Grauvogel TD,Taschner C,Baumgartner S,Maier W,Kaminsky J.A Rare Case of Radiologically Not Distinguishable Coexistent Meningioma and Vestibular Schwannoma in the Cerebellopontine Angle - Case Report and Literature Review.
2010;2: 111-117[PMID: 21045938 DOI: 10.1159/000320213]
8 Bachir S,Shah S,Shapiro S,Koehler A,Mahammedi A,Samy RN,Zuccarello M,Schorry E,Sengupta S.Neurofibromatosis Type 2(NF2)and the Implications for Vestibular Schwannoma and Meningioma Pathogenesis.
2021;22[PMID: 33445724 DOI: 10.3390/ijms22020690]
9 Matyja E,Kunert P,Grajkowska W,Marchel A.Coexistence of meningioma and schwannoma in the same cerebellopontine angle in a patients with NF2.
2012;50: 166-172[PMID: 22773463]
10 Evans DG,Huson SM,Donnai D,Neary W,Blair V,Newton V,Harris R.A clinical study of type 2 neurofibromatosis.
1992;84: 603-618[PMID: 1484939]
11 Evans DG,King AT,Bowers NL,Tobi S,Wallace AJ,Perry M,Anup R,Lloyd SKL,Rutherford SA,Hammerbeck-Ward C,Pathmanaban ON,Stapleton E,Freeman SR,Kellett M,Halliday D,Parry A,Gair JJ,Axon P,Laitt R,Thomas O,Afridi S,Ferner RE,Harkness EF,Smith MJ;English Specialist NF2 Research Group.Identifying the deficiencies of current diagnostic criteria for neurofibromatosis 2 using databases of 2777 individuals with molecular testing.
2019;21:1525-1533[PMID: 30523344 DOI: 10.1038/s41436-018-0384-y]
12 Furtado SV,Venkatesh PK,Ghosal N,Hegde AS.Coexisting intracranial tumors with pituitary adenomas: genetic association or coincidence?
2010;6: 221-223[PMID: 20622373 DOI: 10.4103/0973-1482.65246]
13 Bi Z,Ren X,Zhang J,Jia W.Clinical,radiological,and pathological features in 43 cases of intracranial subependymoma.
2015;122: 49-60[PMID: 25361493 DOI: 10.3171/2014.9.JNS14155]
14 Jain A,Amin AG,Jain P,Burger P,Jallo GI,Lim M,Bettegowda C.Subependymoma: clinical features and surgical outcomes.
2012;34: 677-684[PMID: 22747714 DOI: 10.1179/1743132812Y.0000000064]
15 Laghaei Farimani P,Fatehi M,Chaharyn BM,Akagami R.Large Subependymoma Inferior to the Cerebellopontine Angle With Significant Obstructive Hydrocephalus: A Case Report on an Extremely Rare Tumor.
2021;13: e18686[PMID: 34790451 DOI: 10.7759/cureus.18686]
16 Rincon-Torroella J,Rakovec M,Khalafallah AM,Liu A,Bettegowda A,Kut C,Rodriguez FJ,Weingart J,Luciano M,Olivi A,Jallo GI,Brem H,Mukherjee D,Lim M,Bettegowda C.Clinical features and surgical outcomes of intracranial and spinal cord subependymomas.
2022;1-12[PMID: 35148513 DOI: 10.3171/2021.12.JNS211643]
17 Rushing EJ,Cooper PB,Quezado M,Begnami M,Crespo A,Smirniotopoulos JG,Ecklund J,Olsen C,Santi M.Subependymoma revisited: clinicopathological evaluation of 83 cases.
2007;85: 297-305[PMID: 17569000 DOI: 10.1007/s11060-007-9411-6]
18 Kandenwein JA,Bostroem A,Feuss M,Pietsch T,Simon M.Surgical management of intracranial subependymomas.
2011;153: 1469-1475[PMID: 21499782 DOI: 10.1007/s00701-011-1007-4]
19 LOVE JG,BLACKBURN CM.Association of intracranial meningioma with pituitary adenoma;report of successfully treated case.
1955;38: 335-336[PMID: 14369958]
20 O'CONNELL JE.Intracranial meningiomata associated with other tumours involving the central nervous system.
1961;48: 373-383[PMID: 13730031 DOI: 10.1002/bjs.18004821005]
21 Kitamura K,Terao H,Kamano S,Nakamura N,Hayakawa I,Ishijima T,Sano K.[Primary Multiple Brain Tumors].
1965;17: 109-117[PMID: 14302534]
22 Probst A.[Combined occurrence of Cushing-syndrome,hypophyseal adenoma and suprasellar meningeoma.Case report].
1971;32: 75-82[PMID: 5117477]
23 Brennan TG Jr,Rao CV,Robinson W,Itani A.Case report.Tandem lesions: chromophobe adenoma and meningioma.
1977;1: 517-520[PMID: 615235]
24 Bunick EM,Mills LC,Rose LI.Association of acromegaly and meningiomas.
1978;240: 1267-1268[PMID:682310]
25 Hainer V,Krejcík L,Pelikán J,Tvaroh F,Urbánek J.[Meningioma in contact with eosinophilic adenoma in a patient with acromegaly(author's transl)].
1978;117: 829-831[PMID: 210948]
26 Deen HG Jr,Laws ER Jr.Multiple primary brain tumors of different cell types.
1981;8: 20-25[PMID:6259551 DOI: 10.1227/00006123-198101000-00005]
27 Hyodo A,Nose T,Maki Y,Enomoto T.[Pituitary adenoma and meningioma in the same patient(author's transl)].
1982;25: 66-67[PMID: 6287322 DOI: 10.1055/s-2008-1053959]
28 Irsy G,Góth M,Slovik F,Bálint K,Szabolcs I,Pásztor E,Szilágyi G.Growth hormone producing pituitary adenoma and meningioma.
1985;46: 337-343[PMID: 3914151]
29 Ohata K.[Simultaneous occurrence of a pituitary adenoma and a falcotentorial junction meningioma.Case report].
1985;25: 680-686[PMID: 2415864 DOI: 10.2176/nmc.25.680]
30 Yamada K,Hatayama T,Ohta M,Sakoda K,Uozumi T.Coincidental pituitary adenoma and parasellar meningioma: case report.
1986;19: 267-270[PMID: 3748357 DOI: 10.1227/00006123-198608000-00016]
31 Honegger J,Buchfelder M,Schrell U,Adams EF,Fahlbusch R.The coexistence of pituitary adenomas and meningiomas:three case reports and a review of the literature.
1989;3: 59-69[PMID: 2675917 DOI:10.3109/02688698909001027]
32 Zentner J,Gilsbach J.Pituitary adenoma and meningioma in the same patient.Report of three cases.
1989;238: 144-148[PMID: 2721531 DOI: 10.1007/BF00451002]
33 Uno M,Ohshima T,Matsumoto K,Sano T.[A case report of adjacent tumor of sphenoid ridge meningioma and GH producing pituitary adenoma].
1991;19: 583-587[PMID: 1881528]
34 Cannavò S,Curtò L,Fazio R,Paterniti S,Blandino A,Marafioti T,Trimarchi F.Coexistence of growth hormone-secreting pituitary adenoma and intracranial meningioma:A case report and review of the literature.
1993;16:703-708[PMID: 8282967 DOI: 10.1007/BF03348915]
35 Abs R,Parizel PM,Willems PJ,Van de Kelft E,Verlooy J,Mahler C,Verhelst J,Van Marck E,Martin JJ.The association of meningioma and pituitary adenoma: report of seven cases and review of the literature.
1993;33: 416-422[PMID: 8307062 DOI: 10.1159/000116986]
36 Görge HH,Pöll W,Gers B.[Para- and suprasellar meningioma coincident with a hormonally active intrasellar hypophyseal adenoma--case report].
1993;54: 190-196[PMID: 8128789]
37 Laun A,Lenzen J,Hildebrandt G,Schachenmayr W.[Tuberculum sellae meningioma and hypophyseal adenoma in a woman].
1993;54: 119-124[PMID: 8237164]
38 Mathuriya SN,Vasishta RK,Dash RJ,Kak VK.Pituitary adenoma and parasagittal meningioma: an unusual association.
2000;48: 72-74[PMID: 10751818]
39 Maiuri F,Cappabianca P,Iaconetta G,Esposito F,Messina A.Simultaneous presentation of meningiomas with other intracranial tumours.
2005;19: 368-375[PMID: 16455550 DOI: 10.1080/02688690500305548]
40 Curto L,Squadrito S,Almoto B,Longo M,Granata F,Salpietro F,Torre ML,Marini F,Trimarchi F,Cannavo S.MRI finding of simultaneous coexistence of growth hormone-secreting pituitary adenoma with intracranial meningioma and carotid artery aneurysms: report of a case.
2007;10: 299-305[PMID: 17334927 DOI:10.1007/s11102-007-0011-4]
41 da Costa LB,Riva-Cambrin J,Tandon A,Tymianski M.Pituitary adenoma associated with intraventricular meningioma:case report.
2007;17: 347-351[PMID: 18330434 DOI: 10.1055/s-2007-986440]
42 Prevedello DM,Thomas A,Gardner P,Snyderman CH,Carrau RL,Kassam AB.Endoscopic endonasal resection of a synchronous pituitary adenoma and a tuberculum sellae meningioma: technical case report.
2007;60: E401;discussion E401[PMID: 17415151 DOI: 10.1227/01.NEU.0000255359.94571.91]
43 Basu A,Brabant G,Gnanalingham KK.More than a prolactinoma.
2010;13: 87-88[PMID: 18461461 DOI:10.1007/s11102-008-0129-z]
44 Guaraldi F,Corazzini V,Gallia GL,Grottoli S,Stals K,Dalantaeva N,Frohman LA,Korbonits M,Salvatori R.Genetic analysis in a patient presenting with meningioma and familial isolated pituitary adenoma(FIPA)reveals selective involvement of the R81X mutation of the AIP gene in the pathogenesis of the pituitary tumor.
2012;15 Suppl 1:S61-S67[PMID: 22527616 DOI: 10.1007/s11102-012-0391-y]
45 Ramirez Mdel P,Restrepo JE,Syro LV,Rotondo F,Londoño FJ,Penagos LC,Uribe H,Horvath E,Kovacs K.Neurocysticercosis,meningioma,and silent corticotroph pituitary adenoma in a 61-year-old woman.
2012;2012: 340840[PMID: 23346440 DOI: 10.1155/2012/340840]
46 Masoodi SR,Mir SA,Farooqui KJ,Bhat AR,Wani AI,Bhat MA.Growth hormone secreting pituitary macroadenoma and meningioma: An association or coincidence?
2013;17: 770-771[PMID: 23961510 DOI:10.4103/2230-8210.113785]
47 Mahvash M,Igressa A,Pechlivanis I,Weber F,Charalampaki P.Endoscopic endonasal transsphenoidal approach for resection of a coexistent pituitary macroadenoma and a tuberculum sellae meningioma.
2014;9: 236[PMID: 25685225 DOI: 10.4103/1793-5482.146629]
48 Karsy M,Sonnen J,Couldwell WT.Coincident pituitary adenoma and sellar meningioma.
2015;157: 231-233[PMID: 25416401 DOI: 10.1007/s00701-014-2268-5]
49 Ruiz-Juretschke F,Iza B,Scola-Pliego E,Poletti D,Salinero E.Coincidental pituitary adenoma and planum sphenoidale meningioma mimicking a single tumor.
2015;62: 292-294[PMID: 25963837 DOI:10.1016/j.endonu.2015.03.003]
50 Ben Nsir A,Khalfaoui S,Hattab N.Simultaneous Occurrence of a Pituitary Adenoma and a Foramen Magnum Meningioma: Case Report.
2017;97: 748.e1-748.e2[PMID: 27989978 DOI:10.1016/j.wneu.2016.10.108]
51 Lim KZ,Goldschlager T,Chandra RV,Hall J,Uren B,Pullar M.Co-occurrence of Pituitary Adenoma with Suprasellar and Olfactory Groove Meningiomas.
2016;7: 361-365[PMID: 27872697 DOI:10.15412/J.BCN.03070409]
52 Herrero-Ruiz A,Villanueva-Alvarado HS,Corrales-Hernández JJ,Higueruela-Mínguez C,Feito-Pérez J,Recio-Cordova JM.Coexistence of GH-Producing Pituitary Macroadenoma and Meningioma in a Patient with Multiple Endocrine Neoplasia Type 1 with Hyperglycemia and Ketosis as First Clinical Sign.
2017;2017: 2390797[PMID: 29225978 DOI: 10.1155/2017/2390797]
53 Kumaria A,Scott IS,Robertson IJ.An unusual pituitary adenoma coexistent with bilateral meningiomas: case report.
2019;33: 579-580[PMID: 28961022 DOI: 10.1080/02688697.2017.1386283]
54 Zhao Y,Zhang H,Lian W,Xing B,Feng M,Liu X,Wang R.Collision tumors composed of meningioma and growth hormone-secreting pituitary adenoma in the sellar region: Case reports and a literature review.
2017;96: e9139[PMID: 29390316 DOI: 10.1097/MD.0000000000009139]
55 Engelhardt J,Nunes ML,Pouchieu C,Ferrière A,San-Galli F,Gimbert E,Vignes JR,Laurent F,Berge J,Baldi I,Tabarin A,Loiseau H.Increased Incidence of Intracranial Meningiomas in Patients With Acromegaly.
2020;87: 639-646[PMID: 31625569 DOI: 10.1093/neuros/nyz438]
56 Pravdenkova S,Al-Mefty O,Sawyer J,Husain M.Progesterone and estrogen receptors: opposing prognostic indicators in meningiomas.
2006;105: 163-173[PMID: 17219818 DOI: 10.3171/jns.2006.105.2.163]
杂志排行

World Journal of Clinical Cases的其它文章
- Capillary leak syndrome:A rare cause of acute respiratory distress syndrome
- lmproving outcomes in geriatric surgery:ls there more to the equation?
- Mass brain tissue lost after decompressive craniectomy:A case report
- Primary intracranial extraskeletal myxoid chondrosarcoma:A case report and review of literature
- Spinal canal decompression for hypertrophic neuropathy of the cauda equina with chronic inflammatory demyelinating polyradiculoneuropathy:A case report
- Enigmatic rapid organization of subdural hematoma in a patient with epilepsy:A case report