Application of rational emotive behavior therapy in patients with colorectal cancer undergoing adjuvant chemotherapy
2022-05-10YuxinLiuXioynNiRongWngHuiniLiuZifenGuo
Yuxin Liu , Xioyn Ni , Rong Wng , Huini Liu , Zifen Guo ,c,*
a School of Nursing, University of South China, Hengyang, Hunan, China
b Department of Internal Medicine-Oncology, The First Affiliated Hospital, University of South China, Hengyang, Hunan, China
c Institute of Pharmacy and Pharmacology, University of South China, Hengyang, Hunan, China
Keywords:Anxiety Adjuvant chemoradiotherapy Colorectal neoplasms Depression Patients Rational emotive behavior therapy
ABSTRACT Objective: This study aimed to explore the effects of our rational emotive behavior therapy (REBT)program on symptoms, anxiety, depression, and sleep state in patients with colorectal cancer (CRC)undergoing chemotherapy.Methods: From October 2020 to May 2021,fifty-six patients with CRC in a hospital in the Hunan Province were randomly divided into an intervention group(n =28)and a control group(n =28).The patients in the intervention group completed a 6-week REBT program based on routine nursing care,including four courses: 1) establish a relationship and formulate health files; 2) group communications and study symptom management; 3) continuously provide health knowledge and strengthen healthy behavior;and 4) review the treatment and summary.The control group maintained routine nursing care.The simplified Chinese version of the Memorial Symptom Assessment Scale Short Form (MSAS-SF-SC), the Hospital Anxiety and Depression Scale(HADS),and the Pittsburgh Sleep Quality Index(PSQI) scale were used to investigate and compare the intervention effects of the two groups at baseline (T1, before the intervention), four weeks (T2), and six weeks (T3) after the intervention.Results: The intervention group was significantly improved in symptoms,anxiety, depression, and sleep state, compared with the control group.At T2, MSAS-SF-SC (24.43 ± 4.26 vs.28.07 ± 3.91), symptom distress (17.29 ± 4.04 vs.19.39 ± 3.59), symptom frequency (7.14 ± 1.51 vs.8.68 ± 1.42), HADS(13.68 ± 3.38 vs.15.86 ± 3.79), anxiety (3.89 ± 1.85 vs.5.18 ± 2.18), and depression (9.79 ± 2.06 vs.10.68±2.23),showed that the difference between the two groups was statistically significant(P <0.05).At T3, MSAS-SF-SC (23.89 ± 3.54 vs.30.14 ± 3.94), symptom distress (17.61 ± 3.52 vs.21.32 ± 3.57),symptom frequency(6.29±1.49 vs.8.82±1.47),HADS(11.82±2.57 vs.16.29±3.13),anxiety(3.21±1.64 vs.5.61±1.77),and depression(8.61±1.52 vs.10.68±1.81),showed that the difference between the two groups was statistically significant (P <0.05).The sleep state of the intervention group was better than the control group at T3, with decreased score of PSQI [4.00 (3.00,8.00) vs.9.00 (7.00,12.50), Z =-3.706,P <0.001].Conclusion: The 6-week REBT program can effectively improve the symptom, anxiety, depression, and sleep state of patients with CRC undergoing chemotherapy, which could as a care plan for patients with CRC who are repeatedly admitted to the hospital for chemotherapy.
What is known?
· Chemotherapy is one of the main treatments for patients with colorectal cancer, and they are usually affected by the side effects of chemotherapy, resulting in physical and psychological symptoms.
· Effective psychosocial intervention is beneficial to patients with colorectal cancer.
What is new?
· Rational emotive behavior therapy has a positive effect on patients with colorectal cancer in this study.
· Rational emotive behavior therapy could be used as one of the potential nursing care plans for patients with colorectal cancer who are repeatedly admitted to the hospital for chemotherapy.
1.Introduction
Colorectal cancer(CRC)is the fourth most deadly cancer globally[1].Since the end of the 1990s, China has implemented several strategies for preventing and treating cancer,but the incidence and mortality of CRC have steadily increased[2,3].Chemotherapy is one of the main treatments for patients with CRC and can effectively destroy tumor cells.However, many studies have found that patients are affected by the side effects of chemotherapy after receiving clinical treatment.Physical symptoms and psychological problems are major concerns for CRC survivors[4].According to the study of Han et al.[4], CRC survivors were more likely to have mental health problems during adjuvant chemotherapy.Symptoms such as gastrointestinal dysfunction, fatigue, and peripheral neuropathy were commonly reported, and anxiety, depression, and other adverse emotions increase stress and severity of the symptoms.Moreover, many studies [4,5]have shown that anxiety and depression are closely related to the symptoms, and long-term negative emotions directly affect sleep quality.These problems will directly or indirectly affect the treatment and prognosis of patients with CRC [6]and lead to a reduction in quality of life,eventually increasing the risk of suicide [7].
To alleviate the above problems, various types of psychological interventions and exercises have been developed for patients with CRC.Past studies have found that long-term follow-up and shortterm health education intervention could effectively relieve anxiety and depression in patients with CRC and improve their quality of life [8].At the same time, telephone interviews, face-to-face meetings, and text messages have positive effects on emotion and behavior in patients with CRC [9].Although a series of psychological and behavioral interventions have been developed successively by scholars, there is no adequate theoretical basis for the implementation of chemotherapy in patients with CRC.Some findings[10]showed that cognitive behavior therapy(CBT)was effective for cancer patients.Rational emotive behavior therapy(REBT)is a form of CBT that is an effective psychological behavior intervention that uses professional communication and guidance to help people overcome their irrational beliefs and accompanying symptoms[11,12].It was reported that REBT intervention could efficiently relieve unhealthy behavior or anxiety in college students and improve overall health [13,14].
Additionally,REBT could affect psychological health through the belief establishment behavior change and ultimately improve treatment adherence of women infected with HIV/AIDS [15].Cognitive belief is a prerequisite for behavior change, including patients’ coping and emotional responses.The REBT recognizes,refutes, and changes these irrational beliefs to promote health.Although many studies have shown the effectiveness of REBT in psychology and behavior,there are only preliminary studies on this therapy in cancer patients, especially patients with CRC.Few relevant studies have explored the effects of REBT on symptoms, anxiety, and depression in patients with CRC during chemotherapy.
The main objective of our study was to confirm whether REBT has better effects on the symptoms,anxiety,depression,and sleep state of patients with CRC undergoing adjuvant chemotherapy than routine care and to provide an effective psychological and behavioral intervention for patients with CRC undergoing adjuvant chemotherapy.
2.Methods
2.1.Study design
The study was quasi-experimental with pre/post-assessments.Patients with CRC were randomly divided into the intervention and control groups.The control group received routine nursing care.The patients in the intervention group completed a 6-week REBT program based on routine nursing care.
2.2.Participants and setting
The study was conducted in the inpatient department of a hospital inHengyang,China,betweenOctober2020andMay2021.Allpatients with CRC were individually recruited at admission to participate in this study.All participants were required to meet the following requirements:1)were over 18 years old;2)had basic cognitive abilities without other primary tumors;3)had received at least two cycles of chemotherapy;4)had not participated in another program before;5)had no permanent stomas after the surgery;6)could skillfully use the WeChat app,and 7)agreed to participate.The exclusion criteria were as follows: 1) with other major diseases such as heart, lung, and kidney diseases;2)major change in illness or death in the middle of the study,and 3)contact interruption or withdrawal.
The sample size was calculated using the following formula:n1=n2=2[(Zα+Zβ)2σ2/d2].We set α =0.05,and β =0.1.According to the references,σ (population standard deviation) =3.99, d =4.The minimum sample size was calculated to be 21 people in each group.Considering a 10%-20% sample loss rate and the actual situation, a total of 60 patients were planned to be invited to participate, with 30 patients in each group.To improve participants’compliance, we presented each patient who participated in the entire study with a beautiful gift.
Randomization was performed by the date of hospitalization to avoid sample mixing.We recruited control patients between October 2020 and January 2021, and patients in the intervention group were recruited from February to May 2021.The participants were not aware of the intervention assignment.
2.3.Ethics approval
The scientific ethics committee of the University reviewed and approved this study (approval number: 2020-No.36).The study aim,methods,benefits/risks,and confidentiality of individual data were explained to the patients and their families,and their consent was obtained.
2.4.The intervention
The program was developed based on a review of the literature.Subsequently, two graduate nursing students conducted semistructured interviews with 12 patients who met the inclusion criteria to record their symptoms and psychological reactions during chemotherapy, in addition to what they hoped to receive from nurses and clinicians to improve the REBT program.Then,the graduate tutor held a 40-min expert meeting around the theoretical framework of the REBT,the semi-structured interviews’results,and combined with internet-based communication [16-18]to discuss and decide on the final intervention process.
In practice, three primary nurses who provided oncology care for more than five years were responsible for routine nursing care of two groups,and two clinicians with a Ph.D.were accountable for answering the subjects’ clinical questions.The implementation of REBT was conducted primarily by graduate nursing students under the direction of a psychologist.Before the intervention, three nurses,two clinicians,and two graduate nursing students received unified professional training by the investigator’s clinical mentor,who holds a master’s degree and over 20 years of clinical experience to ensure intervention consistency.The training contents included the study aim, study protocol and themes, theoretical knowledge,communication skills, and ethical principles.
2.4.1.The REBT group
2.4.1.1.Establish a relationship and formulate health files.The first period for the intervention group is establishing a relationship and formulating health files with a face-to-face and 30-min one-on-one interview performed in the first week.First,researchers established a healthy treatment relationship at the bedside and informed the patients of the main contents of the project and the estimated treatment time.Then,researchers provided a blank health file with three topics and asked patients to complete it: 1) What problems did you encounter in chemotherapy and what are the two main problems? 2) How did you solve it by yourself? 3) What are your desired goals according to the two problems? Next, information was exchanged on WeChat.The team’s paper health manual was distributed, including general knowledge of chemotherapy,chemotherapy for colorectal cancer, common symptoms and treatment methods, diet guidance, and exercise guidance.
2.4.1.2.Group communications and study symptom management.
The second step of the study includes group communications and symptom management in the second week.Two to four patients were organized in the department’s conference room to communicate and study at each session.First,a nurse and a clinician took approximately 20 min to explain the health manual’s contents in the last course to study symptom management jointly.Second,based on the REBT health files,the patients’typical problems(e.g.,chemotherapy compliance, common adverse reactions, exercise and diet suggestions, mental health, PICC catheter care) were evaluated and addressed at length by the primary nurse and clinician for about 20 min.Next, patients were encouraged to express their thoughts on the above issues, ensuring that they can distinguish between rational and irrational beliefs (for example,only porridge or a high-protein diet during chemotherapy,walking properly or staying in bed, etc.).The communications lasted approximately 10 min.After that,researchers distributed relaxation therapy diagrams covering abdominal breathing exercises and muscle relaxation techniques.
2.4.1.3.Continuously provide health knowledge and strengthen healthy behavior.The next period involves a course during WeChat interviews between the fourth and fifth weeks.First, researchers conducted one-on-one interviews with participants by voice chat on WeChat for approximately 30 min.Questions about the participants’ health conditions were asked and their problems were addressed, encouraging them to share their inner thoughts.For example,most patients mentioned the common dietary problems,whether drinking porridge can reduce nausea? Based on this, researchers would correctly answer this question as “soft food is conducive to digestion, but it could not meet the nutrition consumed by the body during chemotherapy.It is suggested that patients eat high calorie and high protein food as much as possible.”If patients mentioned that they were afraid that some meat(such as beef and pork)would affect their condition,researchers would use experiences of cancer survivors and other types of inspiration stories to convince them of the importance of an appropriate diet.
Meanwhile, researchers arranged homework at the end of the interviews.Researchers had prepared the relaxation therapy diagrams and a compressed package containing ten soft musical songs,such as Tiny Sunshine, Dear My Hometown, etc.Patients were suggested to relax or exercise more than three times a week, spend more than 60 min listening to music weekly, and record the frequency and duration of relaxation in the next two weeks.Additionally, researchers provided the hospital’s existing health education materials weekly(e.g.,PICC catheter care,diet guidance,exercise guidance, etc.) and reports of successful cases of cancer remission on WeChat to strengthen their health beliefs and confidence.
2.4.1.4.Review the treatment and summary.Finally,the review and summary are made in the sixth week of the study by a voice chat or face-to-face interview.We reviewed and commented on participants’ homework and encouraged patients to share their experience in the intervention process(Was the type and duration of the intervention comfortable? etc.).Subsequently, patients’ health problems and beliefs pre- and post-intervetion were compared to help patients realize the improvement during the six weeks and the capacities need to be strengthened.
2.4.2.The control group
During admission, primary nurses guided patients through the admissions process to help them adapt to the hospital environment as soon as possible, which took about 20 min.This included introducing the ward environment, living facilities, and the assigned clinician, etc.In the hospital, clinicians and nurses were responsible for patients’ treatment and nursing care.Before chemotherapy,primary nurses and clinicians informed the patients of chemotherapy drugs’ effects and adverse reactions and asked patients to sign the informed consent letter for intravenous chemotherapy.Primary nurses and clinicians provided comprehensive health education and guidance for patients at hospital discharge.The clinicians issued a discharge summary with precautions after discharge, including the next admission’s time, laboratory indicators to be paid attention to after discharge,medication, etc.Nurses provided oral health education for about 10 min,including PICC catheter care,diet,exercise guidance,etc.In addition, we offered the department’s telephone number to address patients’ problems during the treatment.
2.5.Data collection
Participants recruited were required to provide medical and sociodemographic data before the intervention.The following questionnaires were completed at different times: at the baseline before the intervention, patients’ symptoms, anxiety and depression, and sleep state were evaluated using the Simplified Chinese version of the Memorial Symptom Assessment Scale Short Form(MSAS-SF-SC),the Hospital Anxiety and Depression Scale(HADS),and the Pittsburgh Sleep Quality Index(PSQI)scale;at the 4th and 6th weeks of the intervention, patients’ symptoms, anxiety and depression were evaluated using the MSAS-SF-SC and the HADS;and at the 6th week of intervention, patients' sleep state was assessed by the PSQI.The researcher, with unified guidance,distributed the questionnaire.The researcher would help them to complete the written questionnaires one by one according to patients’ oral answers for those who could not be completed by themselves.All questionnaires were collected and checked immediately after completion, the deficiencies and omissions were promptly checked.
2.5.1.Simplified Chinese version of the Memorial Symptom Assessment Scale Short Form
Symptoms were evaluated using MSAS-SF-SC[19],which was translated and verified from the Memorial Symptom Assessment Scale(MSAS)[20].The scale is a self-rated questionnaire consisting of 2 dimensions, including symptoms of distress (28 items) and symptoms frequency (4 items).Each item of physical symptoms is scored from 0 to 4.Others are scored from 1 to 4.Higher scores indicate more severe distress.In this study, a total score ≤32 was classified as mild symptoms, 33-64 as moderate symptoms, and 65-128 as severe symptoms.The Cronbach’s α coefficient was 0.782-0.874,and the test-retest was 0.819-0.872[19].It was found that the MSAS-SF-SC had great validity and reliability for Chinese people.
2.5.2.Hospital Anxiety and Depression Scale
Anxiety and depression were evaluated using HADS[21],a selfrated questionnaire containing 14 items.Anxiety items consist of numbers 1, 3, 5, 7, 9, 11, and 13.The remaining numbers are the depression items.All of them are scored from 0 to 3.The higher the score,the greater the severity of anxiety and depression.The total scores 0-7 are rated as no negative emotion, 8-10 as a mild negative emotion, and 11-21 as a severe negative emotion.The Cronbach’s α coefficient was greater than 0.840[22].The scale has shown excellent reliability.
2.5.3.Pittsburgh Sleep Quality Index
Sleep state was evaluated using PSQI scale [23], with seven components consisting of 19 self-rated items.Each item is scored from 0 to 3.The higher the score is,the worse the sleep quality.The 7 component scores of the PSQI had an overall Cronbach’s α coefficient of 0.830[24].The Chinese verification results of the PSQI had a Cronbach’s α coefficient of 0.840, and individual items were strongly correlated between them,which showed good validity and reliability.
2.6.Statistical analysis
The collected data were analyzed using SPSS, version 26.0.Measurement data between two groups were compared using Chisquared tests, Fisher’s exact tests, or Independent-samples t-tests.The counting data are described by frequency and percentages.Normally distributed continuous variables were described as Mean±SD;non-normal distributed data were described by median and quartiles.Differences in pre/post-intervention scores between the REBT and control groups were subjected to independentsamples t-tests (normal distribution data) or Mann-Whitney U tests (skew distribution data).Moreover, we compared difference scores of the two groups on the data of three time periods using repeated-measures ANOVAs and simple effects to distinguish effects among time, group, and time-by-group interaction.We set α =0.05, and the confidence interval was 95%.
3.Results
A total of 60 patients were enrolled in this study, two from the control group changed their treatments at the 4th week, and two from the intervention group were transferred at the 2nd week.Finally, 56 patients completed the study.
3.1.Sample characteristics
The mean age of the REBT group was 57.25±8.51 years,and that of the control group was 53.57 ± 10.77 years.The majority of the participants were married(98.21%),with middle school educations or lower (66.07%), who accepted XELOX or FOLFOX6 treatments(60.71%).The two groups showed no significant difference in their general characteristics (Table 1).After an analysis of outcome variables, we did not find any significant difference in symptoms,anxiety, depression, or sleep state (P <0.05) between the two groups at pre-intervention (Table 2, Table 3).
3.2.Effectiveness of the intervention
According to Table 2, the MSAS-SF-SC and its specific dimensions between the two groups showed a significant difference at the 4th and 6th weeks of the intervention(P <0.05).The results of repeated measurement variance showed that symptom distress was mainly affected by time (F =4.156, P =0.018) and group(F =11.121, P =0.002).The score of the MSAS-SF-SC (F =8.556,P <0.001) and the score of symptom frequency (F =24.709,P <0.001) had interaction effects of time and group.The simple effect results showed that after controlling for the group for interaction effects, the patients who participated in the REBT program showed no significant difference in scores over time, while patients in the control group showed an increase in scores overtime on the MSAS-SF-SC; the score of the REBT group first increased slightly and then decreased, and the score of the control group continued to increase over time for symptom frequency.
We also identified changes in the HADS scores in Table 2.The anxiety and depression scores in the two groups showed a significant difference in the scores of the anxiety dimension and the HADS at the 4th and 6th weeks of the intervention (P <0.05).However, there was no significant difference in the scores of depression between the two groups at the 4th week of the intervention(t =-1.556,P =0.125),there was a significant difference in the scores at the 6th week of the intervention (t = -4.638,P <0.001).The results of repeated measurement variance showed that the HADS(F =13.757,P <0.001),anxiety(F =8.788,P <0.001),and depression(F =7.173,P =0.002)scores had interaction effects of time and group.The simple effect results showed that after controlling for the group for interaction effects,for HADS,the score of the REBT group decreased significantly over time, and the score of the control group showed no significant difference in scores over time; for anxiety, the score of the REBT group decreased significantly over time,and the score of the control group increased after a decrease over time; for depression, the score of the REBT group decreased significantly,and the score of the control group was flat with no significant difference over time.
Because of PSQI’s interval requirement of measurement time,we only compared the sleep state before and after the intervention.According to Table 3,we found a decrease in PSQI scores in the REBT group between pre/post-intervention, whereas the control group showed an increase (Z =-3.706, P <0.001).In addition, we observed that the REBT group showed significant changes compared with the control group in sleep quality (Z =-2.343,P =0.019), sleep efficiency (Z =-2.888, P =0.004), sleep disturbances (Z = -2.612, P = 0.009), and daytime dysfunction(Z =-5.829, P <0.001) at post-intervention.
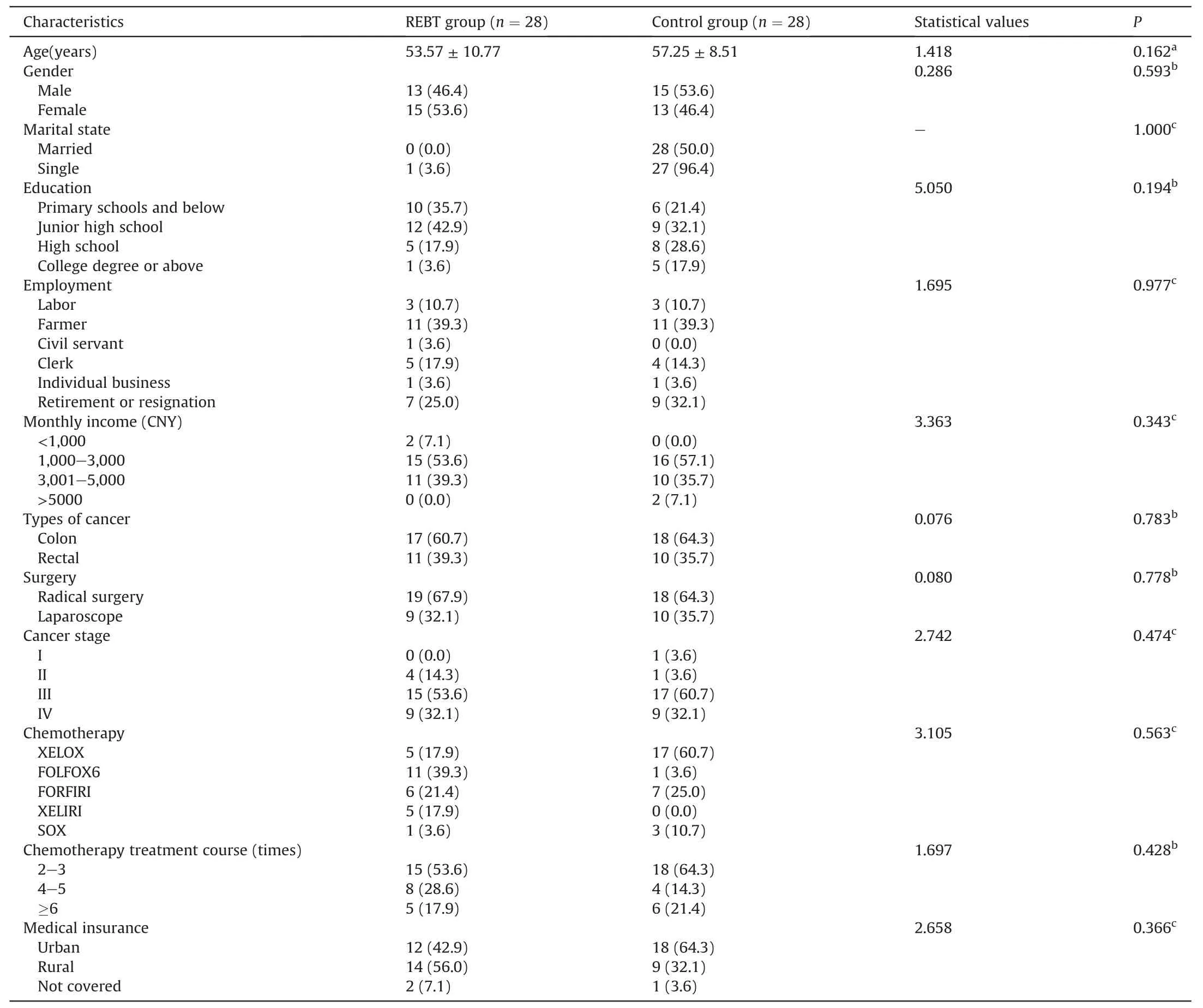
Table 1The homogeneity tests of participants characteristics.
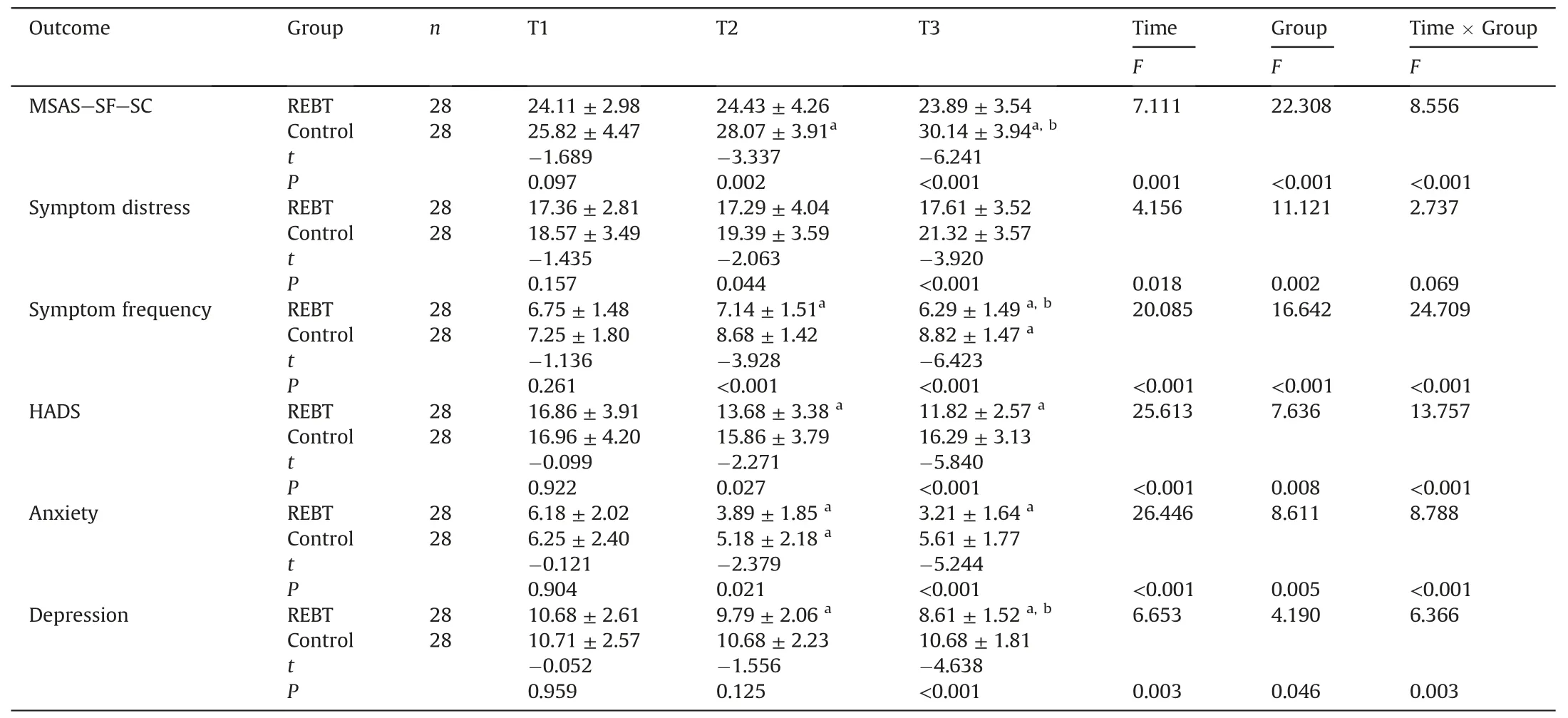
Table 2The effects of REBT on symptoms, anxiety, and depression for patients with CRC.
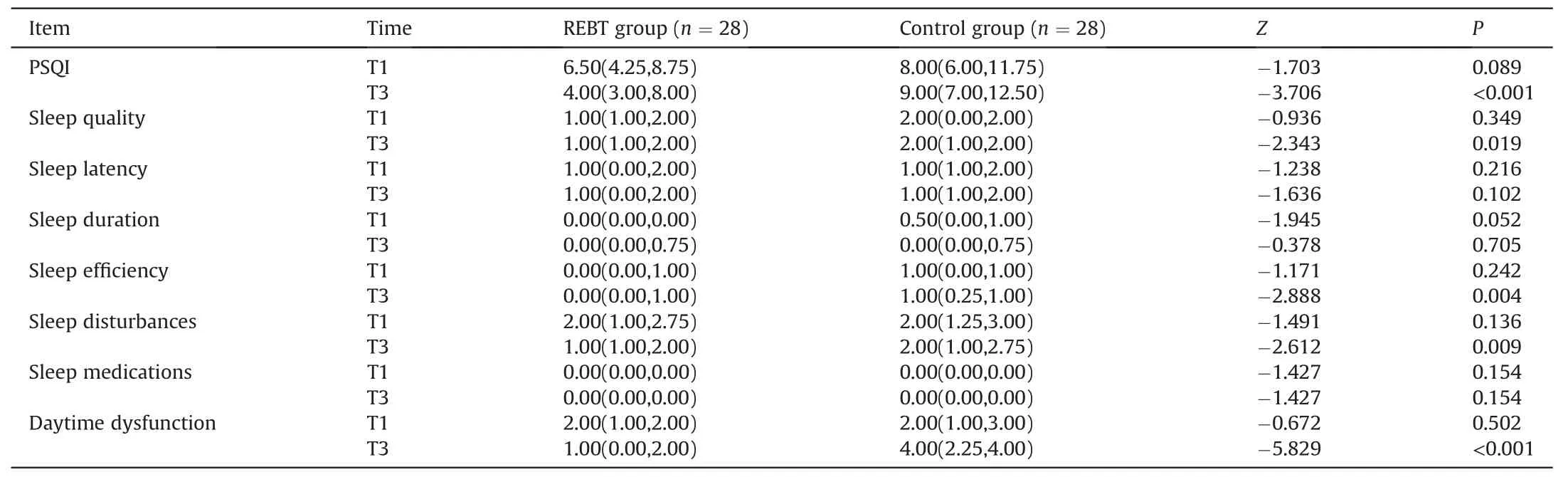
Table 3The effects of REBT on sleep state for patients with CRC.
4.Discussion
In this study, we developed the REBT program according to chemotherapy characteristics in patients with CRC and investigated the effects of REBT in patients with CRC.The results showed that REBT effectively improved symptoms, anxiety, depression, and sleep state in patients with CRC undergoing adjuvant chemotherapy.
Some studies [25,26]discovered that adverse reactions caused by chemotherapy drugs were an important factor affecting thehealth and quality of life of patients with CRC.The results showed that both groups of patients experienced mild symptoms of distress at the time of the first investigation.This finding is consistent with the results of O’Gorman[27],who found that patients experienced at least one symptom (e.g., bowel function, nutrition, pain,dermatological issues, and urinary issues) during chemotherapy.Meanwhile,we found that patients experienced severe anxiety and depression in three investigations.These results are consistent with previously reported research data [27,28], and anxiety and depression were common emotional symptoms of adjuvant chemotherapy patients.If the symptoms, anxiety, and depression are unaffected, they may still deteriorate in a short time.
Moreover, the sleep quality of the two groups was not good in our study.This might be due to the occurrence of symptoms or negative emotions.It has once again been emphasized that patients at different treatment stages have symptom distress and negative emotions.Health care professionals who provide care to cancer patients should focus on symptom relief and sleep quality, thus improving quality of life [28].
REBT is a psychological intervention program that aims to alleviate chemotherapy’s physiological and psychological problems by changing irrational cognition and false beliefs.Our REBT program can better understand the patients’problems and ensure that the patient participates in their care through the establishment of health files at the first interview so that we can judge the patients’cognitive level and eliminate inaccurate health beliefs according to the collected data, by summarizing common problems and recording each problem.After that, a group discussion with professionals could efficiently determine and address the patient’s concerns, which may help to share knowledge and the emotional responses associated with the disease.Meanwhile, we referred to the American Cancer Society Colorectal Cancer Survivorship CareGuideline [29], and our program would continuously provide information about symptom/functioning management and healthy lifestyle recommendations.It was convenient to encourage patients via WeChat to complete weekly relaxation tasks (including listening to music, reading books, walking, and other sports) to continue providing health education content per week to consolidate rational beliefs repeatedly.Although the duration of our intervention was relatively short, the results showed a positive effect.These results were consistent with Ogbuanya’s[25]12-week rational emotive behavior therapy.Both of them could effectively improve poor symptoms by follow-up.It is likely that through group sharing and the continuous dissemination of disease knowledge, the patients’ ability to learn and understand diseaserelated knowledge was increased.
On the one hand, our results showed that symptom distress significantly changed over time with differences in the two groups.The degree of distress in the control group continued to deteriorate,while patients in the REBT group maintained the original state or slightly improved.At the 4th and 6th weeks of the intervention,the symptom frequency in the REBT group showed minimal change,while the control group showed more serious symptoms.This may be because patients had a preliminary understanding of the symptoms that may occur or have occurred so that the degree of distress was alleviated through our intervention.However,patients who have not undergone treatment remain in their original state or even worse.
On the other hand, a study [30]revealed the correlation between rational beliefs and psychological distress that could reduce psychological distress by improving rational belief.To help people overcome their irrational beliefs and the accompanying symptoms,we would conduct Q&A training[12]from text messages and voice chat on WeChat, and face-to-face interviews according to their preferences and cultural background.We improved patients’ anxiety and depression and reduced psychological distress by transforming irrational beliefs into rational beliefs.As time progressed,the patients’ emotions would differ, but after comparing the two groups before and after this study,the REBT group was significantly better than the control group.It was found that the HADS scores of the REBT group decreased significantly.The patients in the control group had no significant change in anxiety and depression over time, while patients’ emotional states in the REBT group were improved considerably.The findings are consistent with the results of Zhang et al.[8]and Dong et al.[9], and a study with a psychoeducational and a support group intervention of Bredal et al.[31]showed the same.This may be because the relationship between patients and medical staff was more intimate through personal interviews disseminating health education materials [30,32],eliminating part of the patients’ fear of disease to embrace life.In addition,Coles et al.[33]mentioned that a quarter of patients likely experienced sleep disturbance after diagnosis.Our study of sleep quality found that the REBT program had no significant advantage in sleep latency and sleep duration, which could effectively improve sleep efficiency and the ability of daytime function and reduce sleep disorders.Even if this result was possibly associated with emotional relief, the relaxation techniques were probably positively affected.Considering that few patients included in the study used hypnotic drugs and the program’s short duration, two measures(sleep latency and sleep duration)did not show statistical significance.The findings are consistent with Fong et al.[34], who showed that mindfulness intervention and REBT could reduce symptoms of distress and improve sleep quality, but the drugrelated indicators were not known.The results show that our REBT program may be an effective intervention that can relieve symptoms of patients with CRC undergoing adjuvant chemotherapy and improve anxiety, depression, and sleep quality.
5.Limitations
Based on our results, this project is valuable for patients with CRC.However,several limitations were inherent in this study.First,we recruited patients from only one hospital in China.The sample size of the participants in this study was small,limiting our results.Second, most of our study participants did not have a high educational background, and most of them were in tumor node metastasis stages III and IV.As such, the efficacy of the intervention cannot be generalized to all patients with CRC.Next, the participants in this study were recruited voluntarily rather than at random.Thus, they cannot represent a general, large population.Therefore, we look forward to developing long-term and effective REBT programs in combination with the internet,community,etc.,platforms in the future.
6.Conclusion
Despite the study’s limitations,the results suggest that a 6-week REBT program can significantly improve patients’ symptoms, anxiety,depression,and sleep state.Over time,both groups’symptoms,negative emotions,and sleep state changed,generally improved in the REBT group compared with the control group, which showed the effectiveness of the REBT program in the project.According to our findings, the REBT with personalized communication and interviews, professional participation in group discussion, continuous dissemination of health education,and relaxation techniques can be included in the nursing care system as a supplementary care plan for patients with CRC who are repeatedly admitted to the hospital for chemotherapy.
CRediT authorship contribution statement
Yuxin Liu:Conceptualization, Methodology, Investigation,Writing-reviewing & editing.Xiaoyan Ni:Data curation, Investigation, and Writing-original draft.Rong Wang:Resources, Investigation, and Supervision.Huini Liu:Writing-original draft,Writing-review & editing.Zifen Guo:Conceptualization, Project administration, and Funding acquisition.
Funding
Guo received partial support from the Education Department of Hunan Province (No.19A419).
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of competing interest
The authors have declared no conflict of interest.
Acknowledgments
We thank the Education Department of Hunan Province and the First Affiliated Hospital of University of South China for their support and the patients and their families who participated in the study.We want to acknowledge the authors of both the Chinese version and the original tool development authors for their contributions.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2022.02.002.
杂志排行

International Journal of Nursing Sciences的其它文章
- Effects of mindfulness meditation on trait mindfulness, perceived stress,emotion regulation,and quality of life in hemodialysis patients:A randomized controlled trial
- The effect of slow deep breathing relaxation exercise on pain levels during and post chest tube removal after coronary artery bypass graft surgery
- The association between frailty of older stroke patients during hospitalization and one-year all-cause mortality:A multicenter survey in China
- Translation and piloting of the Chinese Mandarin version of an intensive care-specific pressure injury risk assessment tool (the COMHON Index)
- Adaptation and validation of pediatric peripheral intravenous catheter insertion and care practices audit tools
- Distress management in cancer patients:Guideline implementation based on CAN-IMPLEMENT