Unusual cause of hemorrhagic pleural effusion: A case report
2022-06-07KeeTatLeeKarNimLeongTingSooChowPengShyanWong
Kee Tat Lee, Kar Nim Leong, Ting Soo Chow, Peng Shyan Wong
Kee Tat Lee, Department of Medicine, Hospital Sultanah Bahiyah, Alor Setar 05460, Kedah,Malaysia
Kar Nim Leong, Ting Soo Chow, Peng Shyan Wong, Infectious Disease Unit, Department of Medicine, Hospital Pulau Pinang, Georgetown 10990, Pulau Pinang, Malaysia
Abstract BACKGROUND Infected aortic aneurysms are uncommon and difficult to treat. We present a case of infected aortic aneurysm with recurrent nontyphoidal Salmonella bacteremia.CASE SUMMARY A 68-year-old gentleman presented with non-specific symptoms and was found to have nontyphoidal Salmonella bacteremia and was treated with intravenous ceftriaxone. However his condition did not improve, and he developed a multiloculated right pleural effusion. Thoracocentesis was done to drain hemorrhagic pleural fluid. Chest computed tomography demonstrated descending thoracic aorta saccular aneurysm with periaortic hematoma likely due to recent bleed and extending to the right pleural cavity. He was referred to cardiothoracic surgery team and was planned for medical therapy in view of hemodynamic stability and no evidence of active leakage. He completed intravenous antibiotic for 5 wk and refused surgical intervention. Unfortunately, he was admitted twice for recurrent nontyphoidal Salmonella bacteremia. Finally, he agreed for surgical intervention and underwent endovascular aortic repair 3 mo later. Postoperatively, his condition remained stable with no recurrence of infection.CONCLUSION Our case highlights the importance of high index of suspicion of infected aortic aneurysm in patients with Salmonella bacteremia with high-risk factors such as atherosclerosis.
Key Words: Infected aneurysm; Aorta; Nontyphoidal Salmonella; Pleural effusion; Case report
lNTRODUCTlON
Infected aneurysm is a rare disease associated with significant morbidity and mortality. Initial symptoms are non-specific, and due to lack of conclusive signs and symptoms, patients are often subjected to various investigations until a diagnosis is made. Standard treatment consists of antibiotic therapy and open surgery with surgical debridement and vascular reconstruction. However, there are no clear guidelines or randomized controlled trial on the best approach for the management of this condition. We report a patient with nontyphoidalSalmonellainfected aortic aneurysm who was treated with medical therapy initially and complicated with recurrence. He was successfully treated with endovascular aortic repair and was well during follow-up with no recurrence of infection. Relevant literature is reviewed.
CASE PRESENTATlON
Chief complaints
A 68-year-old man presented to our hospital with fever associated with lethargy, reduced oral intake,and dyspnea.
History of present illness
The patient’s presenting symptoms had lasted for 1 wk.
History of past illness
His medical illness includes diabetes mellitus, hypertension, ischemic heart disease, and chronic kidney disease.
Personal and family history
No relevant family history.
Physical examination
He was febrile and required the support of face mask oxygen during presentation. Examination revealed reduced air entry over right lower zone with bilateral lower zone crepitations.
Laboratory examinations
Laboratory results showed white blood cell count of 16 × 109/L, hemoglobin level of 8.3 g/dL, urea 16.9 mmol/L, and creatinine 301 μmol/L.
Imaging examinations
Chest X-ray on admission showed blunted right costophrenic angle (Figure 1).

Figure 1 Chest X-ray on admission showed right pleural effusion.
PROGRESS
He was admitted to the medical ward with the diagnosis of pneumonia and acute on chronic kidney disease. He was started on intravenous (IV) ceftriaxone 2 g daily. Blood culture on admission was positive for nontyphoidalSalmonella spp. During the course of admission, he became more tachypneic,and right thoracocentesis was done in view of worsening pleural effusion, which drained out 250 mL of blood stained fluid. Lung ultrasound showed multiseptated right pleural effusion. Despite ultrasound guided pigtail drainage of right pleural effusion, his condition did not improve. Chest computed tomography (CT) demonstrated descending thoracic aorta saccular aneurysm with periaortic hematoma(Figure 2), likely due to recent bleed, and extending to the right pleural cavity. Pleural fluid culture was negative.
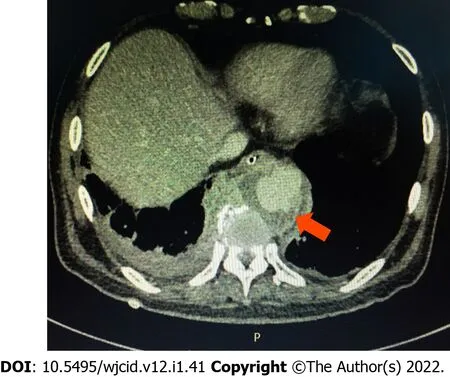
Figure 2 Chest computed tomography showed descending thoracic saccular aneurysm with periaortic hematoma (arrow).
FlNAL DlAGNOSlS
Salmonellainfected aortic aneurysm.
TREATMENT
He was referred to cardiothoracic surgery team and was planned for medical therapy in view of hemodynamical stability and no evidence of active leakage. There were multiple changes in his antibiotics regimen due to persistent fever (which included ceftazidime, piperacillin-tazobactam,meropenem, and cefepime). He completed 5 wk of antibiotics and was planned for a CT angiography of aorta at a later date to decide on surgical intervention.
OUTCOME AND FOLLOW-UP
Unfortunately, the patient was readmitted 2 mo later with abdominal discomfort and unable to pass motion for 1 wk. Abdominal X-ray demonstrated dilated large intestine. CT abdomen and pelvis showed descending thoracic aorta saccular aneurysm (slightly larger) with features suggestive of superimposed infection of periaortic hematoma; size of aneurysm: 2.4 cm × 3.6 cm and fecal laden bowels with features of impending intestinal obstruction. No obvious bowel related mass was seen. He was treated conservatively for the ileus, which resolved after 1 d. Blood culture on this admission was positive again for nontyphoidalSalmonella spp. Echocardiogram did not show any vegetations. He completed 6 wk of IV ampicillin and was discharged well. A repeated CT scan after 2 mo showed resolved periaortic hematoma; however, the patient refused surgical intervention and was given lifelong prophylactic oral antibiotic. Unfortunately, patient presented again with second recurrence after 1 mo, and blood culture was positive again for non-typhoidalSalmonella.He completed IV antibiotic and finally agreed for surgical intervention. He underwent endovascular aortic repair, and his condition remained stable with no recurrence of infection during his last follow-up after 2 years.
DlSCUSSlON
Infected aneurysm is a serious clinical condition. The term mycotic aneurysm was first described by William Osler in 1885[1], however the nomenclature of mycotic aneurysmvsinfected aneurysm remains controversial as a majority of infected aneurysms are due to bacterial infection. Etiology of infected aneurysm includes direct bacterial inoculation, bacteremic seeding of existing intimal injury, atherosclerotic plaque, or preexisting aneurysm, contiguous infection, or septic emboli from heart, which can occlude vasa vasorum of blood vessel and lead to infected aneurysm.
Infected aortic aneurysm is a rare but life-threatening condition with devastating outcomes. Initial clinical presentations are often non-specific; therefore, misdiagnosis is common. Infected aortic aneurysms may manifest as vague pain at the back, chest, or abdomen. Some patients may present as pyrexia of unknown origin and remain undiagnosed until rupture of aneurysm. In our patient, he was only diagnosed with infected aortic aneurysm after 3 wk of admission.
Salmonellaspecies andStaphylococcus aureusare the most common pathogens of infected aortic aneurysm, followed by other organisms such asStreptococcispecies,Treponema pallidum, andMycobacterium spp[2-4]. In East Asia, gram negative bacteria related infected aortic aneurysm is more prevalent,whereSalmonellaspecies are the most common organisms[2,3,5,6]. It is important to obtain a microbiological diagnosis given the need for protracted courses of antimicrobial therapy. However, blood cultures are negative in around 50% of cases[5,7,8]. Initial empirical treatment is often required and guided by the most likely infecting organism according to the individual and clinical circumstances. It is also prudent to use antibiotics judiciously as prolonged broad spectrum antibiotics may lead to development of antimicrobial resistance.Salmonellahas a strong affinity for large blood vessels and can easily adhere to the damaged vascular wall, strongly affecting the natural course of the disease.However, studies showed that non-Salmonellainfections are associated with higher aneurysm-related complications and mortality after treatment[9].
The study by Oderichet al[10], with 43 patients with infected aortic aneurysm, found that the risk factors of aneurysm-related death were extensive periaortic infection, female gender,Staphylococcus aureusinfection, aneurysm rupture, and suprarenal aneurysm location. Another larger series done in Taiwan reported that the independent predictors of aneurysm-related death were advanced age, non-Salmonellainfection, and non-surgical treatment[2].
Until now, there are no randomized clinical trials to guide the management of infected aneurysm.Therapy mainly includes the control of infections by antibiotic and surgical debridement with or without reconstruction of arterial circulation. Management strategies are primarily based upon clinical experience guided by case series. The optimal duration of antibiotic therapy remains inconclusive. Most studies recommend at least 6 wk of antibiotic and stopping only when there is no longer clinical and laboratory evidence of ongoing sepsis[11,12].
Medical therapy alone is associated with devastating outcomes, with in-hospital mortality of 50%[13]. Since infected aortic aneurysm is at high risk of rupture, surgical treatment is encouraged in the absence of absolute contraindications. Open surgery with extensive debridement of infected tissue andin situor extra-anatomical reconstruction has been the gold standard treatment. However, it is associated with high risk of morbidity and mortality[3,14-16]. Recently, endovascular techniques has become an emerging treatment alternative, especially in the treatment of patients at prohibitive risk for open surgery. Few studies have shown that endovascular treatment of infected aortic aneurysm is feasible and that it is a durable treatment option for high risk patients[17,18]. Luoet al[18] reported that survival at 1 mo, 6 mo, 1 year, and 5 year was 90%, 82%, 71%, and 53%, respectively. In addition, a European multicenter study of endovascular treatment for infected aortic aneurysm also showed similar results[17].
CONCLUSlON
Infected aortic aneurysm is a rare clinical entity with high mortality. Due to non-specificity of the early symptoms, misdiagnosis is common. Our case highlights the importance of high index of suspicion of infected aortic aneurysm in patient with recurrent nontyphoidalSalmonellabacteremia. Endovascular technique has become an emerging treatment option.
ACKNOWLEDGEMENTS
We thank the Director-General of Health Malaysia for the permission to present these findings.
FOOTNOTES
Author contributions:Lee KT, Chow TS, and Wong PS were involved in data analysis; Lee KT, Leong KN, Chow TS,and Wong PS contributed to conception of the study and drafting, critically revising, and providing final approval of the manuscript.
lnformed consent statement:Written consent for publication has been obtained from the patient.
Conflict-of-interest statement:The authors declare that there is no conflict of interest.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016) and the manuscript was prepared according to the checklist.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Malaysia
ORClD number:Kee Tat Lee 0000-0003-3638-2541; Kar Nim Leong 0000-0002-0175-6059; Ting Soo Chow 0000-0001-6175-1818; Peng Shyan Wong 0000-0003-1913-6648.
S-Editor:Wang LL
L-Editor:Filipodia
P-Editor:Wang LL
