The social determinants of health influencing obesity for the aged in the Pakpoon community context: A qualitative study
2022-05-10PornchanuchChumpunuchUraiJaraeprapal
Pornchanuch Chumpunuch, Urai Jaraeprapal
School of Nursing, Walailak University, Nakhon Si Thammarat, Thailand
Keywords:Aged Community networks Health services Obesity Qualitative research Social behavior
ABSTRACT Objective: This study aimed to describe the social determinants of health influencing obesity for the aged in a community context and based on the perspectives of various stakeholders.Methods: This was qualitative content analysis study using data from the focus group, individual indepth interview, and observation.The study population was domiciled in Pakpoon Village, Mung District, Nakhon Si Thammarat Province, a tight-knit settlement typical of most retirement communities.Data were collected through two focus group discussions, direct observation, and in-depth interviews with 19 participants.Respondents represented key community groups: local nurses and public health officers, elderly residents, family caregivers (family members), and village health volunteers.Results: The participants shared similar perspectives about the social determinants of health influencing obesity in the aged,which spanned three themes.These were:1)neighborhood food environment(easy access to unhealthy food, no choice to recruit healthy food); 2) social networks influencing obesity(family affects food choices and prohibitions on exercise; belief, and socially imposed body image perceptions contributing to obesity in the aged); and 3) knowledge, attitudes, and beliefs behind lifestyle choices that cause obesity in the elderly(lack of awareness,personal attitudes,job and familial duties as barriers to engaging in physical activities; over-consumption behaviors lead to obesity in older people).Conclusion: These three themes were the root causes of obesity in the elderly in Pakpoon’s retirement community.This finding suggests that policymakers and nurses can create healthy environments,both to treat and prevent obesity, by raising awareness in younger generations,providing aging the provision of healthy food choices for older adults, encouraging health care professionals to share knowledge, and by modifying the attitudes and beliefs of both caregivers and older adults.
What is known?
· Obesity in the aged is most often caused by consuming highdensity, fatty foods and lack of exercise.
· The social determinants of health are defined by the WHO as the conditions in which people are born,grow,live,work,and play,which impact health.
· Social determinants of health influence nutritional and physical behaviors in older adults.
· Social determinants of health include socio-environmental and cultural factors that determine population health.
· Socio-cultural factors such as family eating patterns,community food environments, food costs, income, and food preparation skills influence obesity.
What is new?
· Specific neighborhood food environments, social network influences, and specific knowledge, attitudes, and beliefs influencing lifestyle choices are the main factors influencing obesity in the elderly in particular community contexts.
· Social and cultural environments in local communities influence aged population health.
· The social determinants of Thai society shape local food environments,social networks,and personal lifestyle choices,which are environmental obesogenic factors in aged populations because the elderly are reliant on their communities for support.
· Obesity in aging populations is caused by people’s ingrained responses to their obesogenic environments and willpower,which are impacted by socio-cultural and environmental factors exerting powerful influences on community food environments,eating habits, and physical activity.
1.Introduction
Obesity is a critical public health issue in many countries.According to the WHO, obesity is an abnormal or excessive fat accumulation that may affect health [1].Obese individuals have a BMI greater than or equal to 30 kg/m2[1].The majority of the world population lives in countries where people die more from complications related to obesity than from being underweight [1].Global obesity is expected to increase significantly by 2025[2],with approximately 13% of adults worldwide in the obese category [1].This means more than half a billion people worldwide are clinically obese [3].According to a world survey of geriatric populations,around 37.1% of men and 36% of women aged 60 years old and above are obese.Moreover, around 68.6% of aging women are obese,and consequently,the global burden of disease is increasing because the population of obese, aging people worldwide has increased significantly [4].
In Thailand, obesity in male and female adults has increased significantly from 2000 to 2025 [2].Thailand’s population is also aging longer as health care improves, and consequently, the proportion of older adults is rising sharply [5].In Thailand, the proportion of aging people is predicted to be an astounding 30.2% by 2035 [5].According to a Thai national health survey conducted in 2014,one in three adults in the domestic aging population is obese,equating to 27% of aged males and 43% of aged females [6].
Obesity causes many diseases and negative health outcomes.For instance,four million people die globally because of high BMIs,and two-thirds of people with high BMIs often die due to cardiovascular diseases [7].Furthermore, the obese in the world’s aged populations have a much higher risk of developing hypertension and arthritis [8].Sadly, obesity is also one of the most accurate predictors of type 2 diabetes [9], and obesity is also a well-known clinical risk factor for many non-communicable diseases such as hypertension, stroke, cardiovascular disease, osteoarthritis, and cognitive decline [10].
Obesity in the aged is generally caused by two main factors:consuming high-density,fatty foods,and lack of exercise[1].Social determinants of health shape these nutritional and physical behaviors in older adults.According to the WHO,“social determinants of health are the conditions in which people are born, grow, live,work and play, which impact on health” [11,p361], meaning that social, environmental factors determine population health.Scholars generally agree that a family’s eating patterns, the community food environment, and the wider socio-cultural environment influence obesity [7,12].
The immediate neighborhood food environment can increase a local population’s collective BMIs.Living in a neighborhood with a high density of fast-food restaurants is significantly associated with obesity [8,13].In contrast, the better the access to healthy food is,the healthier local aging populations are[14].A compounding issue is that people who have fewer healthy food choices locally are more likely to be obese than many healthy food choices [15].
Many factors influence the food choices of aging people, in particular.For example, older adults’ eating behaviors are influenced by income,food cost,food preparation skills,and local access to healthy foods [16].Healthiness, taste, price, and travel time to grocery stores impact older adults’meal decisions because they are generally less mobile, with a fixed income [17].
Currently, most studies use quantitative research methods to identify social determinants of obesity in aging populations.Numerical findings are used for generalization, e.g., the correlation between social factors affecting the health of older adults with obesity [18,19].However, quantitative results fail to narrate perceptions of and personal experiences with obesity and obesity determinants in the aged,which are integral to treating the obesity epidemic worldwide, especially in vulnerable populations, i.e., the elderly.Despite these shortcomings, very few studies have attempted to use qualitative methods to elicit community perceptions and explain community experiences of what social determinants of health influence obesity, which could be considered the missing link needed to prevent and reverse obesity in older adults.According to their beliefs, each community is different in context.Therefore, social determinants in the aged population depend on their community’s perspective, view, and experience.
Pakpoon is predominantly a retirement community, with an aged population of around 5,785 people.Approximately 38.3% of the elderly in this community are obese [20].The Pakpoon community has created many aged care services to support its elderly population; for instance, health care professionals have developed a database for collating personal health history medical records and reporting on health assessments [21].In Pakpoon, most elderly residents have access to health care services at the community hospital.This hospital provides primary health care services in dealing with obesity in Pakpoon’s aging community,such as home visits, education about nutrition, exercise programs, and public spaces for exercise[22].Despite these services,many elderly people remain obese.Therefore,this research was commissioned as part of a larger study aimed at developing innovative methods for achieving weight loss in the elderly in 20 sub-districts of the Upper Southern Region of Thailand.Study cofounders believed it was necessary to understand the local social determinants of obesity,which they felt were profound causes of obesity in the elderly.Study cofounders wished to design effective innovations to reduce weight in their charges, the elderly.
The current research aimed to obtain a deep understanding of how social determinants influence obesity in the aging population residing in Thailand’s Pakpoon quarter, a semi-urban area in the Mung District, Nakhon Si Thammarat Province.This research was designed to be a first step in developing a clinically effective obesity intervention for aging populations, with Pakpoon as a pilot.It was envisaged that the pilot could then be applied as a model for providing obesity interventions in similar demographic,social and cultural contexts.Because local voices are important in the obesity discourse,the research team utilized the focus group,and in-depth interview approaches to community assessment to allow people in the Pakpoon community to add their very important views to the discussion.
Study founders believe this work is important for community nurses in Thailand.In other countries where a similar demographic context might exist,the social determinants of obesity are likely to include local elements such as community views in many societies.Thus, this work is seen as a beginning step in creating effective nursing care programs and interventions that can solve the obesity problem from the ground up.Study founders believe that responding to the needs of an aging population requires their voices to be heard if interventions are to be effective.
2.Methods
2.1.Research design
A qualitative descriptive research study design was used.The research team used the focus group,individual in-depth interview,and observation methods as “total package” community assessment tools to understand the social factors associated with obesity in Pakpoon’s elderly.The focus group effectively collected a wider range of views,beliefs,and experiences.In contrast,individual,indepth interviews allowed deeper, narrower investigations of experience,views,beliefs,and personal matters a participant might not be comfortable expressing in a group situation[23].In in-depth interviews and focus group discussions,direct observation of facial expression and body language was also used to gain insights into reactions to others’statements,personal behaviors,and consent or dissent [24].
2.2.Participants and sampling procedure
A purposive sampling strategy was used to select the key informants according to well-established protocols [25,26].The participants were Pakpoon’s obese elderly and those involved in their care who resided in Pakpoon when this study was conducted.“Elderly”and“aged”were defined as adults aged 60 years or above.
To achieve buy-in from participants,community leaders known to the participants were employed as “gatekeepers” to recruit participants by approaching them face-to-face, according to three strict inclusion criteria: 1) participants had to be verbally competent to explain in detail their perceptions of social determinants of health and obesity;2)participants had to display cognitive function sufficient to understand researchers’ instructions and respond clearly to questions about the social determinants of obesity; 3)carers of the elderly were required to have had more than one year or more of experience as caregivers(caregivers could include family members, formally trained health care professionals, community health volunteers, and local leaders); and 4) aged residents were required to be obese,with a BMI greater than or equal to 30 kg/m2as per the WHO definition[1].The“gatekeepers”administered the selection process.
In addition, residents who had lived their whole lives in Pakpoon were preferentially selected.Still, family caregivers were not excluded if they had recently moved into the district to care for family members.However, to ensure enough familiarity with the Pakpoon community to answer questions accurately, all participants were required to have had at least one year of continuous regular association with the community before the study commenced.Commuting health care professionals and caregivers were included.The non-obese(normal weight range)elderly were excluded.Caregivers were not screened according to BMI.
2.3.Data collection: interviews and focus groups
2.3.1.Focus groups
Focus groups were considered a more efficient way of gathering participants’ multiple opinions, views, and experiences.Scholars agree that gathering information from a group where participants are comfortable talking in front of others,yields better results than individual interviews [27].Participants were divided into two smaller,manageable focus groups to allow everyone to have a say.This allowed the moderator to efficiently manage interjections,overtalking, and other interruptions.Smaller groups provided participants with a non-stressful environment where they had plenty of opportunities to contribute their views and experiences[27].
2.3.2.In-depth interviews
In-depth interviews allowed the researcher to explore specific personal perspectives and behaviors; one-on-one, private interview sessions were useful for eliciting more honest responses where individuals were hesitant in front of a group,and gathering new material about the determinants of obesity was our focus[28].In-depth interviews were also used to ensure data reached saturation [29].
2.3.3.Observational methods
The observation method is often used in social sciences research[30].During focus group discussions and in-depth interviews,research participants were observed for non-verbal behaviors while sharing their experiences and perceptions about the social determinants of obesity.The observer was one of the two authors designated to watch proceedings.Body language incongruent with verbal expression was of particular note;the observer took notes on small but important details such as facial expressions, arm and hand movements,posture,foot movements,and muscle clenching,all expressions of feelings about a subject [24].
Two focus groups and individual in-depth interviews were conducted.Each focus group had a subsample of eight (n =8)participants.Participants represented a comprehensive crosssection of the community: community nurses, public health officers, caregivers, aged residents, and village health volunteers.Individual, in-depth interviews were conducted with three research participants (n =3) who did not attend the focus groups due to conflicting schedules and wished for a private hearing.Nine participants(n =9)randomly sampled from the two focus groups were interviewed one-on-one.Some participants in the focus groups were unable to do in-depth interviews because of busy schedules.Consequently, the private interviews included twelve (n =12)research participants, out of a total of 19 (n =19) participants.
The researcher informed respondents about the study and required agreement to participate.Respondents were also consulted about a venue, date, and time convenient to participate in focus groups and in-depth interviews.
The semi-structured interview questions were used for focus groups and one-on-one interviews(Tables 1 and 2).Questions were arranged in a deliberate way to elicit the free expression of participants’ opinions and experiences; for example, the interview schedule contained open-ended questions as per qualitative research protocols[31].In addition,the interview and focus groups questions were constructed as guides, not a rigid schedule, which allowed the facilitators to adapt questioning according to participants’varied responses[31].The two focus group sessions and indepth interviews lasted about 1 h (60 min) each.No participant refused to speak or withdrew at any time.No repeat interviews or focus group discussions were conducted.
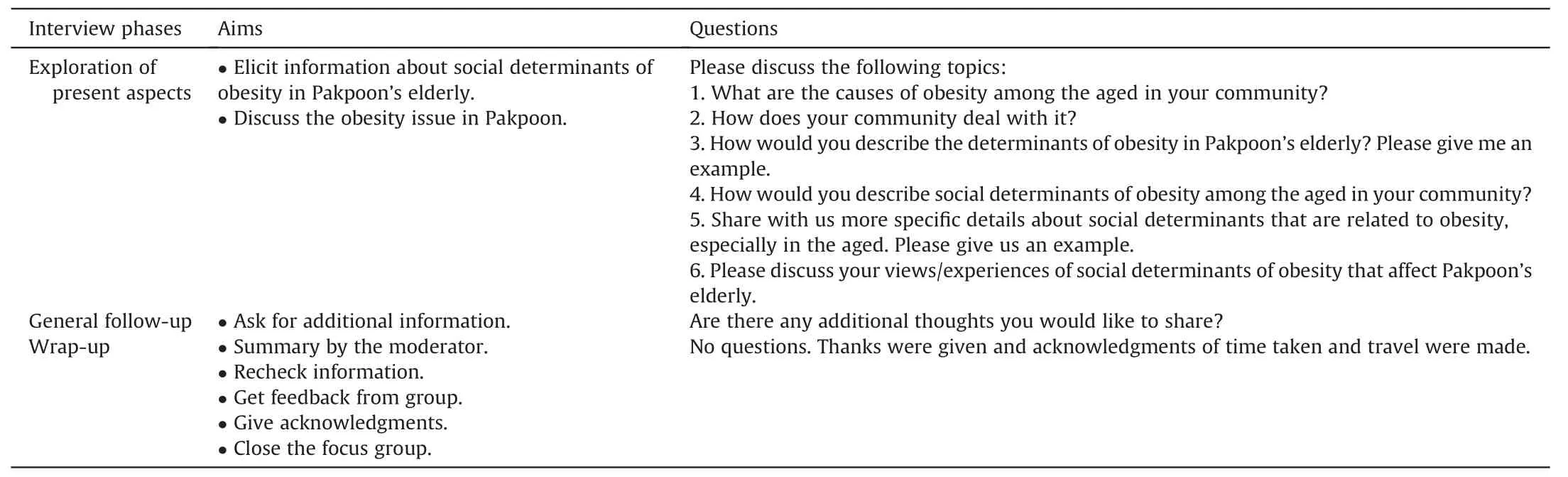
Table 1Semi-structured interview questions for focus group discussions.
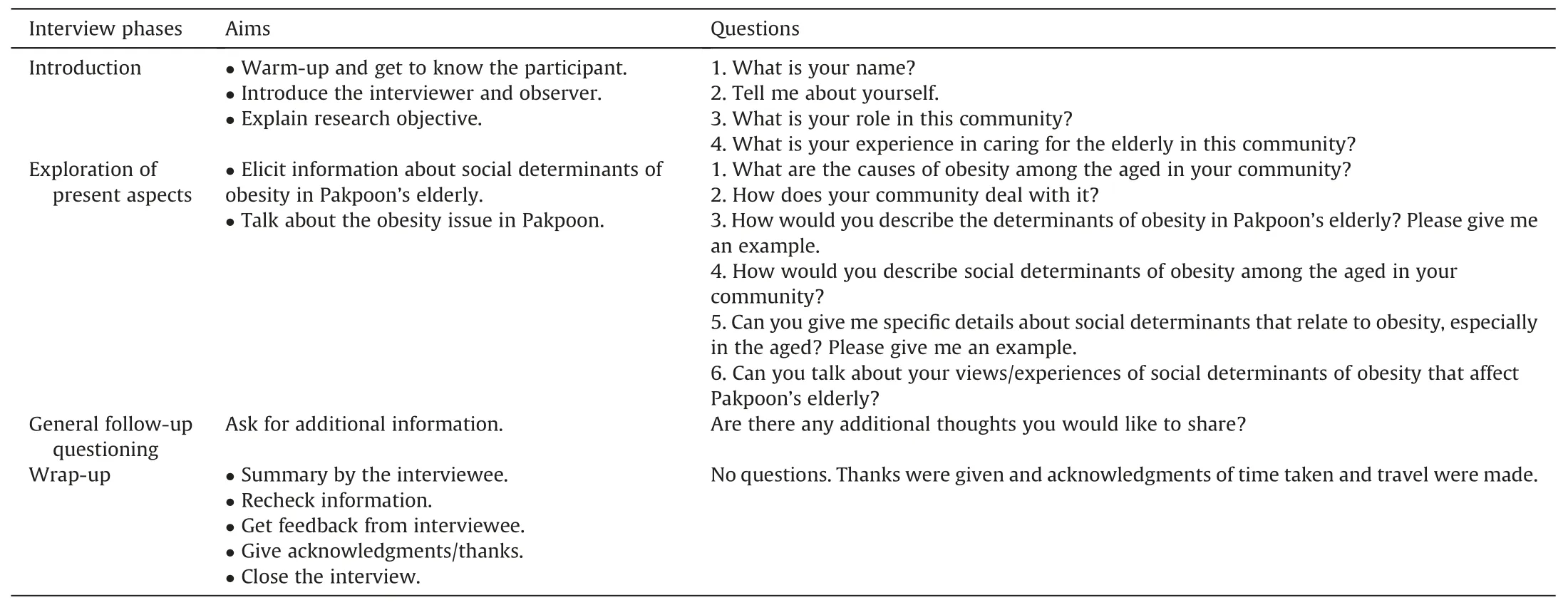
Table 2Semi-structured interview questions for individual in-depth interviews.
Interview questions were not sourced from instruments created by other people; therefore, no permissions to use research instruments were required for the current research.No copyright or licensing restrictions apply to the interview questions.
The authors were the focus group facilitators and interviewers,both female nurses trained in qualitative research data collection from human subjects.Field notes and audio recordings were taken during the interviews and focus group discussions.The transcripts were sent to the participants for comment and correction.Data were collected until there were no new emerging themes, and repetition of categories was observed[32].The independent coders reviewed the data independently and agreed that data saturation had been reached.
2.4.Data analysis
First, content analysis was performed; the interview transcript text was read several times until the authors were familiar with the scripts.The whole text was subsequently parsed into small parts.These parts reflected the entire text and contained their condensed meaning, just as they reflected each portion [33].Thus, eachportion of the text acted as the condensed unit of meaning that could be used to answer the research question.These “units of meaning” were labeled to form several codes.The codes reflected the raw data and indicated the relationships within the units of meaning.
The authors repeated the coding process a second time to ensure that all codes were directly related to the research objective.Codes were then compared to determine broader categories that contained related codes.Themes were subsequently derived from categories so that they shared the same perspective and dimension.This formal organization of the data followed commonly accepted procedures,which allowed the authors to reach conclusions about how social determinants influence obesity in the elderly [33].A flowchart showing the steps used to analyze the data is presented in Fig.1.
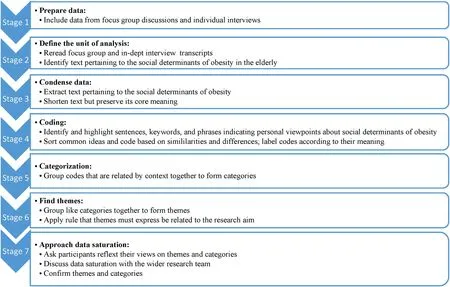
Fig.1. Flowchart showing the seven steps of data analysis.
2.5.Trustworthiness
The trustworthiness of this research can be derived from clearly identifiable aspects of credibility,transferability,and dependability inherent in its methodology [34].
2.5.1.Credibility
Credibility can be derived from the fact that the authors had previous knowledge about obesity in aged populations; when the research was conducted, both authors were trained nurses (with the Registered Nurse[RN]qualification)and lecturers at the School of Nursing, Walailak University.The first author held a Bachelor’s degree in nursing and a Master’s degree in public health,while the co-author held a Ph.D.in Nursing Science.Furthermore,most of the co-author’s previously published research was qualitative.
The research was conducted based on a robust planning process in which the authors carefully mapped procedural details for data collection and analysis processes to ensure a valid result.Alignment with commonly accepted qualitative methods [31]was also checked before the results were reviewed independently by research participants to verify the accuracy of local details.
The author and co-author worked as a unit to ensure credibility to transcribe interview responses.A group of contributing researchers initiated a peer debriefing process to ensure adherence to qualitative protocols.The authors met regularly (three times a week for four weeks) to create the coding scheme and refine criteria for defining categories.The transcribed text was re-read six times by the author, co-author, and the contributing researchers until all parties were familiar enough with the content to identify codes and categories as a group.Experienced coders further validated the groups’ work, and results were challenged until all contributing researchers reached an agreement.
2.5.2.Transferability
Addressed the transferability of this research study by providing a rich,detailed description of the data analysis process and research participants.In addition, this study also explains how all data is handled, including detailed documentation about identification numbers,category names,theme names,and theme definitions,as per commonly accepted guidelines [35].As a result, other researchers could transfer and use this finding to adjust and apply it in different contexts.
2.5.3.Dependability
Dependability was derived from consistency.The codebook ensured that the coders used the same, clearly defined process to analyze all the data.To ensure coding consistency, reliable coding,and dependable research results, the two coders were required to have at least ten years of qualitative research experience.The coders were, in fact, the author and co-author, who were formally trained in qualitative research techniques, particularly the coding process as it applied to the current research.
2.6.Ethical considerations
The work described in this article was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki).The Office approved the study of the Human Research Ethics Committee of Walailak University.The reference number for the approval is WUEC-19-142-0.The approval was issued on September 9th, 2019.
Study participants were informed that their details would remain confidential to the authors and the participants themselves.All references to participants contained herein are anonymized.All respondents provided informed consent before focus group sessions were launched.Before each focus group session,participants were given a brief verbal description of the research,followed by a more detailed written description explaining research objectives and study processes.Participants were also informed of their right to withdraw from the research at any time.They were reassured that identifying details would be removed from recorded audio transcripts.Study participants’ personal information, including their contact details, is securely stored to avoid accidental release.
3.Results
3.1.Demographic information
The participants’demographic information is shown in Table 3,including anonymized ID,age(years),gender,social role,and years spent living or working in Pakpoon.Social positions were representative of community composition: aged resident, village health volunteer,public health officer,community nurse,family caregiver(family members), and a practitioner of traditional Chinese medicine.All participants lived or worked in Pakpoon at the time and had done so continuously for at least one year.Family caregivers were family members of aged residents.All village health volunteers were caring for aged residents with the chronic disease when the study was conducted (some of them also cared for other aged family members).All aged residents who participated lived in Pakpoon and were classified as obese,with a BMI >30 kg/m2.At the time of the interviews, the community nurse and public health officer were working in Ban Pakpoon Tambon Health Promotion Hospital as was the practitioner of traditional Chinese medicine.
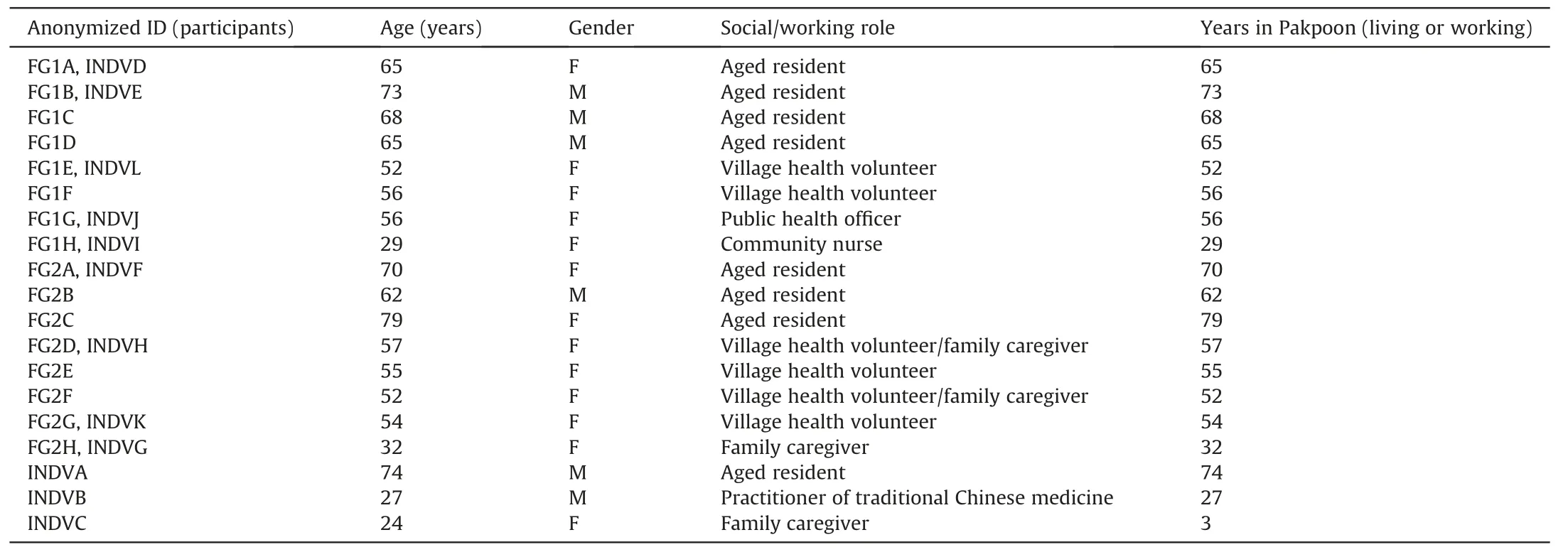
Table 3Participants’ demographic data (n =19).
Village health volunteers are defined as persons willing to help older adults in need.These volunteers perform comparatively well on short-term tasks such as taking health surveys, collecting periodic data,conducting disease prevention campaigns,and caring for aged people who have a chronic disease.
The ages of older adults ranging from 60 to 79 years and aged particpants were classified as obese.Village health volunteers were aged from 35 to 37 years.Health care providers were between 27 and 38 years old, and family caregivers were between 24 and 32 years of age.Table 3 shows participants’ demographic data.Participants are differentiated by an anonymized coding system,whereby FG1 refers to focus group 1, FG2 refers to focus group 2,and the following letter (A-H for eight participants per group)refers to the individual, whereas INDV refers to individuals participating in in-depth,one-on-one interviews,and the following letter (A-L for twelve interview participants) refers to the individual.Some participants were involved in both focus group discussions and private interviews; therefore, they are identified by both an FG and an INDV code.Where identification of participants in one-on-one interviews does not contain focus group information,that individual did not participate in focus group discussions,and vice versa (Table 3).Eight respondents participated in one of two focus groups(n =16),and only seven of these did not wish to be interviewed separately.Twelve respondents consented to individual interviews,and only three of these did not join a focus group.
3.2.Themes and categories
The findings indicated that neighborhood food environment,social networks, and lifestyle framed obesity issues for the elderly in Pakpoon.Table 4 shows the interrelated themes and categories,which are illustrated by verbatim responses discussed in this section.
3.2.1.Neighborhood food environment influences obesity
The participants stated that their local food environment induced obesity in the aged because of Pakpoon’s easy access to unhealthy food, with no healthy food choices available (Table 4).Their comments on the two categories(an abundance of unhealthy choices vs.no healthy choices) provided a clear picture of the neighborhood food environment.

Table 4Themes and categories that emerged from focus groups and in-depth interview transcripts.
3.2.1.1.Easy access to unhealthy food causes obesity.A high number of local restaurants sold unhealthy foods, especially Thai-Islamic fusion restaurants, which offer high-fat, fried dishes.Many teahouses and coffee shops, which sell deliciously sweet and fatty confectionary, were also reported as present in Pakpoon.These outlets were reported as being open at all hours and were conveniently spread across the Pakpoon area.One participant mentioned just how convenient access to the many unhealthy retail food outlets was:
“Due to food prosperity and convenient access, the Pakpoon …people’s eating habits are easy,simple and conveniently accessible.Moreover, Pakpoon has additional factors as teahouses and coffee shops [that]stay open almost 24 hours.” (FG1H)
Another two participants concurred:
“There are a lot of Muslims here,[and]Islamic food,which focuses on fat and deep-fried dishes.You can find them anywhere, likewhen you walk from here for about 100 m, you will find one.Roti shops…[there]are several here,and open from morning until late[at]night.There are a lot of teahouses, which focus on mostly desserts with coconut milk.” (FG1G)
“For Pakpoon people, [junk food]is easily accessible.We drive for less than 1 km, we will see [a]teahouse, convenience store, food store.” (FG1F)
3.2.1.2.No choice to recruit healthy food induce of obesity in the elders.In Pakpoon,most people spent most of their time working to earn money.Therefore,they bought junk food close to home for the aged, even though they knew it was unhealthy.Lack of time,combined with the proximity of fatty foods, was cited.
“They spend all their time working to earn money.Therefore, it is necessary to buy food that is sold near the house.Even knowing that it is unhealthy food.” (FG1H)
One caregiver felt that if the community had as many fruit shops, people would buy fruit.But the plethora of tea houses provided only opportunities to purchase “junk” food.
“Many tea shops in this community lead to obesity.Some people can’t go anywhere, they can’t buy anything.They need something to eat nearby.If there are many fruit shops, people will be interested in buying fruit,but there is no fruit to choose from.There are only tea shops,so [older people are restricted].” (INDVC)
It was stated that most local parties offered fatty foods,such as pork soup or mild coconut soup.
“Moreover, there are several parties in the village; we can’t[make healthy]food choices, what we want to eat in the party.” (FG1G)
“That fat-filled pork soup, coconut milk soup! They’re party staples.” (FG2A)
3.2.2.Social networks influence obesity
“Social network”describes close social contacts,such as families and close friends, who exert influence on older people's health behaviors, which in turn affects tendencies to obesity.
3.2.2.1.Family affects food choices and prohibitions on exercise.
In Pakpoon, age-related deterioration was the leading cause of an inability to move long distances.Due to lack of mobility, such as being unable to walk because of a knee problem, family members brought meals to the elderly.Therefore, they ate whatever their families provided.Because Pakpoon’s elderly did not have a chance to choose healthy foods,they had to eat foods that induced obesity,such as sweet and fatty foods.In addition, families did not allow their elders to exercise because they believed it was inappropriate.
“The problem [is]knee ache, [being]unable to conveniently walk.And in the working age[group],they go out and work,so they find food and leave it for the aged.They buy whatever they want without asking if the food is right for the aged.” (FG1F)
A caregiver concurred.
“The elderly’s diet depends on the person who buys the food for them because the elderly always stay at home and do not go out.The choice of food depends on what the family member brings.For example,the grandchildren buy sweets or coconut curry.In the end,the elderly have to eat the sweets or coconut curry.” (INDVC)
One aged participant indicated that their children bought all the food because they worked nearby to food outlets, whereas the participant worked at home, further away from food shopping.
“We stay in the same house but work in different places.When we come back,they buy a lot of things,and we eat[what we get]from them.” (FG1A)
Another participant added that the inability to choose one’s own food impacted on consumption patterns,such as eating schedules.
“The eating habits [of the aged are]from the inability to choose.” (FG2E)
“The kids will buy food and leave it for their parents.They eat when they’re hungry,so there’s no schedule.Can’t choose the food.Eighty percent is from what the kids buy.” (FG2F)
One participant mentioned that the aged could not dance because their children did not want them to do it.
“The kids don’t want [the aged]to [exercise]because they are already old.When they want to dance, the kids also don’t want them to.This is the problem in the family.” (FG1F)
3.2.2.2.Beliefs and socially imposed body image perceptions contributing to obesity.The elderly in Pakpoon made other lifestyle choices based on their own attitudes, beliefs and knowledge as well.Being overweight was associated with wealth, financial stability,and dignity.In contrast,thin body shapes indicated financial instability.This belief influenced dietary behaviors such as the tendency to consume large amounts of food.
“I strongly believe that the elderly must have a body shape that looks fat but not obese.They should gain weight a little bit.Older people do not look good if they are too thin.If they are too thin,really thin,they look like they lack power and[that is]undignified.”(INDVA)
3.3.3.Knowledge,attitudes,and beliefs behind lifestyle choices that cause obesity
The elderly’s lifestyle choices regarding physical activities and dietary behaviors that induce obesity is related to the knowledge,attitudes, and beliefs of themselves, their family, health care professionals, volunteers,and community leaders as follows.
3.3.3.1.Lack of awareness, personal attitudes, job and familial duties as barriers to engaging in physical activities.Many factors associated with inappropriate physical activity in the elderly may induce obesity due to lack of awareness, attitudes, job and family duties.The elderly must take care of their grandchildren until they do not have time to do suitable exercises.Meanwhile, professional caregivers and elderly care volunteers think the elderly lack awareness of exercise, despite having support from a group and a place for practice.Lack of physical activity was an age-related attitude as well.
Elderly participants believed that swinging their arms around or other gently exercise every day was enough.“Part of it is that [we]aren’t interested in outdoor workouts, [we]just do some light indoor workout,such as[arm exercises].”(FG1D)
Related to lack of exercise, participants indicated that jobs and familial duties,such as looking after grandchildren every day,were reasons for a lack of exercise and obesity.Work and child minding gave Pakpoon's older adults excuses to avoid exercise.
“One of the reasons for lack of exercise is that[we]have no time as[we]have to take care of the grandchildren.” (FG2C)
“The aged need to take care of their grandchildren because the parents have to go to work.” (FG2B)
Busyness at work (paid employment) was also cited as an impediment to exercise.
“Lack of exercise.Even though the exercise places are not enough for all Pakpoon people,it is not an overall factor.The main factor is the importance people put on exercise when job duties give them excuses, more than not having time.” (FG1H)
This community had many places for exercising,but participants said that older people still chose not to exercise.
“Obesity in [the]aged might be from less exercise.” (FG2H)
“There [are]places to work out.If the aged [have]some time, they can come.But most of them just aren’t interested.” (FG2B)
One health practitioner mentioned that the aged did not pay attention to exercise although Pakpoon had many exercise groups where they could exercise with their friends.
“Our community has many places for the elderly to gather and work out together.Our community also has many exercise groups,such as aerobics and Thai traditional dance,where older people can exercise and spend their time with their friends.But most of them are not interested in physical exercise.” (INDVB)
3.3.3.2.Over-consumption behavior leads to obesity in older people.
Participants recognized that most aged residents were educated about healthy food choices,but they still over-consumed food and were not concerned about a balanced diet.They ate large amounts just before bedtime.Although tied to other influences,the volume of food consumed appeared to be mainly a personal lifestyle choice.The relationship between overeating in general and binging on sweets,in particular, was a hot topic.
“The favorite focus[is]on sweets.Some of them[the elderly]focus on carbs, mainly rice.Sticky rice for the morning, fried chicken,greasy rice.They have knowledge but lack awareness.See, that’s general people, even us.We know everything, but do we put[emphasis]on breakfast?No.Instead,it’s on lunch and dinner.A lot of people are like this.Actually, we should focus on breakfast as it gives all-day energy.We focus on dinner because we want to enjoy it.There’s a lot[to eat],but less[energy is]used.We eat and then go to bed.So, this is another factor of obesity.” (FG1G)
“Normally we have three meals a day, but here there are five of them.Coffee and snacks for breakfast,snacks for late morning;late afternoon,almost dinnertime,we go out and buy something to eat.Don’t refuse.Don’t want to waste money.” (FG2A)
Inability to stop eating was related by participants to individual choice.
“Because they don’t limit the diet.They eat a lot,some of them eat 2-3 plates of rice with too much coconut or coconut milk soup.People with obesity is from eating too much,and they don’t know how to stop.It doesn’t matter if you are in a coconut orchard and get fat.The surrounding doesn’t affect this.They have to control themselves.How can you not get fat when you eat,then go to bed?”(FG2C)
“Obesity in [the]aged might be from eating before going to bed.”(FG2H)
“Most of the age will eat then go to bed, so they have obesity and some of them also have diabetes.Food is the important factor,and doing [this]will make them gain weight.” (FG1H)
“We have coconuts,so we make dessert every day,not[all the time]but after the meal, it is good to have dessert.” (FG1A)
4.Discussion
This study found three leading solutions for dealing with the neighborhood food environment, mitigating the power of social networks, and overcoming lifestyle choices.We have presented these findings to the community members and other stakeholders in the Pakpoon community.We created an innovative weight loss program tailored to individual circumstances as future mitigation.
4.1.Dealing with the neighborhood food environment
The neighborhood food environment, especially easy access to unhealthy food and no age-appropriate dietary choices, heavily impacted obesity in Pakpoon’s aged population.An unhealthy food environment is statistically significant in its association with obesity in the elderly[13,36].Worldwide,less mobile,older people like the elderly research participants in Pakpoon, who all had comorbidities,are more likely to buy unhealthy food from a cheap and close to home [37-40].Even in China, where meat is not an everyday staple, higher daily calorie intakes are positively correlated with a better selection of fast foods handy to residential areas[41].
The staple crop in Pakpoon is the coconut,also a staple in other countries [42].Most party dishes cooked for celebrations in Pakpoon use high-kilojoule coconut milk, which is grown locally,similar to different places around the world where staple crops contribute to obesogenic environments [43].This finding suggests that health care teams must manage the neighborhood food environment by helping residents create easier access to healthy foods.Our future interventions will:
· Manage the neighborhood food environment to provide access to healthy food by working with grocery stores, fast-food outlets, and restaurant owners in the community to source healthier food choices by comparing prices,suppliers’terms and conditions, and by utilizing local crops other than coconut, of which there are many,including green vegetables,low-kilojoule fresh fruits, and root vegetables.
· Teach residents and caregivers to prepare healthy and deliciously easy dishes that do not require a lot of time to prepare,construct easy weekly menus that are healthy, and how bad food choices can cause obesity in the aged.
· Encourage existing fast-food outlets and restaurants to adjust their service menus to provide at least a small sample of healthier dishes and products that may rotate based on when local crops are in season.
4.2.Mitigating the power of social networks
The power of social networks influences population health globally[11],especially the elderly,who cannot choose their foods;older people sometimes even prefer to eat alone so that family members cannot supply them with unhealthy food choices, even when the entire family lives together in the same house [44,45].Most older people in Pakpoon took care of their grandchildren because the parents could not afford a nanny and had to work for a living,a common situation worldwide that is also growing in more affluent Western societies [46,47].This suggests that our preliminary findings of social influences on obesity in the elderly may be applicable in many other societies.
In contrast,in Pakpoon,family influences had a negative impact on older people’s exercise behaviors.Still, in other places around the world, family members support physical activity, and younger people often transport seniors to exercise classes or buy home exercise equipment [48].In the Pakpoon context, it was clear that family members’lack of support and negativity was a huge barrier to exercise because the prohibition was felt more strongly by the homebound and less mobile elderly [49], thus making family prohibitions particularly powerful.Our future interventions will:
· We plan to work as a community partnership with families,caregivers, local health professionals, and food store owners under the auspices of an existing Healthy Food for the Elderly program by providing regular, interactive educational and practice-based seminars in Pakpoon, which will involve the preparation of food by participants.The aim is to deepen the relationship with the community and gradually influence local society to accept changes in eating habits.
· Exercise will also be a topic, with short exercise classes offered and education on how to exercise correctly without causing injuries.Recordings of Thai seniors in other locations doing these exercises and giving instructions to their peers will be presented to encourage exercise classes in Pakpoon.A leader in organizing these classes will be recruited with the help of community elders.
4.3.Overcoming lifestyle choices embedded in the culture
In Pakpoon, body image was culturally embedded.People believed that the elderly should be overweight to show their wealth,similar to many other cultures’preferences for curvy body shapes and large body sizes [50-54].In contrast, other people of Asian descent with normal weights prefer thin body shapes in line with their cultural expectations [55,56].These contrasts suggest just how powerful culture is in regulating body weight.
In Pakpoon, elderly residents had, at best, an incomplete awareness about the causes of obesity-especially overeating.This result was consistent with a generally agreed finding that aged people with high BMIs (>25 kg/m2) [1]lack awareness about food quantities that are appropriate to their level of activity, and consequently,they make poor lifestyle choices[57,58].By Pender’s health promotion model,family and peers have the most influence on their elders’ engagement, alongside caregivers and health workers[59].Unfortunately,engaging families in examining deeply embedded cultural constructs is no easy task.
The traditional Thai belief that older adults should limit their activities to taking care of the grandchildren,rather than spending time on themselves,is also an attitude in other cultures,where selfindulgences such as exercise can be seen as selfish [60].Yet, in Pakpoon,paid employment also heavily impacted leisure time,and consequently,the eating habits and health of some elderly research participants [61,62].The full schedules of the elderly, both in Pakpoon and in other communities domestically and worldwide[46,47],mean that interventions must be tailored to meet the needs of busy older people.Our future interventions will:
· We will tailor programs to individuals’ needs to help aged people take time for themselves, lose weight, and learn to appreciate a thinner body image.Eating smaller portions of higher-fiber foods will be a focus.Encouraging the elderly to involve their grandchildren in exercise will also be explored as an option to integrate child-minding duties with healthier lifestyles.
· Older people from nearby districts who have embraced weight loss and exercise, and are happy with the result, may be recruited to visit Pakpoon and deliver their message in a fun,social setting where healthy snacks are served.
· Working as a partnership with the elderly, their families, caregivers, and local health care professionals, we also hope to design weight-loss tutorials covering the topics of healthy food classes and the benefits of involving children in exercise.These tutorials will be designed so that caregivers can use them at home and access them online via desktop or by phone application (app).
5.Discussion
Unhealthy behaviors are strongly correlated to a worldwide epidemic of overweight and obese people affected by similar social determinants of health [63,64].Community health care professionals must transform higher BMIs, associated with increased risk of cardiovascular disease [65], into lower BMIs by promoting moderate food consumption,physical activity,and healthy foods to support quality of life in our elderly[66].The better understanding nurses have of the social determinants framing obesity, the better the chances of the elderly will be in controlling their weight and living longer, healthier lives [11,67].
Although this study probably cannot be generalized to other social settings operating in different contexts, it does provide information about determinants of obesity.It is an example of how powerful social determinants are.Because the obesity epidemic in Pakpoon’s aged population is framed by powerful social determinants of health, which are influences similar to those experienced in many other parts of the world, we believe our findings can be adapted and applied to community nursing interventions in which nurses work with the elderly in similar settings and community contexts.We believe that nurses can deliver betterdesigned health care services tailored to suit the needs of busy but less mobile elderly patients throughout Thailand and in similar social contexts by using our preliminary findings as a guide.We plan to do this in Pakpoon.
In summary,we found that 1)neighborhood food environment;2)social networks influencing obesity;and 3)knowledge,attitudes,and beliefs of those involved influencing lifestyle choices were the three main social determinants associated with obesity in the elderly in a community context.
This research may enable health care professionals, caregivers,and older people in similar settings or contexts-who are all faced with similar living situations as the people in Pakpoon-to realize that high-sugar and high-lipid diets are not the only factors in obesity.The most important factor is,in fact,the social aspect,and“people networks” reinforce obesity in older adults who cannot shed weight as easily and are more influenced by other people in their immediate environment.
Central governments, policy makers, and health professionals worldwide must take action on the social determinants of obesity to support community nurses in delivering effective nursing care plans.When social determinants of obesity are understood, interventions are more effective.Therefore, the ultimate aim is to develop effective health policies and impact solutions that suit the needs of the aged,caregivers,and specific local communities.
6.Limitations
The sample size in this study was limited to 19 people(n =19).While this sample was adequate for an initial exploration of the social determinants of obesity, further research is needed with a larger field sample to validate initial results.In addition, more research should be conducted with a larger cohort across several communities to provide a more comprehensive perspective.Sampling participants from a wider geographical area that includes other regions in Thailand or other communities in other countries should also be considered to address any potential political,geographical, or societal biases in participants’ responses.This would allow results to be extrapolated in a wider geographical and social context with greater confidence so that nurses worldwide can rely on the results.
Two female interviewers conducted the current research.Future studies and interviews should be conducted by both male and female researchers to ensure that any potential gender biases on the part of the current researchers are mitigated[31].
CRediT authorship contribution statement
Pornchanuch Chumpunuch:Conceptualization,Data Curation,Formal Analysis, Funding Acquisition, Investigation, Methodology,Project Administration, Resources, Software, Supervision, Validation, Writing - original draft, Writing -reviewing and editing.Urai Jaraeprapal:Conceptualization, Data Curation, Formal analysis,Investigation, Methodology, Project administration, Resources,Software, Supervision, Validation, Writing- original draft, Writingreviewing and editing.
Declaration of competing interest
The authors have declared on conflict of interest.
Funding
Funding for this research study was provided by the Thai Health Promotion Foundation.Furthermore, the Excellence Center of Community Health Promotion, School of Nursing, Walailak University will fund publication fees should this article submission be accepted for publication.No funding was granted for English language editing.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors wish to thank the Chief Editor, Heather Michelle Taylor of First Person Editing Limited (Wh¯angarei, New Zealand),for contributing to this research by providing English language assistance and proofreading this article.Heather Michelle Taylor has provided permission to be listed as a contributor.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2022.02.005.
杂志排行

International Journal of Nursing Sciences的其它文章
- Effects of mindfulness meditation on trait mindfulness, perceived stress,emotion regulation,and quality of life in hemodialysis patients:A randomized controlled trial
- Application of rational emotive behavior therapy in patients with colorectal cancer undergoing adjuvant chemotherapy
- The effect of slow deep breathing relaxation exercise on pain levels during and post chest tube removal after coronary artery bypass graft surgery
- The association between frailty of older stroke patients during hospitalization and one-year all-cause mortality:A multicenter survey in China
- Translation and piloting of the Chinese Mandarin version of an intensive care-specific pressure injury risk assessment tool (the COMHON Index)
- Adaptation and validation of pediatric peripheral intravenous catheter insertion and care practices audit tools