Effects of mindfulness meditation on trait mindfulness, perceived stress,emotion regulation,and quality of life in hemodialysis patients:A randomized controlled trial
2022-05-10HossamAlhawatmehSamiAlshammariJehadRababah
Hossam Alhawatmeh, Sami Alshammari, Jehad A.Rababah
College of Nursing, Jordan University of Science and Technology, Irbid, Jordan
Keywords:Chronic kidney failure Emotional regulation Meditation Mindfulness Psychological stress Quality of life Renal dialysis Kidney diseases
ABSTRACT Objective: This study aimed to examine the effects of mindfulness meditation on trait mindfulness,perceived stress, emotion regulation, and quality of life in end-stage renal disease patients undergoing hemodialysis.Methods: An experimental study with repeated measures design was conducted among a sample of 74 end-stage renal disease patients undergoing hemodialysis between January and May 2021 in the dialysis center at Jahra hospital, Kuwait.The patients were randomly assigned to the experimental (n =37) and control groups(n =37).The experimental group participated in 30-min mindfulness meditation sessions(three sessions a week for five weeks) held during their hemodialysis sessions; the participants in the control group were instructed to sit with their eyes closed and relaxed for 30 min three times a week for five weeks during hemodialysis sessions.The dependent variables of both groups were measured at baseline (T0), middle of intervention (T1), and end of intervention (T2) using the Mindful Attention Awareness Scale (MAAS), Perceived Stress Scale (PSS), Emotion Regulation Questionnaire (ERQ), and Kidney Disease Quality of Life (KDQOL-36) questionnaire.The study was registered in the ClinicalTrial.gov (Identifier: NCT05176730).Results: The repeated measures ANOVA(within-subject)results for the experimental group showed that mindfulness meditation had significantly decreased perceived stress by the end of the intervention.Also,mindfulness meditation improved mindfulness, emotion regulation, and kidney disease-related quality of life in the experimental group, and this improvement occurred significantly at both T1 and T2.The repeated measures ANOVA(within and between-subject)results showed that the experimental group,as compared to the control group, had lower perceived stress, higher trait mindfulness, higher emotional regulation, and higher kidney disease-related quality of life over time.Conclusions: The positive findings of this study offer health policy-makers and hospital administrators a promising tool to use with patients undergoing hemodialysis as a way to manage stress and improve quality of life.However,this study should be replicated in multiple settings with follow-up assessments.
What is known?
· End-stage renal disease(ESRD)has been reported to be a major cause of disability and increased mortality worldwide.
· Hemodialysis, in addition to the signs and symptoms of ESRD,were reported as sources of stress, resulting in diminished health-related quality of life.
· Mindfulness meditation has been found to be highly effective for a variety of health outcomes in several psychiatric and medical illnesses.
· Few study has examined the effectiveness of mindfulness-based interventions among ESRD patients undergoing hemodialysis in Arab countries such as Kuwait.
What is new?
· The findings of the current study generally provided preliminary evidence about the effectiveness of mindfulness meditation as a coping tool for end-stage renal disease patients undergoing hemodialysis to manage stress and quality of life in Kuwait.
· Mindfulness meditation decreased perceived stress and increased trait mindfulness, emotion regulation, and quality of life in ESRD patients receiving hemodialysis.
· The findings of the current study added new preliminary evidence to the stress/coping field that could be used to guide hemodialysis-related clinical practice,education,and healthcare policies in Kuwait and other countries.
1.Introduction
End-stage renal disease(ESRD)has been reported to be a major cause of disability and increased mortality worldwide.In patients with ESRD, hemodialysis is a critically vital therapy that prolongs survival through the excretion or removal of poisonous metabolic waste from the human body [1].However, compliance with treatment has been found to be poor among ESRD patients [2].Such incompliance can be attributed to the different sources of stress associated with hemodialysis, including hemodialysis complications, time-consuming treatment schedules, restriction of dietary and fluid intake, and prescription of multiple medications [3,4].These sources of stress, in addition to the signs and symptoms of ESRD, result in diminished health-related quality of life, which is associated with increased risks of morbidity, mortality, and incompliance with hemodialysis therapy [3,5].
Despite the significant physical, emotional, and social burdens of stress, stress-reduction strategies have been inadequately used in patients undergoing hemodialysis.This may be contributed to the small-scale studies on psychotherapies with variable and holistic outcomes and the limited availability of evidenced-based coping interventions that are significantly supported [6].Mindbody therapies, which comprise a variety of techniques that increase the capacity of the mind to influence the functions of the body using emotional strategies,have gained increasing popularity worldwide in recent years.Evidence shows that mind-body therapies are affordable, easily-practiced, and safe, and that they improve perceived stress, health-related outcomes, and quality of life among various community-dwelling and clinical populations[7,8].One of the most popular mind-body therapies in the literature is mindfulness meditation, which has been found to be a feasible,beneficial,and well-tolerated therapy in hemodialysis patients[6].
It is theoretically claimed that mindfulness meditation can positively impact perceived stress, known also as stress appraisal,and quality of life through the improvement of trait mindfulness and emotion regulation [9].When faced with a situation, such as hemodialysis,patients with ESRD appraise whether this situation is stressful or not[10].Cognitive appraisal of stress is divided into the primary and secondary appraisal.The primary appraisal involves appraising whether the situation is a loss, threat, challenge, or uncontrollable.Hemodialysis is usually appraised as a threatening,uncontrollable situation since patients have no choice but to undergo hemodialysis on a regular basis for their entire lives for survival [10].Secondary cognitive appraisal of stress involves appraising and determining the available internal and external coping resources that enable patients to control and manage a stressful situation (e.g., continuous hemodialysis).Lack of coping resources may increase patients’ perceived stress, consequently threatening physical and social health status and inducing psychological maladaptation.Thus, modifying patients’ secondary cognitive appraisal by increasing their coping resources may enable them to manage the perceived stress induced by hemodialysis[10].
Coping resources are often classified into four types, including physical,environmental,materialistic,and psychological resources.Specifically,psychological coping resources are usually used to cope effectively with an unavoidable situation such as hemodialysis.Mindfulness mediation is a psychological coping resource that can relieve stress and the corresponding physical, psychological, and social reactions, threatening quality of life [10].Mindfulness meditation cultivates and improves the natural mental capacity to pay attention to, be aware of, and accept current experiences in a non-judgmental way [11].The developed capacity of mindfulness enables patients to acknowledge and accept their overwhelming current experience of hemodialysis, even if this experience is uncomfortable.In addition, it allows patients to be aware of their responses to senses, emotions, and thoughts, which enable effective self-management and problem-solving abilities [10].It also helps them to not engage in judgmental or negative thinking or avoidance of the hemodialysis-related experiences,resulting in less reactivity to stressful situations such as emotional, physical, and social reactions [9,10].
Research supports these theoretical claims, whereby mindfulness meditation has been found to be highly effective for a variety of health outcomes in several psychiatric and medical illnesses[7,8].For patients undergoing hemodialysis specifically,few studies conducted in Western and Asian countries have demonstrated that mindfulness meditation significantly improves trait mindfulness[12,13], stress symptoms [13,14], emotion regulation [15], and quality of life [14].However, these studies suffer from using very small sample sizes (e.g., 15 to 36 participants) or/and quasiexperimental designs, limiting validity [12-15].The current study addressed these issues as a randomized controlled design and a power analysis to calculate the required sample size were used.Even though evidence-based recommendations support the use of theory-based approaches for developing and delivering interventions [16], the existing studies have not taken in consideration this aspect.Theories can help identify the components and duration of intervention and decrease variations in the delivery of intervention [16].Therefore, the development of the intervention protocol in the current study was based on the ABC Relaxation Theory (Smith, 2005), which suggests a standardized and empirically tested version of mindfulness meditation[17].Moreover,few study has examined the effectiveness of mindfulness-based interventions among ESRD patients undergoing hemodialysis in Arab countries such as Kuwait.Therefore, any generalization of these previous study findings to other hemodialysis patients of different cultures such as ESRD patients in Kuwait is limited due to the different belief systems and self-care practices of these cultures.Thus,the current randomized controlled trial aimed to examine the effects of a standardized version of mindfulness meditation on trait mindfulness, perceived stress, emotion regulation, and healthrelated quality of life in ESRD patients undergoing hemodialysis in Kuwait.
Theoretically, investigating the effects of mindfulness meditation on the selected variables may provide insight into the mechanisms through which mindfulness meditation impacts the quality of life in hemodialysis patients.The current study findings may enrich the body of knowledge on mindfulness meditation and bridge the gap in the literature regarding the effects of mindfulness meditation on patients receiving hemodialysis.Practically, the findings of the present study may provide a basis for decisionmakers in adopting mindfulness meditation in Kuwaiti hospitals.
2.Method
2.1.Design
This study used a repeated-measures, randomized, parallel,control design and was conducted between January and May 2021 in the dialysis center at Jahra Hospital, Kuwait.The recruitment took approximately ten weeks, and the data collection and intervention took approximately six weeks.Seventy-four ESRD patients undergoing hemodialysis were recruited using convenience sampling.Jahra Hospital is a governmental hospital with one of the biggest dialysis centers in Kuwait, with a female ward, male ward,and isolation ward.The center holds 70 dialysis machines/beds,with an average number of 30 patients managed per day.The inclusion criteria for participation in this study were being a patient with ESRD undergoing hemodialysis three times a week, being aged 18 years old or over,and being able to read and write in Arabic.The exclusion criteria included being a patient with cognitive dysfunction or mental retardation, taking psychopharmacological drugs, or undergoing psychotherapy.The trial is reported in accordance with the CONSORT guideline.
The required sample size was calculated using G-power version(3.1).Given a mixed-design (within groups and between groups)repeated measures ANOVA, power of 0.95, moderate effect size of 0.25, and α of 0.05, the required sample size was 44 subjects.In a similar study, an attrition rate of 60% was reported [17].Considering an expected attrition rate of 60%,26 subjects should be added.Thus, the final required sample size was 70 participants.
2.2.Data collection instruments
The study data were collected using an Arabic self-report questionnaire with five parts.
2.2.1.Demographic characteristics
This section included a question for each variable: Age,gender,employment status, nationality, family status, and educational levels.
2.2.2.Trait mindfulness
Mindfulness is defined as open or receptive awareness of and attention to what is taking place in the present [18].An Arabic version of the Mindful Attention Awareness Scale(MAAS)was used to measure trait mindfulness [19].The MAAS is one-dimensional and comprises 15 items measured on a 6-point Likert-type scale ranging from 1(almost always)to 6(almost never).The score range is between 15 and 90,with higher scores indicating higher levels of trait mindfulness.The original scale has shown strong psychometric properties when validated among college students.The scale showed single-factor construct and a Chronbach’s α value of 0.82 among a sample of university students [18].Correlational,quasi-experimental, and laboratory studies have shown that the MAAS taps a unique quality of consciousness that is related to,and predictive of,a variety of self-regulation and well-being constructs[18].The Arabic MAAS has been shown to have excellent internal consistency and convergent validity among an Arab population[19].In our study,Chronbach’s α coefficient for the MAAS was 0.93.
2.2.3.Perceived stress
The Arabic version of the Perceived Stress Scale (PSS)was used to measure the degree to which situations in one’s life are appraised as stressful (unpredictable, uncontrollable, or overloaded)[20].The scale comprises ten items which are measured on a 5-point Likert scale (0 =never, 4 =very often) and which are relatively free of content specific to any subpopulation group.The total possible score ranges from 0 to 40, with higher scores indicating higher levels of perceived stress (stress appraisal) [21].The PSS has been validated for use among college students.The internal consistency coefficient for the PSS is 0.84 and the scale’s test-retest reliability is 0.85 [21].The Arabic PSS has been shown to have adequate reliability and validity and is considered a suitable instrument for assessing perceived stress in Arab people [20].The Chronbach’s α coefficient for the PSS was 0.82.
2.2.4.Emotion regulation
Emotion regulation is defined as the processes by which individuals influence which emotions they have and how they experience and express these emotions[22].The Arabic version of the Emotion Regulation Questionnaire (ERQ) was used to assess emotion regulation among the study sample [23].The questionnaire items are scored on a 7-point Likert-type scale ranging from 1(strongly disagree) to 7 (strongly agree) and are divided into two subscales, namely cognitive reappraisal and expressive suppression.Higher scores indicate greater emotion regulation abilities[23].The Arabic version of the ERQ has shown valid and reliable results among the Arab population[23].In our study,Chronbach’s α coefficient for the ERQ was 0.81.
2.2.5.Quality of life
The Arabic version of the Kidney Disease-Quality of Life questionnaire (KDQOL-36) is used to assess kidney disease-related quality of life and consists of four subscales: Generic Core [Physical Component Summary (PCS,12 items) and Mental Component Summary (MCS, 12 items)]; Symptoms/Problems (12 items);Burden of Kidney Disease(4 items),and Effects of Kidney Disease(8 items) [24].The scores of the different subscales are calculated according to the KDQOL-36 scoring system.Raw, pre-coded numeric values for each item are transformed linearly to a range of 0-100, with higher scores reflecting better kidney diseasequality of life [25].The Arabic version used in this study showed good psychometric qualities among Arab patients with chronic renal failure[24].In our study,the Chronbach’s α values for KDQOL-36 was 0.93.
2.3.Intervention
2.3.1.Experimental group
The experimental group received the Smith’s version of mindfulness meditation [26], which is a standardized theory-based intervention found to be effective in improving stress and its related health problems.Smith’s version of mindfulness meditation[26]comprises the following components.
(1) Being mindful of breathing,which includes easily taking in a full,deep breath,filling the lungs,simply exhaling,and then breathing naturally.It also includes noticing and simply attending to the air as it flows in and out of the nose and moves deeper into the throat and lungs (5 min).
(2) Being mindful of the body,which includes attending to how the body feels from head to toes and noticing any sensations that come and go.Upon noticing a sensation, the individual must gently note it,let it go,and continue attending to how the body feels (5 min).
(3) Being mindful of thought, which includes attending to the mind as thoughts come and go.Whenever a thought or feeling comes to mind,the individual should just notice it,let it go,and continue attending to the mind repeatedly(5 min).
(4) Being mindful of sounds, which includes attending to the sounds one hears, without thinking about them.The individual must gently notice the sound, let it go, and continue waiting (5 min).
(5) Being mindful of taste, which includes imagining a wonderful bowl of pieces of one’s favorite fruit and simply attending to a taste sensation, without thought, analysis, or effort (5 min)
(6) Full meditation,includes gently opening one’s eyes and being mindful of the world of the moment, quietly attending, and waiting.When noticing something, be it a sight, sound,thought,or sensation,the individual must let it go and then resume attending, doing nothing else, and waiting for what comes next (5 min).
The experimental group received 30-min individually administered, guided, chairside interventions during their hemodialysis sessions.This protocol has been found to be feasible and effective for patients undergoing hemodialysis [6].Smith (2005) explained in his ABC relaxation theory that at least two and preferably five weekly 30-min sessions of actual training of mind-body therapies should be provided to evoke relaxation,relieve stress,and improve health in general populations.However,for hemodialysis patients,it has been suggested that brief program formatting with at least 400 total minutes may lead to greater health benefits [17].Accordingly,the experimental group received 30-min mindfulness meditation sessions three times a week for five weeks (450 min).
The participants also received a 2-h foundation course which was introduced and supervised privately by one of the study researchers prior to the actual training sessions at a room in the dialysis center and which taught the participants the intervention basics, benefits, protocol, and method of access.To ensure the consistent delivery of the intervention,the researcher recorded the intervention instructions in Arabic based on the Smith (2005)protocol and sent the audio-recorded instructions to the participants via WhatsApp or email.The audio-recorded intervention contents were validated by two psychologists and experts in meditation.The recorded intervention instructions were accessed by the participants during the sessions using their cell phones and headsets, as recommended [17].The intervention delivery using audio-recorded instructions allowed the researcher to introduce the individual intervention sessions for up to five participants simultaneously.
The researcher responsible for supervising the intervention delivery was an advanced nursing specialist with six years of nephrology nursing experience and a 4-day training course on mindfulness meditation.This researcher attended the sessions to manage any potential interruptions (e.g., machines’ peeps and interruptions)and evaluate the intervention delivery and compliance using checklists produced according to Smith’s protocol [17].The researcher completed the checklist after each session by asking the participants whether they completed all intervention protocol.
If the participants felt discomfort, nausea, headache, muscle tension or any other uncomfortable symptoms during or immediately after the intervention sessions, the researcher informed the participants to stop the intervention to seek and provide the appropriate healthcare.
2.3.2.Control group
The participants in the control group were instructed to sit with their eyes closed and relaxed for 30 min three times a week for five weeks during hemodialysis sessions to control for the nonspecific effects of social interaction and environment [27].The timings of the control group sessions were similar to those of the experimental group,whereby if a given experimental group intervention lasted for 30 min,the control group participants would be asked to sit with their eyes closed and relax for 30 min also.
The participants’ privacy and confidentiality were maintained where nobody was able to attend the data collection and intervention sessions.To avoid contamination bias, the participants in the experimental group were asked not to share any information related to the intervention with others during the study.Also, the nurses and physicians working in the hemodialysis centers were not given any detailed information about the intervention of the experimental group and would not pass any information about the intervention to the participants in the control group.At the end of intervention, the participants in the control group confirmed that they had not practiced or received any information about mindfulness meditation during the study when they were asked about that by the researcher who supervised the intervention delivery.
2.4.Procedure
First,the permission from the instruments used in the study was obtained.Recruitment of participants was conducted by one of the study researchers(Alshammari S.),who supervised the delivery of intervention, after obtaining approval to conduct the study from the hospital administrators.The study purposes and protocol were explained to the patients in detail.Patients who agreed to participate in the study and met the eligibility criteria were asked to sign a consent form.Participants then completed the baseline measurements (T0) of the study variables using the self-report questionnaires with a research assistant having a bachelor nursing degree and 10 years of nephrology nursing experience.Another study researcher having a PhD degree, who was not involved in the recruitment process and data collection, randomized the participants to the experimental group (n =42) or the control group(n =42), using a simple 1∶1 computer-generated sequence.The study variables were measured two weeks post the start of the intervention (immediately after the sixth session, T1) and at the end of the final session(T2)for both groups.The measurements of the study variables at T0, T1 and T2 were conducted by the same research assistant who was not involved in any other parts of the study and blinded to randomization allocation.All measurements were privately taken at the dialysis center.
2.5.Data analysis
SPSS version 25 (SPSS Inc., Chicago, Illinois, USA) was used to analyze the collected data.Prior to the main analysis, outliers and missing data were examined and managed as appropriate.Then,the assumptions of the statistical tests used, normality using histogram graph, homogeneity of variance, and sphericity were checked and managed as appropriate.Mauchly’s test of sphericity is used to assess whether the sphericity assumption has been violated.When Mauchly’s test of sphericity was significant(P < 0.05), the degrees of freedom were corrected using Greenhouse-Geisser estimates of sphericity.The comparability of the two groups was evaluated in terms of demographic characteristics and the baseline measurements of the dependent variables using t-test and Chi square, based on the measurements of the dependent variables.The main analysis was conducted with repeated-measures ANOVA (mixed design: within and between groups).A P-value of 0.05 was set as the significance level for the main analysis tests.
2.6.Ethical considerations
The study proposal was approved by the Institutional Review Board at Jordan University of Science and Technology and the Kuwaiti Ministry of Health(Number of approval:78/136/2020).The study was conducted in accordance with the Declaration of Helsinki.The participants were asked to sign informed consent forms which included an explanation of the study purpose and protocol,in addition to a statement indicating that the participants had the right to refuse to participate or withdraw from the study at any time without consequences.The participants were assured that their information would not be made available to others without their consent.The study data were stored in a locked locker after all names were replaced by numbers.The study was registered in the ClinicalTrial.gov(Identifier: NCT05176730).
3.Results
3.1.Participants and sociodemographic characteristics
The study flow diagram shows the flow of participants through each stage of the randomized trial (Fig.1).Table 1 shows the demographic characteristics of the participants in the experimental and control groups and any significant group differences on demographic variables.
3.2.Effectiveness of mindfulness mediation
Scores of MAAS, PSS, ERQ and KDQOL-36 of the two groups at T0,T1,and T2 are shown in Table 2.At baseline(T0),independent t-tests were conducted to examine any pretest mean differences between the experimental and control groups based on the dependent variables.The results revealed no significant differences between the experimental and control groups on baseline PSS scores(t =1.117,P =0.268)and ERQ scores(t =-0.712,P =0.479).At the same time, there were statistically significant differences between the experimental and control groups on baseline MAAS scores (t =-2.267, P =0.026) and KDQOL-36 scores (t =-2.194,P =0.031), indicating that trait mindfulness and kidney diseasequality of life of the experimental were lower than those of the control group at baseline.
Table 2 shows the results of repeated measures ANOVA(withingroup) tests.In the experimental group, the results revealed that there were significant main effects of time for MAAS, ER, and KDQOL but a non-significant main effect of time for PSS.In the control group,the results showed that there were significant main effects of time for MAAS, ER, PSS, and KDQOL.Table 3 shows the results of analyses of variance on dependent variables across three repeated measures for two groups, with significant effects of time by condition interaction for MAAS, ER, PSS, and KDQOL of the two groups.
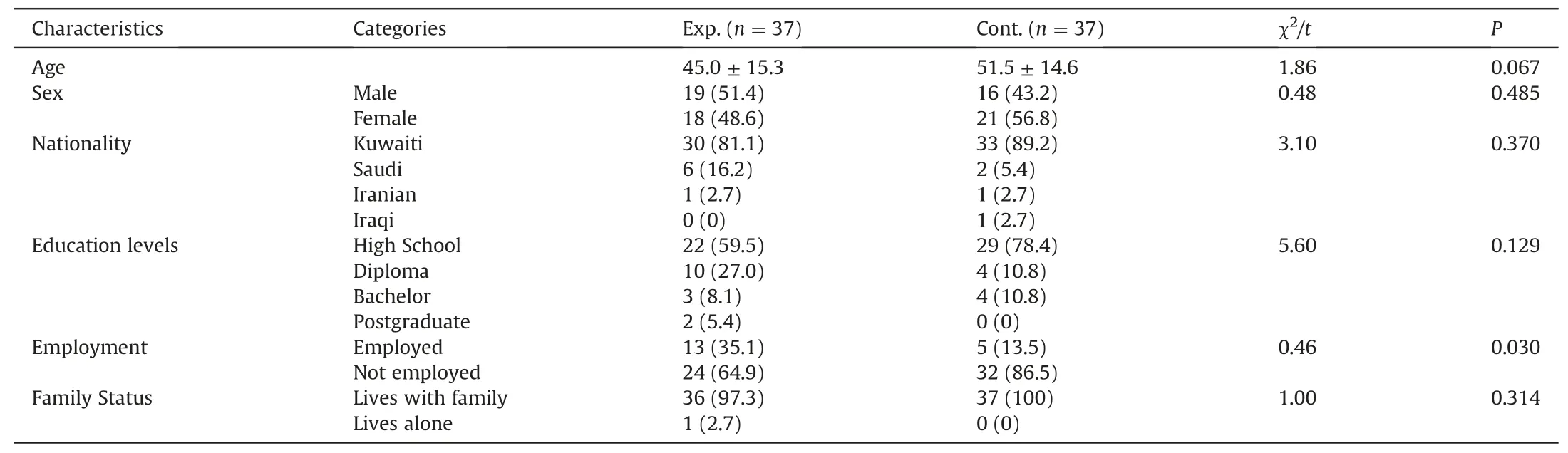
Table 1Demographic and clinical characteristics.

Table 2Results of repeated measures ANOVA (within-group)for experimental and control groups.

Table 3Analyses results of variance on dependent variables across three repeated measures by group(n =74).
4.Discussion
The current study results showed significant improvements in perceived stress, mindfulness, emotion regulation, and kidney disease-quality of life scores generally over time and at the end of the intervention.
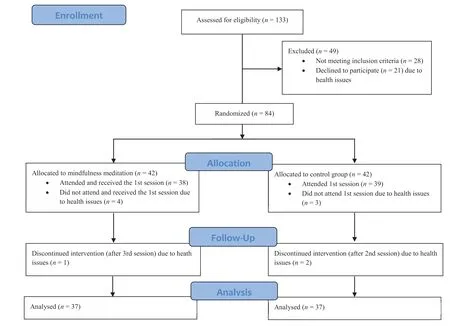
Fig.1. Study flow diagram for the study participants.
4.1.Trait mindfulness
In the current study, mindfulness meditation significantly increased MAAS scores over time in the experimental group, as compared to the control group.These findings are consistent with the findings of previous studies.Adamoli et al.(2021)found that in hemodialysis patients, an 8-week mindfulness-based intervention led to greater awareness of body sensations, emotions, and thoughts and greater acceptance of experiences, which are the main attributes of trait mindfulness [13].In a one-group quasiexperimental study, a mindfulness meditation intervention of 10-20-min sessions received during hemodialysis sessions,3 times a week over 12 weeks, increased mindfulness scores in hemodialysis patients[12].These results support the theoretical hypothesis claiming that repeated mindfulness-based practices can cultivate and improve the natural mental capacity of mindfulness, called trait mindfulness [9].
4.2.Perceived stress
In the current study, mindfulness meditation significantly decreased PSS over time in the experimental group compared to the control group.These findings are consistent with those of other studies.In a randomized controlled trial (RCT), patients with chronic renal failure who received an 8-week mindfulness-based intervention during their hemodialysis sessions showed reduced reactivity to stressful situations[13].Similarly, another RCT used a mindfulness-based stress reduction (MBSR) intervention, adapted to a workshop and teleconference format, and found the intervention feasible and effective in reducing symptoms of stress in patients waiting for kidney or pancreas transplant [14].These results support the theoretical claim that the developed mental capacity of mindfulness enables psychological distance and positive reappraisals, helping to stop initial automatic uncontrollable appraisals [9,10].
4.3.Emotion regulation
In the current study, mindfulness meditation significantly increased ER over time in the experimental group,as compared to the control group.These findings are consistent with previous study results.In a three-group pretest-posttest quasi-experimental study conducted among hemodialysis patients [15], the effectiveness of two months of practicing mindfulness therapy and memory specificity training in improving negative and positive cognitive emotion regulation was greater than the effectiveness of receiving usual care [15].It has been argued that mindfulness meditation targets the fundamental beliefs and negative thoughts of selfefficacy in patients.It helps hemodialysis patients to change their cognition and makes them aware of their own cognitive and emotional content, which then allows them to explore more appropriate alternatives and stop automatic reactions to stressful situations like hemodialysis [15].Also, it has been explained that mindfulness meditation can regulate amygdala functioning, a part of the brain limbic system which is responsible for regulating emotions,such as fear and aggression [28].
4.4.Kidney-disease quality of life
In the current study, mindfulness meditation significantly increased KDQOL over time in the experimental group, while compared with the control group who showed a decreased KDQOL over time.This comes in line with the results of other studies.In a previous RCT, an 8-week MBSR program delivered in a novel workshop-teleconference format, as compared to a telephonebased support group, was more effective in improving HRQOL in patients awaiting kidney transplantation[14].Another clinical trial demonstrated that eight sessions of mindfulness meditation, as compared to eight educational sessions on end-stage renal disease and hemodialysis,were more effective in improving general health.Mindfulness meditation has been found to decrease physical symptoms, anxiety, depression, sleep disorder, and social dysfunction [16].A previous experimental study examined the impacts of a mindfulness meditation intervention of 10 to 20-min sessions received during hemodialysis sessions, three times a week over 12 weeks,on physical and psychological health,the main components of HRQOL.The intervention was found to improve depressive symptoms,blood pressure values,self-compassion,and serum phosphorous levels[12].
While hemodialysis increases life expectancy, it poses for patients a wide range of physical, psychological, and social problems which lead to changes in their lifestyle and jeopardize their healthrelated quality of life over time.The participants in the control group showed a decreased quality of life over time.The findings of this study were consistent with a longitudinal study that showed that the physical and mental functioning of patients with hemodialysis decreased rapidly over time, attributed to increasing comorbidity [29].However, mindfulness meditation is designed to increase attention to the body and cultivate awareness of and decrease the automatic interaction of physical, cognitive, and emotional processes, jeopardizing the quality of life [9,10].
4.5.Limitations of the study
As a study to evidence the feasibility of mindfulness meditation and its effectiveness on some health outcomes in ESRD patients undergoing hemodialysis, there were some limitations.The use of convenience sampling to recruit a small sample from one setting limits the generalizability of the study findings.Therefore, it is recommended that future studies use randomized sampling methods to recruit larger samples from multiple settings.Further,the long-term effects of the intervention were not assessed, and thus, it is recommended that future studies include follow-up assessments.There were significant differences between the study groups regarding the pretest mean scores of trait mindfulness and KDQOL and employment status.These baseline differences may indicate that the simple random assignment method used in this study was not completely successful in equating the two groups on these variables at pretest.Nevertheless, the differences showed a better condition of the control group than the experimental group at baseline, which would not influence the explanation for the study results.It is recommended that future studies use more effective random assignment methods and procedures.Moreover,even though many techniques were used in this study to avoid contamination bias as mentioned previously, there was no guarantee that contamination would not be found since the participants in the two groups were recruited from the same setting.Thus,it is recommended that future studies use cluster random assignment methods preferably to avoid contamination bias [30].
4.6.Implications for clinical practice
The findings of the present study indicate that mindfulness meditation is generally effective in improving health outcomes,including perceived stress,trait mindfulness,emotional regulation,and health-related quality of life, among ESRD patients receiving hemodialysis in Kuwait.These positive findings offer a promising tool for patients undergoing hemodialysis as a way to improve their health and quality of life.Mindfulness meditation has been found to be a simple, feasible, and effective stress-reduction technique that can be taught to patients within 30 min [6,10].Thus, developing and incorporating mindfulness meditation training as a complementary treatment in the care plans of hemodialysis patients may improve the psychological, physical, and social health of these patients.
5.Conclusions
The findings of the current study generally provided preliminary evidence about the effectiveness of mindfulness meditation as a coping tool for end-stage renal disease patients undergoing hemodialysis to manage stress and health in Kuwait.This was evidenced by the decrease in perceived stress and increase in trait mindfulness, emotion regulation, and quality of life among the participants of experimental group by the end of the intervention.
Overall, the study findings add new knowledge to the stress/coping field that can be used to guide hemodialysis-related clinical practice, education, and healthcare policies in Kuwait and other countries.Further studies are needed to investigate the effects of mindfulness meditation on other non-tested health outcomes using random samples recruited from multiple settings, with the inclusion of follow-up assessments of these outcomes.
CRediT authorship contribution statement
Hossam Alhawatmeh:Conceptualization, Methodology, Investigation,Writing-review&editing,Project administration,Funding acquisition.Sami Alshammari:Conceptualization, methodology,Writing-original draft, Data curation, Resources, Investigation,Formal analysis, Visualization.Jehad A.Rababah:Forma analysis,Writing- review &editing.
Funding
This study received funding from Jordan University of Science and Technology, Deanship of Research.
Data availability statement
The study dataset and protocol are available upon reasonable request.
Declaration of competing interest
There is no actual or potential conflict of interest,including any financial, personal or other relationship with other people or organizations that could inappropriately influence,or be perceived to influence,our work.
Acknowledgement
The authors thank the participating hospitals,head nurses,and nurse participants for their assistance,as well as Jordan University of Science and Technology for funding the study.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2022.03.004.
杂志排行

International Journal of Nursing Sciences的其它文章
- Application of rational emotive behavior therapy in patients with colorectal cancer undergoing adjuvant chemotherapy
- The effect of slow deep breathing relaxation exercise on pain levels during and post chest tube removal after coronary artery bypass graft surgery
- The association between frailty of older stroke patients during hospitalization and one-year all-cause mortality:A multicenter survey in China
- Translation and piloting of the Chinese Mandarin version of an intensive care-specific pressure injury risk assessment tool (the COMHON Index)
- Adaptation and validation of pediatric peripheral intravenous catheter insertion and care practices audit tools
- Distress management in cancer patients:Guideline implementation based on CAN-IMPLEMENT