Relationship between clinical remission of perianal fistulas in Crohn’s disease and serum adalimumab concentrations: A multi-center cross-sectional study
2022-03-15LauraSirmaiAnneLaurePelletierNathalieGaultCamilleZallotGuillaumeBouguenDominiqueBouchardPascaleRolandNicaiseMarinePeyneauSandrineSironneauMarceloDeCarvalhoBittencourtAntoinePetitcollinPedroFernandezXavierRoblinLaurentSiproud
Laura Sirmai, Anne-Laure Pelletier,Nathalie Gault, Camille Zallot, Guillaume Bouguen, Dominique Bouchard,Pascale Roland Nicaise, Marine Peyneau, Sandrine Sironneau, Marcelo De Carvalho Bittencourt,Antoine Petitcollin,Pedro Fernandez, Xavier Roblin, Laurent Siproudhis, Laurent Abramowitz
Abstract
Key Words: Crohn’s disease; Clinical pharmacology; Peri-anal disorders; Adalimumab
INTRODUCTION
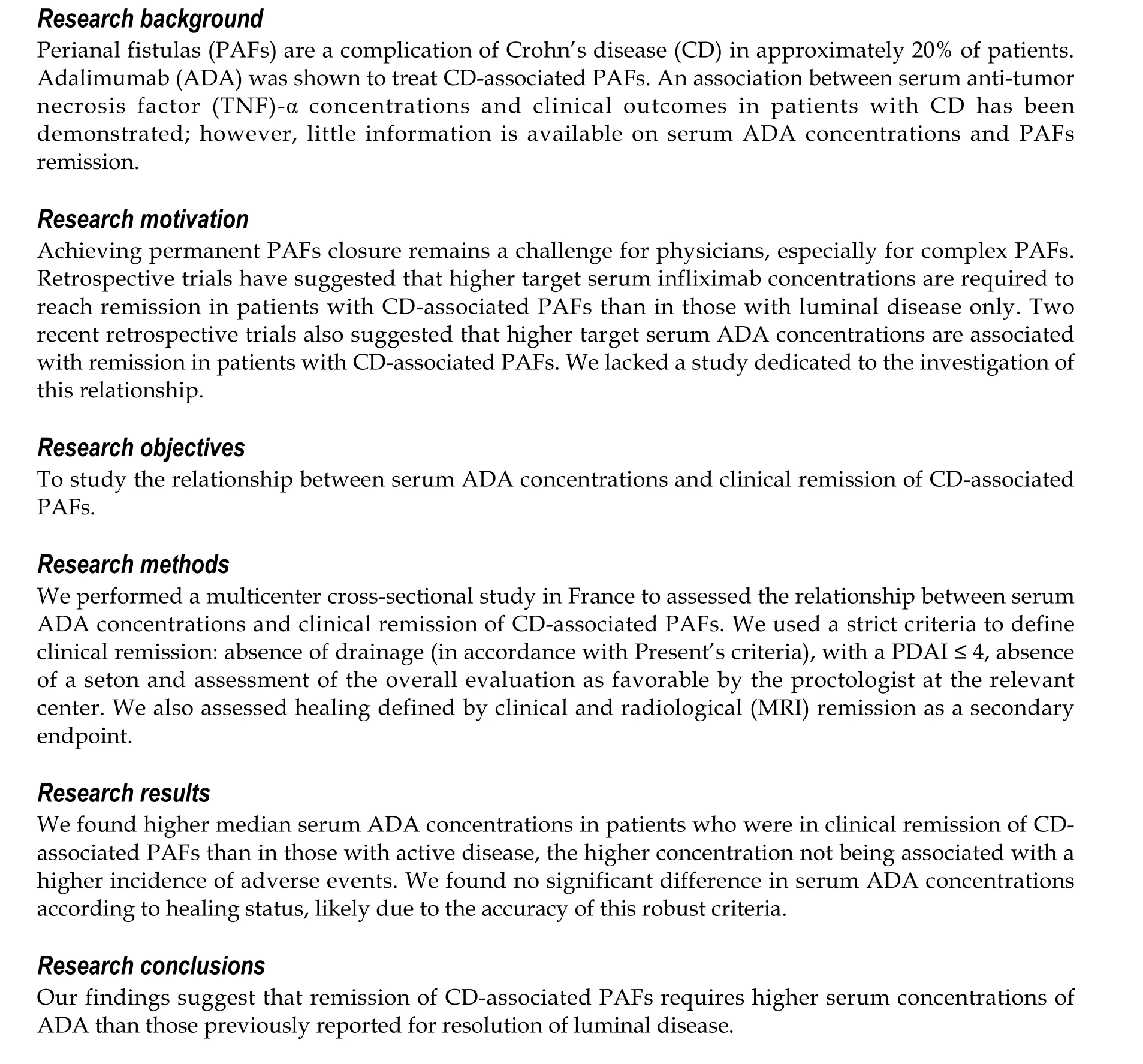
Crohn’s disease (CD) is complicated by perianal fistulas (PAFs) in approximately 20% of patients and these PAFs can severely and negatively affect patients’ quality of life[1]. Treatment of CD-associated PAFs was revolutionized by the advent of anti-tumor necrosis factor (TNF)-α antibodies[2]. A metaanalysis of treatment with adalimumab (ADA), a TNF-α blocker, found that complete PAF closure occurred in 36% of patients with CD-associated fistulas (95%CI: 0.31-0.41) and partial responses in 31%(95%CI: 0.031-0.61)[3]. Its efficacy is better in anti-TNF-α-naive patients but it can also be effective after infliximab failure[4]. Adding surgical drainage with a seton has been shown to be superior to anti-TNFα alone, with better responses and fewer recurrences[5,6]. Resolution of complex PAFs takes longer and timing of seton withdrawal depends on the effectiveness of the medical treatment and findings on clinico-radiological evaluation[5]. However, achieving permanent fistula closure remains a challenge for physicians.
Optimization of anti-TNF-α therapy (increasing the drug dosage and/or shortening the intervals between injections) is advised in patients with confirmed active disease, good compliance, and subtherapeutic drug serum concentrations in the absence of anti-drug antibodies[7]. Adding an immunosuppressive drug (in combination therapy) should also be considered[8]. Thus, optimization of treatment on the basis of anti-TNF-α (including ADA) and antibody serum concentrations has been evaluated[9-11]. Retrospective trials have suggested that higher target serum infliximab concentrations are required to reach remission in patients with CD-associated PAF than in those with luminal disease only[12-16]. Two recent retrospective trials also suggested that higher target serum ADA concentrations are associated with remission in patients with CD-associated PAF[15,16]. However, in those studies the evaluation criteria were mostly clinical, the studies were not confined to assessment of ADA, and they were small single-center studies. Our primary objective was, therefore, to study the relationship between serum ADA concentrations and clinical remission of CD-associated PAFs.
MATERIALS AND METHODS
Study cohort and setting
This cross-sectional study was conducted in four French centers between December 2013 and March 2018. Patients with at least one active CD-associated PAF at the time of ADA initiation, or who developed a PAF while being treated with ADA (thus requiring optimization of ADA), whose serum ADA concentrations were measured at least once during follow-up (induction or treatment maintenance) were considered eligible. The PAFs could be associated with upper, ileal, colonic, or rectal lesions. Patients who were eligible on the basis of the above criteria were included irrespective of the durations of their PAFs and ADA treatment, associated or previously received treatments, and surgical procedures performed, particularly the closure technique (glue, plug, or rectal advancement flap after removal of a seton). ADA treatment could have been optimized or not and an immunosuppressive drug may also be used in combination therapy. Pregnant or breastfeeding women and patients with a history of proctectomy or undrained abscesses were excluded.
Data collected and definitions
Data were collected between October 2017 and March 2018 using a standardized paper collection file.The clinical data collected at each evaluation were as follows: remission of any fistula, perineal disease activity index (PDAI) score, presence of associated lesions in the rectum or anus, durations of PAFs and seton drainage, Harvey Bradshaw score, ADA dosage and duration of treatment, associated treatment,and adverse events. Patient characteristics collected and assessed were as follows: treatment center; age;sex; body mass index; co-morbidities; smoking status; Montreal classification; and medical and surgical history (abdominal surgery, number of fistula(e); simple, complex, or vaginal involvement; and surgical treatments for the PAF, including the type of closure performed). Pelvic magnetic resonance imaging(MRI) and colonoscopy findings obtained within 3 mo of clinical evaluation and in the absence of more recent changes in treatment were collected if performed, which was at the discretion of the physician.MRI images were reassessed by a single expert radiologist (Fernandez P). ADA and anti-ADA antibody serum concentrations were measured in the laboratories of each investigating center using a standardized drug-sensitive ELISA test (Lisa Tracker; Theradiag, France) or equivalent immunologic test[17]. If more than one serum ADA concentration was available, the trough concentration (Day 13 or 14 after ADA injection) was used, as recommended in a recent published study[18]. Serum ADA concentrations were measured systematically or at the times of clinical evaluations in accordance with the standard procedures at the participating centers. Some serum ADA concentrations were reported as greater than 16 μg/mL; therefore, all measures were recorded to a maximum of 16 μg/mL.
The primary study endpoint was clinical remission of PAF, defined as the absence of drainage (both spontaneous and after soft pressure on the orifice by the clinician, in accordance with Present’s criteria[2]), with a PDAI ≤ 4, absence of a seton and assessment of the overall evaluation as favorable by the proctologist at the relevant center. This outcome was defined after agreement by experts from the Proctology Research Group of the French National Society of Colo-Proctology, the investigators being members of these groups. If one of the above criteria were absent, the PAF was described as active.Favorable evaluation by the proctologist was defined as no inflammation of external(s) and internal(s)orifice(s) and absence of current or new associated anal lesions (stenosis, ulceration, or fistulous branching) that had developed after introduction of ADA or the most recent change in modality of medical or surgical treatment. In patients with multiple CD-associated PAFs, all lesions had to have resolved to conclude the evaluation was favorable. The clinical remission criteria were reviewed at all evaluations.
The secondary study endpoint was healing, which was defined as clinical remission (as described above) plus radiological healing on pelvic MRI, this definition having been reached by agreement of the Proctology Research Group’s experts and as reported by other research groups[19,20]. The full criteria were absence of hypersignal T2 or enhancement after gadolinium T1 injection, absence of any abscess,and absence of rectal inflammation.
ADA optimization was defined as shortening of the interval between injections to 7 d or increasing the dosage of injections to 80 mg (or both).
Combination therapy was defined as addition of an immunosuppressive drug (thiopurine or methotrexate) to ADA.
Endoscopic luminal remission was defined by a score of less than 6 on the CD Endoscopic Index of Severity.
Clinical luminal remission was defined by a Harvey Bradshaw score of less than 4.
ADA tolerance was assessed on the basis of occurrence of adverse events.
The following definitions apply to terms used in the remainder of this article. Immunization was defined as undetectable serum ADA concentrations and the presence of anti-ADA antibodies in concentrations above 20 ng/mL[21].
Complex PAFs were defined as PAF branched in two or more directions or presence of ramifications or diverticula[5,22].
PDAI scores are based on the presence of fistula drainage, pain, and its effects on activity, limitations on sexual activity, degree of induration, and type of fistula. A score greater than 4 indicates definite active disease.
Statistical analysis
First, patients’ characteristics are reported according to occurrence of clinical remission. Quantitative variables are presented as median and interquartile range and categorical variables as frequencies and percentages. The overall number and proportion of patients achieving clinical remission, achieving healing, and having at least one adverse event were determined.
The distribution of durations of PAFs and drainage, ongoing treatment, and serum albumin and Creactive protein concentrations was further explored according to the clinical remission status at the time of evaluation.
The relationship between serum ADA concentrations and each of the following was assessed: clinical remission, healing, endoscopic luminal remission, clinical luminal remission, treatment optimization,and treatment with combination therapy. These relationships were studied using univariate generalized estimating equations models, considering an evaluation as the statistical unit (some patients having undergone several evaluations).
Association between serum ADA concentrations at each visit and clinical remission was also adjust on the duration of treatment.
All analyses were performed using R version 3.2.0. All tests were two-tailed, and the level of statistical significance was set atP= 0.05.
RESULTS
Patient characteristics
Of the 45 patients who were screened for inclusion, 34 were found to be eligible (9 from Paris, 8 from Rennes, 13 from Nancy, and 4 from Saint-Etienne), 16 of whom were women (47%). The remaining 11 patients were excluded for the following reasons: three for wrong diagnoses (two anal stenosis, one ulcerative colitis), three because they had undergone proctectomy, one was a minor, one had an undrained abscess, and three had PAFs that had resolved. Patients had between one and four evaluations (total of 56 evaluations), 50% of them having only one evaluation. Three of the 56 evaluations were performed during induction of ADA treatment.
Overall, 44% of the patients (n= 15) achieved clinical remission. Pelvic MRI was available for 23 of the 34 patients (56%) and showed that 17% (n= 4) had radiological evidence of healing. Of the patients in clinical remission, 44% had radiological evidence of healing.
Table 1 summarizes the characteristics of the participants that were collected at the first evaluation.Most of these characteristics were comparable between patients who achieved and did not achieve clinical remission (Table 1), particularly smoking status (43%vs47%) and previous treatment with biotherapies including infliximab (47%vs53%). More patients’ treatment was optimized at the first evaluation in patients who achieved clinical remission than in those who did not (60%vs42%). Patients who achieved clinical remission tended to have fewer complex PAFs (73%vs89%) and vaginal PAFs(7%vs21%) and they had colonic lesions less frequently (33%vs42%) Patients who achieved clinical remission tended to have undergone more fistula closure procedures than those who did not achieve remission (33%vs16%).
None of the six patients who achieved remission and underwent more than one evaluation relapsed.These evaluations took place between 3 mo and 4 years after the first evaluation. All patients in clinical remission from PAF were in luminal remission (established by clinical and endoscopic evaluation),whereas half of the patients who did not achieve clinical remission from PAFs had luminal activity. Of the 19 patients with active disease, three had immunization status regarding ADA, five had undrained branches detected by MRI indicating insufficient surgical treatment, and six had low serum ADA concentrations (< 4 μg/mL) that could probably have benefited from optimization. The remaining five patients may have truly failed ADA treatment after 6 mo of well-conducted treatment.
Adverse events
Five patients (14.7%) had at least one adverse event leading to ADA discontinuation. Two of them were in the clinical remission group (pancytopenia and joint pain of no definite cause) and the remaining three in the activity group (axonal neuropathy attributed to ADA and digestive, pulmonary, and ganglionic tuberculosis; vertigo; and joint pain).
Serum ADA concentrations and clinical remission
Median serum ADA concentrations were significantly higher in assessment visits of patients in clinical remission than in those not in clinical remission [14 (10-16)vs10 (2-15) μg/mL,P= 0.02 after adjustment on the duration of treatment] (Figures 1 and 2), with an area under the ROC curve of 65.6%. Clinical remission was not identified in the three evaluations of patients with immunization status regarding ADA.
The duration of treatment with ADA tended to be longer in the clinical remission than in the nonclinical remission group (37vs12 mo). The median duration of drainage with a seton was 8 mo in the clinical remission group compared with 9 mo in the non-clinical remission group (Table 2). The median duration of PAFs tended to be longer in the clinical remission than no clinical remission group (53 movs12 mo) (Table 2).
Serum ADA concentrations and healing
Median serum ADA concentrations did not differ significantly between evaluations in which healing(clinical and MRI remission) was identified and those in which it was not [11 (7-14)vs10 (4-16) μg/mL,P= 0.69].
Serum ADA concentrations and optimization or combination therapy
Serum ADA concentrations tended to be higher in patients whose treatment was optimized than in those whose treatment was not optimized [14 (5-16) μg/mLvs10 (4-13) μg/mL,P= 0.20] and in patients receiving combination therapy than in those receiving ADA alone [12 (5-16) μg/mLvs11 (5-14) μg/mL,P= 0.11]. Neither of these differences was statistically significant.

Table 1 Patients’ characteristics according to clinical remission status

Table 2 Characteristics of perianal fistulas at each visit according to the presence of clinical remission
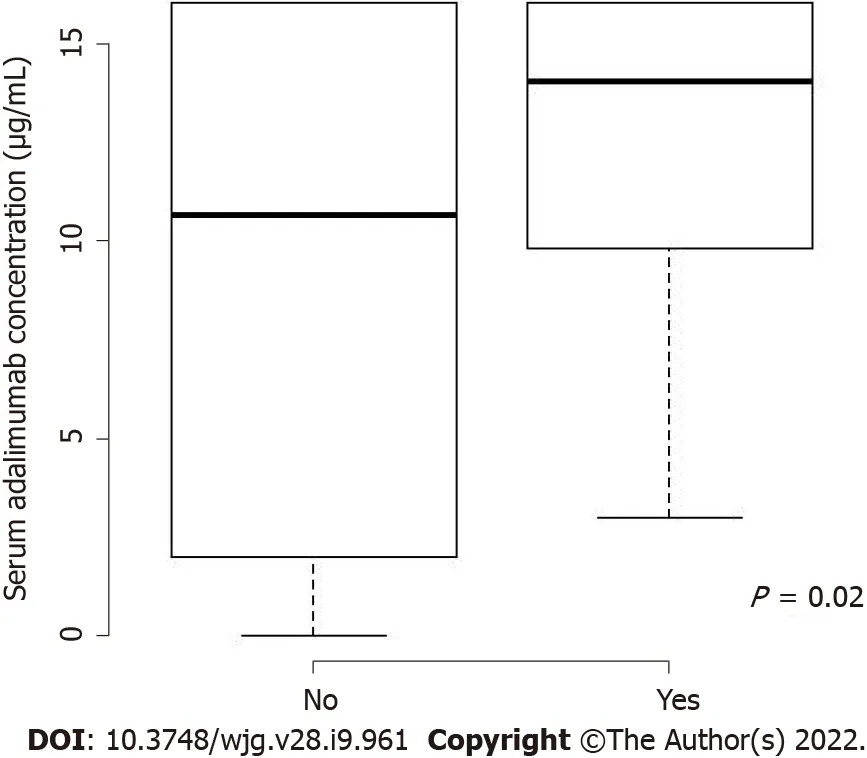
Figure 1 Serum adalimumab concentrations according to clinical remission status.
Serum ADA concentrations and luminal remission
Median serum ADA concentrations tended to be higher in patients with endoscopic luminal remission and in those with clinical luminal remission than in those without it [12 (6-16) μg/mLvs2 (1-4) μg/mL,and 14 (10-16) μg/mLvs4.2 (1-11) μg/mL, respectively].
DISCUSSION
In this study, we found higher median serum ADA concentrations in patients who were in clinical remission of CD-associated PAFs than in those with active disease, the higher concentration not being associated with a higher incidence of adverse events. To the best of our knowledge, this is the first multicenter study dedicated to investigating the relationship between serum ADA concentrations and remission of CD-associated PAFs. Our definition of healing of PAFs included clinical and MRI criteria,as recently recommended[5,20,22,25].
Our findings suggest that remission of CD-associated PAFs requires higher serum concentrations of ADA than those previously reported for resolution of luminal disease (between 4.5 and 12 μg/mL based on results of clinical trials)[9,10]. The high serum concentrations that we found to be associated with clinical remission seem to be more frequently achieved through optimization of ADA dosage or combination therapy (or both).
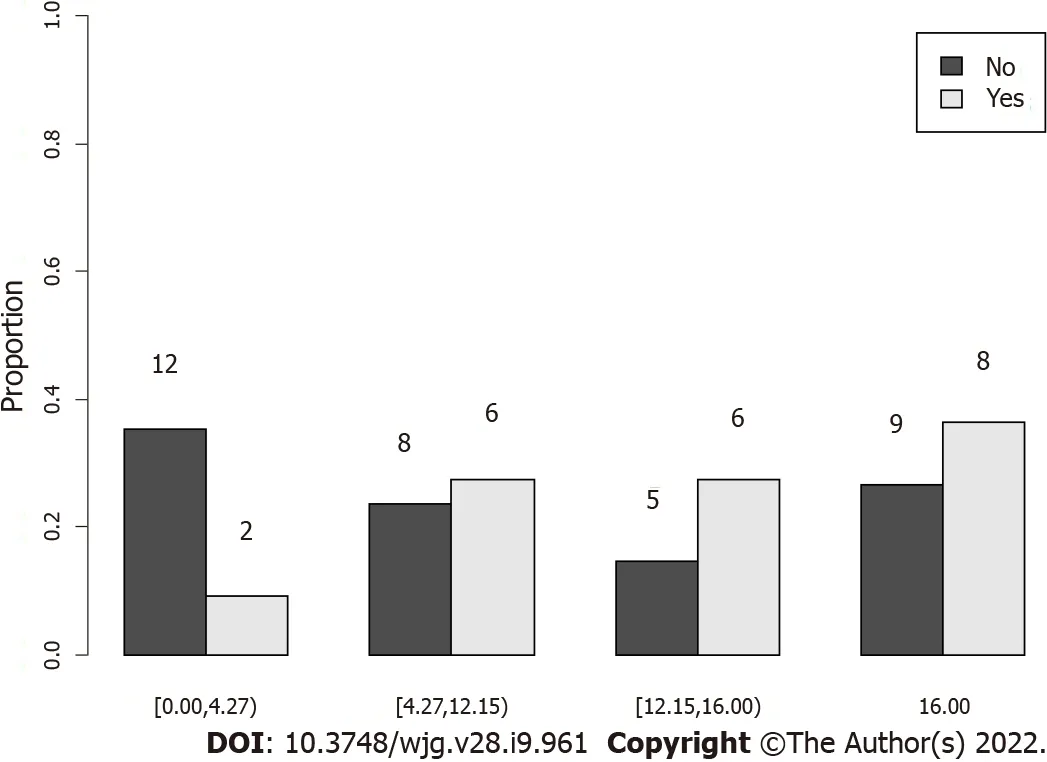
Figure 2 Clinical remission according to quartiles of serum adalimumab concentrations.
Serum ADA concentrations have shown considerable variability and overlap between patients with and without clinical remission, as previously described[9]. It is likely that not all patients need to reach these high concentrations. For patients not achieving remission, we suggest measuring serum ADA concentrations and antibodies to exclude immunogenicity issue. Optimizing ADA dosage or adding combination therapy (or both) should be considered, even if we do not have yet a concentration to target.
In our study, patients with active lesions had more complex PAFs (89%vs73%) and more vaginal fistulas, indicating the severity of the disease. No patients who achieved remission of PAFs had colorectal activity, highlighting the importance of achieving luminal remission when managing PAFs.
Four of the 23 patients (56% of the whole cohort) who had an MRI in our study achieved healing(17%).
Our low rate of healing of PAFs (clinical plus MRI remission) is likely attributable to our high rate of complex PAFs, the well-known delay between MRI remission compared with clinical remission(approximately 12 mo)[23], given that some follow up data were missing, and the fact that 44% of our patients did not undergo MRI evaluation.
We found no significant difference in serum ADA concentrations according to healing status [11 (7-14) μg/mLvs10 (4-16) μg/mL,P= 0.69]. We think the lack of statistical significance is attributable to our small sample size, and our low rate of healing of PAFs, likely due to the accuracy of this robust criteria.
We found that the PAF duration was longer in patients with PAF activity than in those in remission(53.5vs12 mo), which likely reflects failure of medical or surgical (or both) treatment.
The three patients with anti-ADA antibodies and undetectable serum ADA had clinically active disease, which is consistent with the findings of a previous study that showed that the presence of anti-TNF-α antibodies is a risk factor for disease activity and recurrence[24].
Recently, two retrospective trials[15,16] were performed to assess the relationships between concentrations of anti-TNF medications, including ADA, and outcomes of CD-associated PAFs. Their results are consistent with ours: Striket al[15] (19 patients treated with ADA) found significantly higher median serum ADA concentrations in patients with closed PAFs than in those with active PAFs [7 (6-11) μg/mLvs5 (2-6) μg/mL,P= 0.003]. Additionally, Plevriset al[16] (35 patients treated with ADA) found significantly higher median ADA concentrations in individuals with healed fistulas than in those with unhealed fistulas (12.6 μg/mL vs. 2.7 μg/mL;P< 0.01).
首先从犯罪主体的年龄上来说,必须是年满十六周岁的具有刑事责任能力的自然人,同时这里的醉酒需要达到一定的标准,如果不符合标准只能认定为“酒后驾驶”,达不到醉驾标准只需要承担相应的行政责任,而不需要承担刑事责任。其次,有些学者在该罪名主体的研究上,会将无证驾驶和醉酒驾驶进行某种程度上的混淆,因为我国新的道路交通法规定,无证驾驶的行为人需要处以一定的行政拘留和罚款,但是无证同时醉驾的行为人是不是构成醉酒型危险驾驶罪呢?笔者认为这个答案是肯定的。醉驾之所以受到处罚是出于对其行为的危害性考虑,跟其行为人有没有驾驶证并没有直接的影响,可以作为醉驾行为的一个严重结果。
Of note, our patients’ serum ADA concentrations were much higher than in these two studies.Possible explanations for this discrepancy are that more of our patients were receiving combination therapy or optimization of ADA treatment (or both) and we had a high rate of complex PAFs (82%),including 15% with vaginal involvement. One strength of our study is the very precise description of our study cohort and their PAFs (PAF complexity, the presence or absence of setons, and endoscopic data). We chose a stricter clinical definition of remission, incorporating PDAI scores, and a greater proportion of our patients underwent radiological evaluation (no MRIs in Plevriset alstudy and 15% in the Striket alstudyvs56% in our study), which has been shown to be very important in assessing healing of PAFs[25].
In our study, high serum ADA concentrations was not associated with an increased incidence of adverse events, knowing that we only took into account the serious adverse events leading to a stop of ADA. In the literature, Drobneet al[26] and Greeneret al[27] studies found that higher infliximab serum concentrations are not associated with a higher frequency of infections. Interestingly, Landemaineet al[28] study found that infection risk was individually correlated with cumulative increase in drug exposure, but not infliximab trough level.
Our study had several important limitations. Being a cross-sectional, non-interventional, nonrandomized study, management of patients was heterogeneous both in terms of surgical and medical treatment. Additionally, most data were collected retrospectively. However, it was an evaluation of management of CD-associated PAFs in real life in tertiary centers. We had a small sample size, as did the other two available studies, because of the competition of other biotherapies. Trough serum ADA concentrations were not always measured; thus, it is possible that ADA concentrations fluctuated between injections[18]. Timing of measurement of serum ADA concentrations was either systematic or clinically oriented, depending on the center, favoring non-responders or partial responders. With an area under the ROC curve that was close to 50%, we could not identify target serum ADA concentrations associated with clinical remission using the Youden index. Additionally, half of the patients had only one evaluation, limiting the availability of follow-up data.
CONCLUSION
In conclusion, there is an association between clinical remission of CD-associated PAFs and high serum ADA concentrations that is not associated with an increased incidence of adverse events. Our data suggest that higher ADA concentrations are associated with remission of CD-associated PAFs than in mucosal healing. Target serum ADA concentrations to guide physicians should be determined by a prospective trial.
ARTICLE HIGHLIGHTS
Research perspectives
Target serum ADA concentrations to guide physicians should be determined by a prospective trial.
ACKNOWLEDGEMENTS
We thank Jodi Smith, PhD, and Dr Trish Reynolds, MBBS, FRACP for editing a draft of this manuscript.We thank Toni Alfaiate for statistical advices.
FOOTNOTES
Author contributions:Sirmai L is the Guarantor of the article; Sirmai L conceived the study together with Pelletier AL and Abramowitz L; Fernandez P read the MRI images; Sirmai L, Pelletier AL, Zallot C, Bouguen G, Bouchard D,Roland Nicaise P, Peyneau M, Sironneau S, De Carvalho Bittencourt M, Petitcollin A, Roblin X, Siproudhis L, and Abramowitz L collected data; Gault N performed statistical analyses; all authors commented the article and approved the final version of the article, including the authorship list.
Supported bythe Assistance Publique des Hôpitaux de Paris and AbbVie (North Chicago, Illinois, United States).
Institutional review board statement:The study was reviewed and approved by the CNIL (N° CERFA 13810*01).
Conflict-of-interest statement:Sirmai L reports having received grant support from Abbvie and congress invitations from Roche and Sandoz and having received conference or consultancy fees from Gilead, MSD, Abbvie, Mayoly Spindler, Takeda, Ipsen, Allergan France and Ferring; Pelletier AL reports having received grant support from Abbvie and financial support from Ferring; Zallot C reports having received financial support from Takeda, Abbvie,Ferring, Janssen and Pfizer; Bouguen G reports having received lecture fees from Abbvie, Ferring, MSD, Takeda and Pfizer and consultant fees from Takeda, Janssen, Mylan and Abbvie; Bouchard D reports having received speaking fees from Abbvie, MSD and Janssen, consultancy fees from Takeda, and congress invitations from Abbvie, Pfizer and Takeda; Gault N, Roland Nicaise P, Peyneau M, Sironneau S, Bittencourt M, Petitcollin A, Fernandez P all declare they have no conflicts of interest; Roblin X reports having received financial support from Abbvie, Amgen, Pfizer,Takeda, Janssen, MSD and Theradiag; Siproudhis L reports having received conference or consultancy fees from Gilead, MSD, Abbvie, Mayoly Spindler, Takeda, Ipsen, Allergan France and Ferring; Abramowitz L reports having received grant support from Abbvie and financial support from Takeda.
Data sharing statement:No additional data are available.
STROBE statement:The authors have read the STROBE Statement-checklist of items, and the manuscript was prepared and revised according to the STROBE Statement-checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:France
ORCID number:Laura Sirmai 0000-0002-8627-8155; Anne-Laure Pelletier 0000-0003-4055-7615; Nathalie Gault 0000-0002-9913-9760; Camille Zallot 0000-0003-0993-6983; Guillaume Bouguen 0000-0002-7444-5905; Dominique Bouchard 0000-0003-0984-8545; Pascale Roland Nicaise 0000-0001-7137-135X; Marine Peyneau 0000-0002-5554-0835; Sandrine Sironneau 0000-0002-5656-7917; Marcelo De Carvalho Bittencourt 0000-0002-2698-2458; Antoine Petitcollin 0000-0003-4811-0439; Pedro Fernandez 0000-0001-8410-1623; Xavier Roblin 0000-0002-7929-4878; Laurent Siproudhis 0000-0002-2575-6790; Laurent Abramowitz 0000-0002-5106-4317.
S-Editor:Chang KL
L-Editor:A
P-Editor:Chang KL
猜你喜欢
杂志排行
World Journal of Gastroenterology的其它文章
- Radiomics-clinical nomogram for response to chemotherapy in synchronous liver metastasis of colorectal cancer: Good, but not good enough
- Applications of endoscopic ultrasound elastography in pancreatic diseases: From literature to real life
- Postoperative morbidity adversely impacts oncological prognosis after curative resection for hilar cholangiocarcinoma
- Cystic fibrosis transmembrane conductance regulator prevents ischemia/reperfusion induced intestinal apoptosis via inhibiting PI3K/AKT/NF-κB pathway
- Dualistic role of platelets in living donor liver transplantation: Are they harmful?