One-year outcomes and predictable factors for microhook ab interno trabeculotomy
2022-04-19DaikiSakaiMasashiFujiharaSatoshiYokotaMakotoNakamuraYasuoKurimoto
INTRODUCTION
Trabeculotomy is an established surgical procedure for patients with glaucoma. The supposed mechanism of intraocular pressure (IOP) reduction is through relieving the resistance of aqueous humor (AH) flow by the cleavage of trabecular meshwork (TM) and the inner wall of the Schlemm's canal (SC). Trabeculotomy expectedly achieves a mild reduction in IOP, compared to trabeculectomy,which is the gold standard surgical treatment for glaucoma.Nonetheless, the former is associated with a low frequency of vision-threatening complications such as hypotony and blebrelated infection, which can be attributed to its blebless profile.Conventional trabeculotomy uses theapproach.However, the currently trending procedure of minimally invasive glaucoma surgery (MIGS) uses theapproach, sparing the conjunctiva and sclera. The mainstream procedure for MIGS is the trabecular bypass procedure, which is classified into the following groups: 1) removal of the TM and inner wall of the SC (trabeculectomy and 2) cleavage of the TM and inner wall of the SC [trabeculotomy (μLOT)]. While the former category utilizes the trabectomeand Kahook Dual Blade, the latter involves gonioscopy-assisted transluminal trabeculotomy (GATT)and microhook μLOT. μLOT is a novel surgical procedure developed in Japan as an option for MIGS. A short surgical time (<10min) and low surgical cost requiring no expensive devices are the strengths of μLOT. Moreover, based on safety profile, μLOT is permitted in wide variety of cases.Thus, it is considered a promising treatment option for patients with glaucoma requiring surgical intervention. Despite the increasing popularity of μLOT, few reports describe its surgical outcomes. For optimal indications, information that predicts outcomes is required. The purpose of this study is to investigate the one-year outcomes in consecutive cases and factors that influence the results of μLOT.
SUBJECTS AND METHODS
This retrospective, single-center, observational study was performed according to the Declaration of Helsinki.It was approved by the Institutional Review Board of the Kobe City Medical Center General Hospital (Kobe, Japan). We applied the opt-out methods to obtain informed consent for this observational study involving the use of medical records.Patients who did not give their consent were excluded.
We enrolled consecutive patients who underwent μLOT at the Kobe City Eye Hospital between February 2018 and July 2019. Both μLOT alone and combined with cataract surgery were included. Indications for μLOT were the followings: 1) open angle glaucoma patients who had early to moderate glaucomatous damage; 2) requiring a reduction in IOP or in reliance on glaucoma medications while avoiding filtering surgery. There was no strict protocol and the decision to operate was at the discretion of each surgeon. If both eyes underwent μLOT during the recruitment period, only the first one was selected. We included all types of open angle glaucoma, regardless of the history of glaucoma surgery.Patients with a follow-up of less than 1mo were excluded.
图13结果显示,优化后的刀片1上的扭矩为1.22 N·m;刀片2上的扭矩为1.4 N·m;刀片3上的扭矩为1.45 N·m。可见,采用方案3(异形刀片)进行优化后,刀片上的扭矩均比原方案小,达到了节能的效果,但是相比优化方案2(弯曲刀片),方案3中的3片刀片上的扭矩变化平稳,均未出现波动情况。
Previous studies have reported that the μLOT is effective for various types of glaucoma including POAG, EXG, uveitic glaucoma, steroid-induced glaucoma, developmental glaucoma,and secondary glaucoma following vitrectomy.However, limited studies compared the effectiveness of μLOT among different types of glaucoma. According to Rahmatnejad, the success rates of GATT were not significantly different between POAG and SOAG eyes (including EXG eyes). While, Aktasreported that patients with POAG who underwent GATT had a higher percentage of IOP reduction compared with those with SOAG (including EXG) at 18mo postoperatively. Tanitoreported that steroid-induced glaucoma and developmental glaucoma might be good candidates for μLOT by performing multiple regression analysis. Our study added that POAG, which had a one-year surgical success rate of 80.0%, might be a good candidate for μLOT. There were no significant differences in the mean postoperative IOP and the number of glaucoma eye drops between the POAG and SOAG eyes that did not require additional surgery. This result suggests there are some populations of SOAG eyes which could achieve IOP reduction equivalent to that of POAG eyes. Additionally, our result showed that uveitic glaucoma had poor one-year surgical success rate, although the sample size was too small. Future studies involving large number of each type of SOAG patients are required to evaluate the effectiveness of μLOT for SOAG.Regardingtrabelulectomy, some studies have reported a higher success rate or greater IOP-lowering effect of trabectome surgery in EXG eyes compared to that in POAG eyes, which were not consistent with our results. While μLOT comprises the cleavage of the TM and inner walls of the SC, trabectome surgery includes the ablation and removal of the strip of the TM and the inner wall of the SC. Tingdescribed that the effect of trabectome surgery on washing out the exfoliation materials may lead to favorable results in EXG eyes. The difference in the surgical procedure may reflect as discrepancies between the surgical results of trabectome surgery and μLOT. Tojorecently reported trabectome surgery had significantly better surgical results compared with μLOT for glaucoma patients including various types of glaucoma. Comparisons of surgical outcomes for specific type of glaucoma are expected to determine the optimal indications oftrabeculotomy, because the best candidate for these two surgeries might be a different type of glaucoma. To identify the good candidate for μLOT is useful for clinicians because μLOT has the benefit in terms of surgical costs.
2)在恒温热风干燥和分阶段控温热风干燥两种方法下,辣椒干燥后的品质相差不大,但是在分阶段控制温度条件下,辣椒达到安全含水率的总干燥时间普遍较短,即其干燥速率较快、干燥能耗较低。试验所得最优的干燥辣椒的工艺是:分阶段控制温度热风干燥,初始温度为45℃,150min后迅速升温至60℃,风速为1.2m/s,辣椒达到安全含水率的总干燥时间为420min。
We performed the μLOT as previously reported. The Swan-Jacob Autoclavable Gonioprism or Ocular Hill Surgical Gonioprism (Ocular Instruments,Bellevue, WA, USA) were used to observe the anterior chamber (AC) angle opposite to the corneal port. We inserted the Tanitotrabeculotomy micro-hook (Inami,Tokyo, Japan) into the AC through the corneal port. The tip of the micro-hook was inserted into the SC and circumferentially moved to incise the TM and the inner wall of the SC. Surgeons could select any of the straight-type (M-2215S) or angledtype (M-2215R, M-2215L) microhooks. The position, number of corneal port incisions, and subsequent incision range of the TM were at the discretion of each surgeon. Although the incision range of the original method from Tanitowas approximately 240 degree, the incision range of 120 degree was recently reported in some studies; both methods were included in our cases.
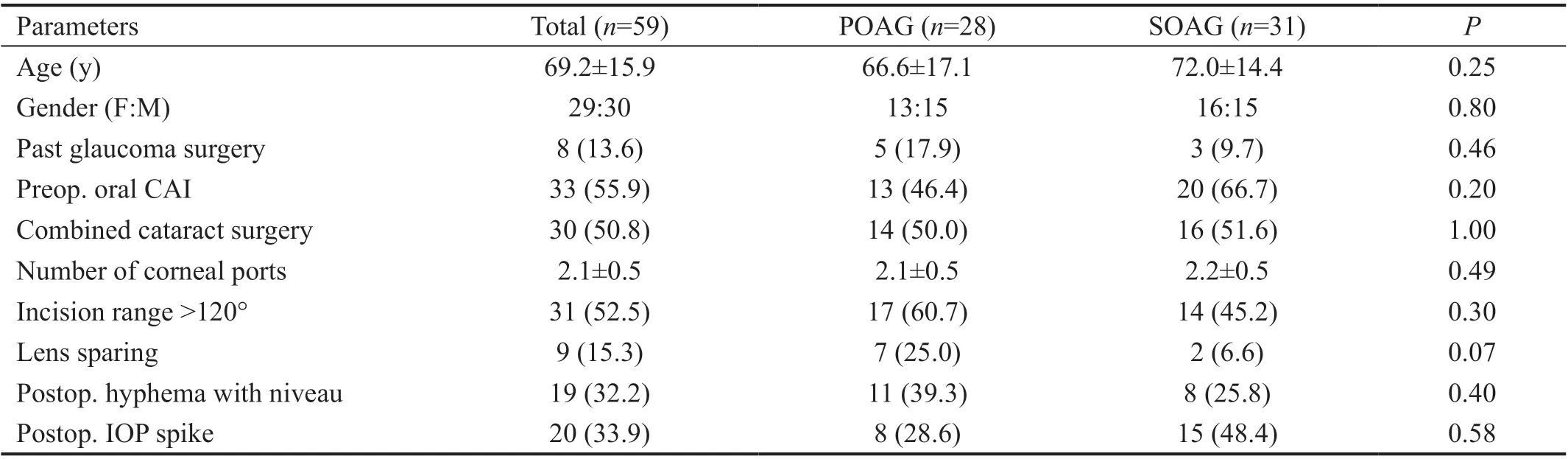
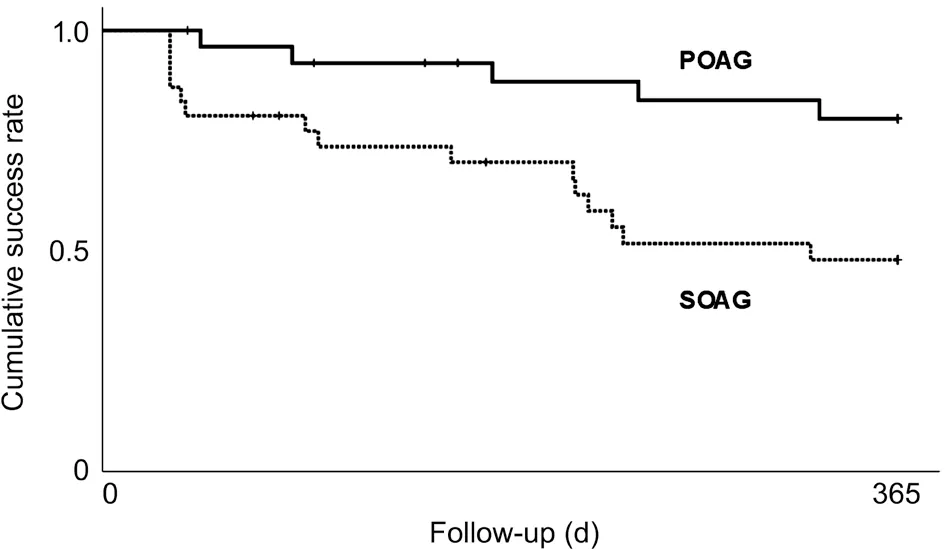
There was no substantial difference in the clinical characteristics and perioperative factors between the POAG and SOAG eyes(Table 1). The one-year cumulative rate of surgical success was significantly higher in POAG eyes than that in SOAG eyes (80.0%48.0%,=0.011, log-rank test; Figure 2). EXG,uveitic glaucoma, steroid-induced glaucoma had one-year cumulative surgical success rate of 63.5%, 16.7%, and 53.3%,respectively. After μLOT, the mean IOP and the number of glaucoma eye drops significantly decreased at 1wk, 3 and 12mo postoperatively in both POAG and SOAG eyes (all<0.01), and there was no significant difference between the POAG and SOAG eyes in IOP and the number of glaucoma eye drops at any point (Tables 2 and 3).


RESULTS
We performed multivariate analyses to detect the factors associated with failure, and the presence of a postoperative IOP spike was revealed as an independent risk factor. Postoperative IOP elevation or IOP spike is a common complication of trabeculotomy, which is often ascribed to a micro-apparent hyphema or postoperative inflammation. TM reportedly has the greatest resistance throughout the outflow of AH. AH initially exits the eye through the TM into the SC. It enters the collector channel opened along the external wall of the SC in the distal outflow. It then moves through the intrascleral plexus, eventually leading to the aqueous and episcleral veins where the AH joins the systemic circulation. Following μLOT,postoperative IOP elevation is presumed to be a consequence of an impaired distal outflow. Thus, pre-existing obstruction or constriction of the distal outflow pathway prevents the eyes from having enough drainage capacity to withstand the surgerymediated additional stress. Postoperative IOP elevation may occur in these eyes even with mild postoperative hyphema or inflammation. Thus, the presence of postoperative IOP spike is presumed to indicate poor drainage capacity of the eyes.Rahmatnejadinvestigated the factors influencing the surgical results of GATT and revealed a significantly higher rate of postoperative IOP spike (defined as IOP>30 mm Hg) in the surgical failure groups than in the surgical success groups.μLOT and GATT are classified in the same category of μLOT.Therefore, the results of our study and those of Rahmatnejadmay have similar underlying mechanisms. We speculate that postoperative IOP spike is not only a common complication of μLOT, but also a factor associated with surgical failure.
We conducted repeated measures analysis of variance (ANOVA) and paired-test with Bonferroni correction to compare the pre- and postoperative values. We divided the eyes into two diagnostic categories based on the type of glaucoma: primary open angle glaucoma (POAG) and secondary open angle glaucoma (SOAG) including exfoliation glaucoma (EXG). We performed unpaired-test or Fisher's exact test to compare the values between the two diagnostic categories (POAG and SOAG). Kaplan-Meier survival curves with log-rank tests were used to assess the cumulative rate of surgical success. We truncated all patients at 365d postsurgery, with a follow-up greater than 1y, because the majority of censoring occurred after one-year of follow-up visit.Associations between the surgical failure and collected factors were assessed using a multivariate Cox proportional-hazards regression model. We included all statistically significant variables on univariate analyses in the multivariate analyses.value <0.05 was considered statistically significant. All statistical analyses were performed using SPSS for Windows software package, version 25 (SPSS Inc., Chicago, IL, USA).
近3年来,在新入科的CSSD护士培训中,通过实行PDCA循环管理法,使新入科护士的专业技能和知识得到明显提高,全部都按标准按时按质完成培训。
对Kinect采集到的20个三维关节点坐标进行行为特征提取时选择的特征量应满足平移不变性及缩放不变性,角度特征很好的满足了以上两个条件。为了方便计算角度将20个关节点分别用“A”-“O”进行标记,对应关系见图2,其中A(Head),T(HandLeft),P(HandRight),L(FootLeft),H(FootRight)5个关节点由于会发生抖动现象[6],所以并未使用。
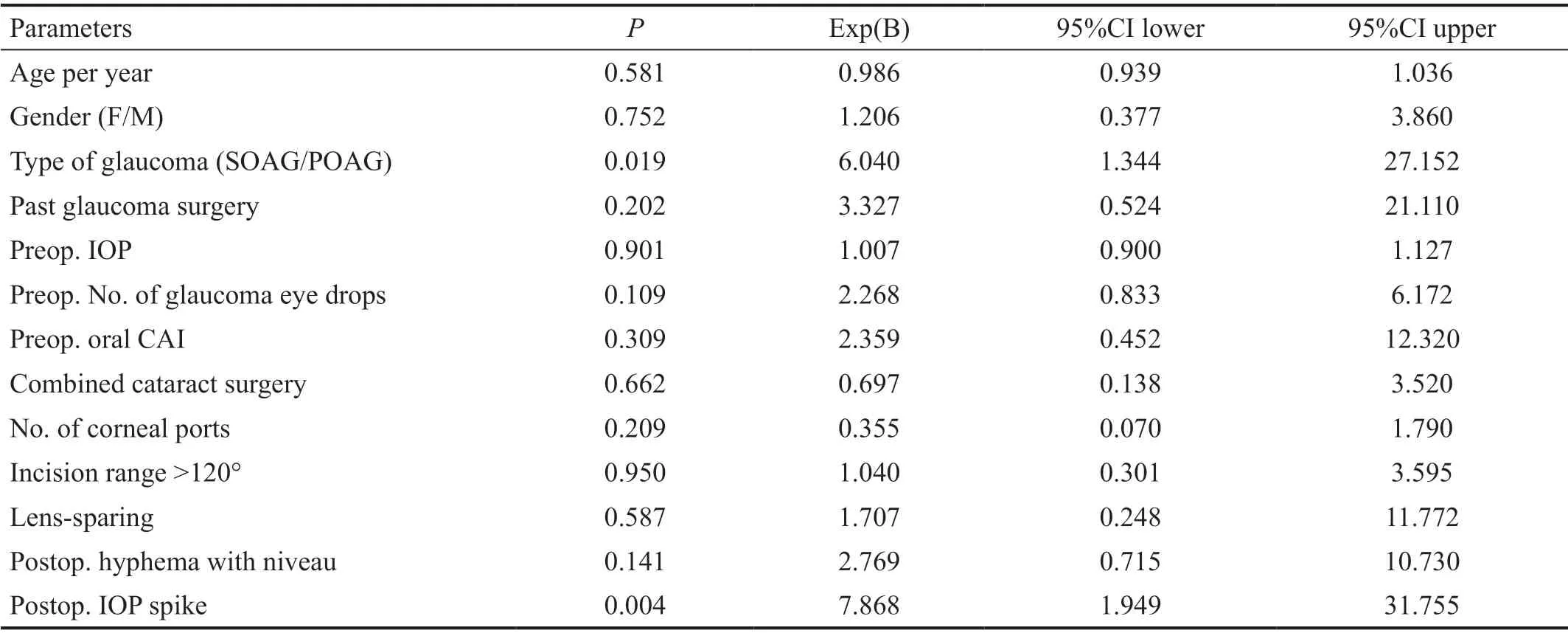
The results of univariate analyses revealed SOAG (=0.019) and postoperative IOP spike (=0.004) as potential factors (Table 4). Both of SOAG[=0.017, adjusted hazard ratio (aHR): 3.468, 95%CI: 1.246-9.654] and postoperative IOP spike (<0.001, aHR: 5.382,95%CI: 2.113-13.707) were independent factors associated with surgical failure in multivariate analyses (Table 5).

There were only two cases of postoperative complications requiring interventions, and both were hyphema(washout at 2 and 7d postoperatively). Vitreous hemorrhage occurred in three eyes post-surgery. However, it improved spontaneously without causing any visual impairment. There were 20 cases of postoperative IOP spike, which were treated by resuming glaucoma eye drops (=10) or oral CAI (=5)or both (=4). Patients did not receive routine antiglaucoma medications to prevent postoperative IOP spike, although two cases with relatively advanced visual field defect received preventive oral CAI. Seventeen eyes needed additional glaucoma surgery during the follow-up period. The indication of additional surgery was uncontrollable IOP elevation resistant to maximum medical antiglaucoma therapy (=16)and progression of visual field defect despite good IOP control(=1). While 12 eyes underwent standard trabeculectomy, 5 underwent additional μLOT.
DISCUSSION
Our study presents the one-year surgical outcomes and some factors associated with surgical outcomes of μLOT in consecutive cases of open angle glaucoma. The IOP and number of glaucoma eye drops had significantly decreased from baseline at the one-year follow-up visit. The mean postoperative IOP of 16.1±4.4 mm Hg was comparable to that previously reported by Moriof 17.8±6.3 mm Hg. Although there were some cases with postoperative complications which caused transient visual impairment, all of them improved spontaneously or were treatable with minor interventions.Regarding the types of glaucoma, POAG eyes achieved better one-year outcomes compared to SOAG eyes. Additionally,our results of multivariate analyses revealed SOAG eyes and postoperative IOP spike as the factors associated with surgical failure of μLOT.
We collected data on IOP and the number of glaucoma eye drops at the preoperative visit and each postoperative follow-up visit. Postoperative follow-up interval of each case was decided by each surgeon (5mo was the longest), and the postoperative data were collected at one week postoperatively, one month postoperatively, and monthly after that (if available). Furthermore, we collected the following clinical characteristics and perioperative factors for analyses:age, sex, type of glaucoma, history of glaucoma surgery,preoperative use of oral carbonic anhydrase inhibitor (CAI),combined cataract surgery, postoperative lens status, number of corneal ports for trabeculotomy, intraoperative incision range of TM, presence of postoperative hyphema with niveau, and IOP spike. We defined an IOP spike as an IOP exceeding 25 mm Hg at any follow-up IOP measurements within 2wk post-surgery.
The IOP and the number of glaucoma eye drops at each postoperative follow-up visit were the primary outcome measures. Surgical failure was defined as failure to meet the following target criteria of surgical success on two consecutive visits: 1) IOP≤21 mm Hg or 2) IOP≤ the preoperative IOP with a reduced number of glaucoma eye drops. The need for additional glaucoma surgery was also defined as failure. We recorded the first consecutive visit as the time of failure in all cases. Considering the postoperative IOP fluctuations after trabeculotomy, the surgical failure judgment was delayed up to 30d post-surgery. However, the cases requiring additional glaucoma surgery within 30d post-surgery were defined as failure on the day of second surgery (one patient). If the patients underwent additional glaucoma surgery, we excluded all follow-up measurements of the IOP and the number of glaucoma eye drops after the second surgery. The secondary outcome measures were the factors associated with surgical failure and postoperative adverse events.
反复使用的竹签存在许多的卫生隐患,服务人员不注意卫生操作规范、没有卫生的储存条件,就可能让各种细菌存活,而大肠杆菌、沙门氏菌等不是开水一烫就能够烫死的,带有细菌的竹签会对食客身体健康造成严重威胁。
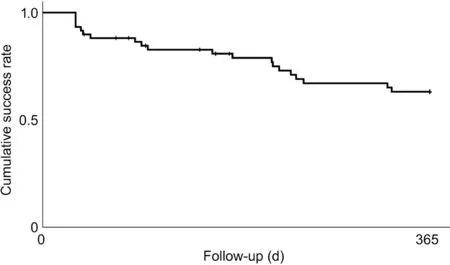
A total of 59 eyes of 59 patients were included in the study.The mean age was 69.2±15.9y, and the patients comprised 29 women. Twenty-eight eyes were POAG and 31 eyes were SOAG. Out of the 31 SOAG eyes, 18 eyes were EXG and the remaining 13 were other secondary glaucoma [uveitic (=6),steroid-induced (=5), after pars plana vitrectomy (=1),traumatic (=1)]. Four eyes had a history of trabeculotomy, 1 eye had a history of trabeculectomy, and 3 eyes had a history of selective laser trabeculoplasty. Table 1 summarizes the clinical characteristics and collected perioperative factors.There was a significant difference between the IOP measurements (<0.01, repeated measures ANOVA), and the mean IOP significantly decreased from 25.3±7.2 mm Hg preoperatively to 19.5±8.1 1wk postoperatively (<0.01), to 17.8±6.3 mm Hg 3mo postoperatively (<0.01), and to 16.1±4.4 mm Hg 12mo postoperatively (<0.01; Table 2). There was also a significant difference between measurements of the mean number of glaucoma eye drops (<0.01, repeated measures ANOVA),and the mean number of glaucoma eye drops significantly decreased from 3.9±1.1 preoperatively to 1.2±1.7 1wk postoperatively (<0.01), to 2.8±1.7 3mo postoperatively(<0.01), and to 2.1±1.8 12mo postoperatively (<0.01;Table 3). The overall cumulative surgical success rate at 12mo post-surgery was 63.1%. Figure 1 outlines the Kaplan-Meier survival curve for all cases.
Limitations of our study include its retrospective nature,limited sample size, multiple surgeons, mixture of standalone and cataract-combined surgery, and a short follow-up time.Additionally, there was no strict protocol to standardize the indications of interventions. We presumed our surgical success rate to be relatively inferior to those of previous reports. This can be attributed to the inclusion of consecutive patients,regardless of the type of glaucoma or past surgical history.Future prospective studies with the protocol of surgical indications and procedures involving a larger sample size with longer follow-up time are needed.
In conclusion, μLOT is a good treatment option for POAG eyes. However, the postoperative course should be carefully followed in cases with postoperative IOP spike.
RAPD标记技术是出现最早的分子标记技术之一,其操作简便、成本较低及不需要DNA的序列材料等特点是其他标记技术无法比拟的[7]。但RAPD标记也存在某些不足,其中最主要的是其灵敏度高,受反应条件影响较大,检测的重复性较差,因此,研究者在利用RAPD标记技术进行遗传多样性分析时一定要严格控制试验条件,采用稳定优化的反应体系方能取得理想的试验结果[8]。同时,在运用RAPD标记技术时,由于每个随机引物并不适合于所有物种,因此对引物的筛选是非常必要的,筛选出多态性丰富、稳定性好的随机引物是整个试验成功的关键[9]。
This study was partly presented at the 9World Glaucoma E-Congress 2021.
None;None;None;None;None.
猜你喜欢
杂志排行
International Journal of Ophthalmology的其它文章
- Comment on: Real-world outcomes of two-year Conbercept therapy for diabetic macular edema
- Efficacy of intravitreal conbercept combined with panretinal photocoagulation for severe nonproliferative diabetic retinopathy without macular edema
- Efficacy of conbercept after switching from bevacizumab/ranibizumab in eyes of macular edema secondary to central retinal vein occlusion
- lntraoperative complication rates in cataract surgery performed by resident trainees and staff surgeons in a tertiary eyecare center in Hungary
- Comparing surgical efficiencies between phacoemulsification systems: a single surgeon retrospective study of 2000 eyes
- Factors associated with corneal astigmatism change after ptosis surgery