Relationship of Aboriginal family wellbeing to social and cultural determinants, Central Australia: ‘Waltja tjutangku nyakunytjaku’
2022-03-04AlysonWrightVanessaNapaltjarriDavisMakaylaMayBrinckleyRaymondLovettJoanneThandrayenMandyYapWilliamSandersEmilyBanks
Alyson Wright , Vanessa Napaltjarri Davis, Makayla- May Brinckley, Raymond Lovett, Joanne Thandrayen, Mandy Yap, William Sanders, Emily Banks
ABSTRACT
INTRODUCTION
Public health and primary healthcare develop—ments increasingly recognise the importance of family in the health of individuals.1Inter—ventions based on theoretical underpinnings in social epidemiology demonstrate that fami—lies are an asset for the development, mainte—nance and restoration of health.2—4Families also provide the social emotional support needed to foster children’s development. A recent review of Aboriginal and Torres Strait Islander wellbeing concepts identified that family was considered the most important factor for overall wellbeing.56McCalmanet alfound that family— centred primary health—care interventions generated clinical health outcomes for Indigenous children, led to greater parent satisfaction with the service and wider community utilisation of health—care services.7Others have described that importance, prioritisation and value placed on attending to social relationships and responsibilities and learning ‘respect’ as underpinning Aboriginal culture and knowledge.89
International and Australian research demonstrates links between family functioning and social determi—nants, but there is little research on associations between functioning of a family and cultural determinants, partic—ularly among adults. This is despite the clear concep—tual linkages in family and culture. Family is the support structure and the basis to which people understand their social networks and relations, and the world. A quality within Aboriginal worldviews is the concept of family goes beyond immediate family, to those related by skin group names, kinship and social structures10and are based on both biological and social networks. Extended family and grandparents (particularly grandmothers) often have critical roles in the caring for children.11In this context, it can be problematic to consider family as constituting only household members,12because households can contain multiple families and families can extend beyond the household. Recent evidence from a sample of Aboriginal adolescents in Victoria demonstrated higher wellness was associated with participants who grew up in their Aborig—inal family and community, and conversely institutionally imposed family displacement was associated with lower odds of being well.13
The importance and value of family to Aboriginal people’s wellbeing is juxtaposed against a dominant deficit narrative of Aboriginal families and parents in the public arena. The most lurid of these was Leak’s obscene comic of an Aboriginal man holding a beer, unaware of his son’s name.14The son was being held by a police officer who suggested that the father talk to his son about ‘personal responsibility’. The comic, called out as racist by Indigenous leaders across the country, was defended by the newspaper’s editor, “Leak’s confronting and insightful cartoons force people to examine the core issues…”.15Aboriginal people are met with the narrative of dysfunctional families on a daily basis.1617These depictions and imagery can have implications for health service delivery, as they foster racial bias, rein—force stereotypes and promote prejudices which can influence clinician responses and overall care.18—20At a 2018 launch ofIn My Blood It Runs, a movie depicting the life of Dujaan, a 10— year— old living at Ewyenper— Atwatye camp in Alice Springs (Northern Territory, Australia),Dujaan’s mother, Megan Hoosan, commented “I just want Australia to know that we love and care for our kids”.21Her sentiment appeared to reflect an exhaustion with the deficit narrative and a resilience to speak back against it.
This paper aimed to apply a strength— based approach to explore the relationship of high family functioning to the cultural and social determinants for Aboriginal people in Central Australia. The analysis and interpretations involved the participation of Aboriginal organisations,their Aboriginal Directors and community researchers.The co— design and review process is consistent with Indig—enous ethical research approaches and principles.22
METHOD
Setting
This work was conducted in Central Australia, a site which self— nominated to participate based on estab—lished research partnerships, and importantly, a region of profound historical injustices and ongoing discrimi—nation for Aboriginal language groups and people. The region of Central Australia is remote; it contains two main service towns (Alice Springs and Tennant Creek)and a number of remote Aboriginal communities. Most Aboriginal people live in (or maintain connections with)communities where they are surrounded by family. The locations of communities are closely aligned with ances—tral country and support the ability to foster cultural knowledge transmission. However, remote communi—ties often have serious deficits in physical and health infrastructure. They can also be physically remote from services (for example, high schools and hospitals) and infrastructure (for example, mobile phone towers).23The Aboriginal population in this region have consider—able health and social disparities when compared with the Aboriginal population in other parts of Australia and with general Australian population.24
Further, Central Australia is marked with historical and recent intervention by the state, including the 10— year effort to ‘mainstream and normalise’ remote Aboriginal communities, under policies such as Northern Territory Emergency Response and the National Partnership on Remote Service Delivery. These policies were premised on government priorities to reduce social inequities across education, income levels, employment and health,but have been largely ineffective in achieving greater parity.2526Government policy decision and funding prior—ities dominates the service delivery environment, at the same time Aboriginal people’s capacity regionally and locally to be self— determined is supported by the Aborig—inal Land Rights Act Northern Territory and the large Aboriginal community controlled sector. Notably though,Aboriginal governed agencies are outside of the tiers of government decision— making and Aboriginal people’s struggle for a legitimate voice in the state’s decision—making systems remains ongoing.27
Despite challenges to self— determination and service delivery in this setting, several influential projects have arisen from Aboriginal research partnerships. In partic—ular, this current study was influenced by 2008 concep—tual work of senior Aboriginal women from a partner organisation, Waltja, in Central Australia that explained the foundations to family. This work documents four principles:Tjukurpa,Ngura,Kanyini,Waltja(defined table 1) for growing up children and identifies rela—tionships and responsibilities between people, animals,land and spirituality.28With guidance from Waltja, we used this conceptual frame in the analysis of cultural determinants.
The Mayi Kuwayu Study
Mayi Kuwayu
Mayi Kuwayu, the National Study of Aboriginal and Torres Strait Islander Wellbeing is a longitudinal cohort study of Aboriginal and Torres Strait Islander adults aged 16 years and over.29Participants were recruited through a multimode approach including mail— out survey (using the Medicare Enrolment Database), in— community,online and social media, over— the— phone and word of mouth. Questionnaires were self— completed on paper or online, or completed with assistance from community researchers. The Mayi Kuwayu Study has over 20 Aborig—inal and Torres Strait Islander partner communities around Australia.
Community oversight and review
Community partnerships were key in determining the research question being answered here and interpreting the findings. Waltja and Tangentyere had initially been involved in Mayi Kuwayu Study community— based survey recruitment and were keen for the Study results to generate meaningful findings for communities in Central Australia. At initial meetings with Waltja and Tangen—tyere, Aboriginal directors were asked to identify research areas of interest and it was at these first meetings that a project on family and culture was identified, including the suggested use of the conceptual frame described above. Following the analysis, we undertook workshops with community participants and governance groups to discuss preliminary results. This involved structured discussions on the results with Waltja Board of Direc—tors (August 2020, May 2021) and with the Tangentyere Research Hub staff (November 2020, May—June 2021).The research team used these discussions to inform the interpretations of results and in describing the research implications. Quotes and observations from these stake—holder discussions are incorporated in the Results and Discussion sections of the paper to contextualise findings.
Study population and inclusion criteria
The region of Central Australia was selected for this study in negotiation with community partners. Quantitative data in this analysis were from the Mayi Kuwayu Study baseline survey (Data Release 4.0) and are based on self—reported responses to the questionnaire. Participants were included in the analysis if they lived in the Central Australian region (n=639/9691) as defined by partic—ipant’s postcode (online supplemental table 1). Addi—tionally, qualitative data from workshops with Aboriginal leaders in key partner organisations, many of whom had also completed the baseline survey, are included in this paper.
Outcome variable
The Mayi Kuwayu Study family functioning measure is a validated, modified scale of family functioning from the Western Australian Aboriginal Children Health Survey.3031The measure has recently been validated by Mayi Kuwayu research team, including the development of quartile cut— points applied in this paper.30Participants responded to nine items regarding their family, “In my family: We get on together and cope in hard times; We celebrate special days and events; We talk with each other about the things that matter; We are always there for each other; We manage money well; We have common inter—ests; People are accepted for who they are; We have good support from mob); We have family knowledge and tradi—tions that we pass on our children”. The response options are as follows: ‘not at all’ (coded as 1), ‘a little bit’ (2),‘a fair bit’ (3), ‘a lot’ (4), ‘unsure’ (recoded as missing).For participants who responded unsure or missing to one item, an imputed value (the mean of their other eight family functioning items) replaced the missing or unsure.Total family functioning score was derived by summing responses for the nine items, and categories are based on quartile cut— points established in the work by the Mayi Kuwayu research team to validate the measure30and in line with the original family functioning scale.31
The categories are low (9 to ≤24), medium (>24 to≤29), high (>29 to ≤33) and very high (>33 to 36). Cate—gories were collapsed to a binary outcome for the regres—sion analysis: low/medium (9 to ≤29) and high/very high(>29 to 36). These categories were determined based on findings from the validation study of the family func—tioning measure.30
Exposure variables and covariates
We examined the relationship between family func—tioning and a range of cultural and social indicators identified in the literature as conceptually related family wellbeing and functioning.283233Cultural measures were specifically linked toAnanguterms developed by Waltja in previous conceptual research (table 1).28The cultural measures include community cohesion, individual agency,exposure to cultural practice, first language, time spent speaking your Aboriginal language, lives on country, time across your life spend on country, know tribe’s country,knows skin name and knows your mob.
The social measures were household composition,household size, crowded housing, number of children in the house, family financial status, employed, welfare recip—ient and highest level of education. Age group (16—35,36—55, ≥56) and gender (male, female) were treated as covariates. Specific details on variables are reported in online supplemental table 2.
Statistical analysis
Scores for family functioning items (percentage and number) are presented. Total family functioning scores and their distribution across categories and demographic factors are presented.
We used binomial regression to calculate prevalence rate ratios (PRs) and 95% CIs for each exposure in rela—tion to the binary family functioning categories. Models were restricted to participants with data on the outcome of interest. Models are presented unadjusted, and then adjusted for age group and gender, as these factors were identified a priori as potential confounders of the rela—tionship between the outcome of family functioning and cultural and social factors. PR was selected as the measure of association in the statistical analysis over OR because the outcome family functioning was common.
We tested the sensitivity to models using both family functioning score with no imputation and the imputed score for one missing or unsure item. Results were not materially different after changing the method of calculating the family functioning measure (online supplemental table 3). Cells with <5 observations were confidentialised, with the exception of cells for the missing category (which pose no risk of identification).An alpha level of 0.05 was the threshold for statistical significance. Data were analysed in Stata V.16.
Ethics
This study was approved by the Central Australian Human Research Ethics Committee (19— 3315) and the Australian National University Human Research Ethics Committee(2019/19). Participation in the Mayi Kuwayu Study is voluntary and all participants provided consent. Partic—ipants involved in follow— up workshop provided written consent and all written outputs were provided to partner organisations for review and approval prior to submitting for publication. The Mayi Kuwayu Study is Aboriginal and Torres Strait Islander led and governed, and conducted with ethics approvals from jurisdictional Human Research Ethics Committees and relevant Aboriginal and Torres Strait Islander organisations. Data access to Mayi Kuwayu data was approved by a data governance committee.
RESULTS
Responses to family functioning items and sample characteristics
The highest proportion of responses were to the following statements: ‘We are always there for each other’ (72.1%reported ‘A lot’), ‘We have family knowledge and tradi—tions that we pass on to our children’ (65.4% report ‘A lot’), ‘We have good support from mob’ (62.6% reported‘A lot’) and ‘People are accepted for who they are’ (62.0%reported ‘A lot’) (table 2). Of all 639 participants, 515 had full answers to the family functioning items and an additional 48 participants had only one unsure or missing(total sample with family functioning score=563), 76 participants were missing (11.9%). The majority (57.9%,n=370) of participants had either high (26.1%, n=167) or very high (31.8%, n=203) family functioning, and 13.3%(n=85) recorded a low family functioning score.
The sample with full responses to family functioning measure was characterised by more women than men(table 3) but there was no observable gender difference in the proportion of participants in each family functioning category (table 4). There were similar proportions by agegroup and household size categories. The sample was also characterised by large sized households with a mean number of 6.9 people per household and mean number of 2.6 children, 25.2% of participants (n=142) reported having 7—9 people living in the house and 36.1% (n=203)had at least 3 children. Most households were classified as a multigenerational (33.6%, n=189) or extended family household (25.8%, n=145). A total of 14.6% of house—holds were nuclear family (n=82) and only 2.1% (n=12)were single person households.

TabIe 2 Responses to family functioning individual items and overall, Central Australian participants
The large household sizes and high proportion of extended family or multigenerational households were confirmed by Waltja Directors, as one Director responded:
We have big families and we live with lots of people…We all live together and that’s what keeps those fam—ily connections so strong. It’s a part of culture living together, being together and always being there for each other.
Arrangements can change between families and house—holds with people moving between houses and shifting roles in family, particularly in relation to caring for kids.This was summarised by one Waltja Director who shared:
There is a fluidity around Aboriginal families. There are a lot of extended family members involved in the care of the children—that’s how it works. It’s mainly grandmothers who do a lot of active caring for kids,but it can also be sisters, uncles, and aunties…. These are often informal arrangements, just discussed day by day but it’s important to recognise all the people involved as[in] growing up and raising the kids.
Relationship between family functioning and social factors
High family functioning was associated with financial situ—ation and household composition. Higher family func—tioning was associated with high family financial status compared with lower family financial status (aPR 0.74,95% CI 0.60 to 0.91) and not being on welfare compared with being on welfare (0.88, 0.77 to 1.00) (table 4). High family functioning was also positively associated with living in an extended or multigenerational family (1.19,1.02 to 1.38) compared with nuclear family household.We did not observe a significant statistical relationship between high family functioning and larger household size, greater number of children in house, less family or community worries, being employed or considering your house to be overcrowded.
Relationships between family functioning and cultural factors
There were positive associations between family func—tioning and a number of cultural domains. Family func—tioning was associated with a strong sense of belonging(Kanyini) represented by higher levels of community cohesion (aPR 2.72, 95% CI 1.68 to 4.39) and higherindividual agency (2.15, 1.63 to 2.85), with a dose response found in these relationships (table 5). Addition—ally, within theAnangudomain ofTjukurpa,higher family functioning was associated with exposure to cultural prac—tice and knowledge (1.45, 1.28 to 1.65), speaking your Aboriginal language as your first language (1.20, 1.04 to 1.37) and speaking your Aboriginal language a lot (1.37,1.12 to 1.68). These findings were discussed with the Directors:

TabIe 3 Sample characteristics of Central Australian participants and by categories of family functioning categories
I feel we are living and doing this culture work in our family programs at Waltja. We start our work with young people in the bush. We take them on country and sit them down. We give them space, and we teachthem culture by being on country. But it’s always hard to get this recognised by our funders. We can get a program to address alcohol easily, but what we need is a healing pathway back to our culture, back to the community and back to our elders teaching.
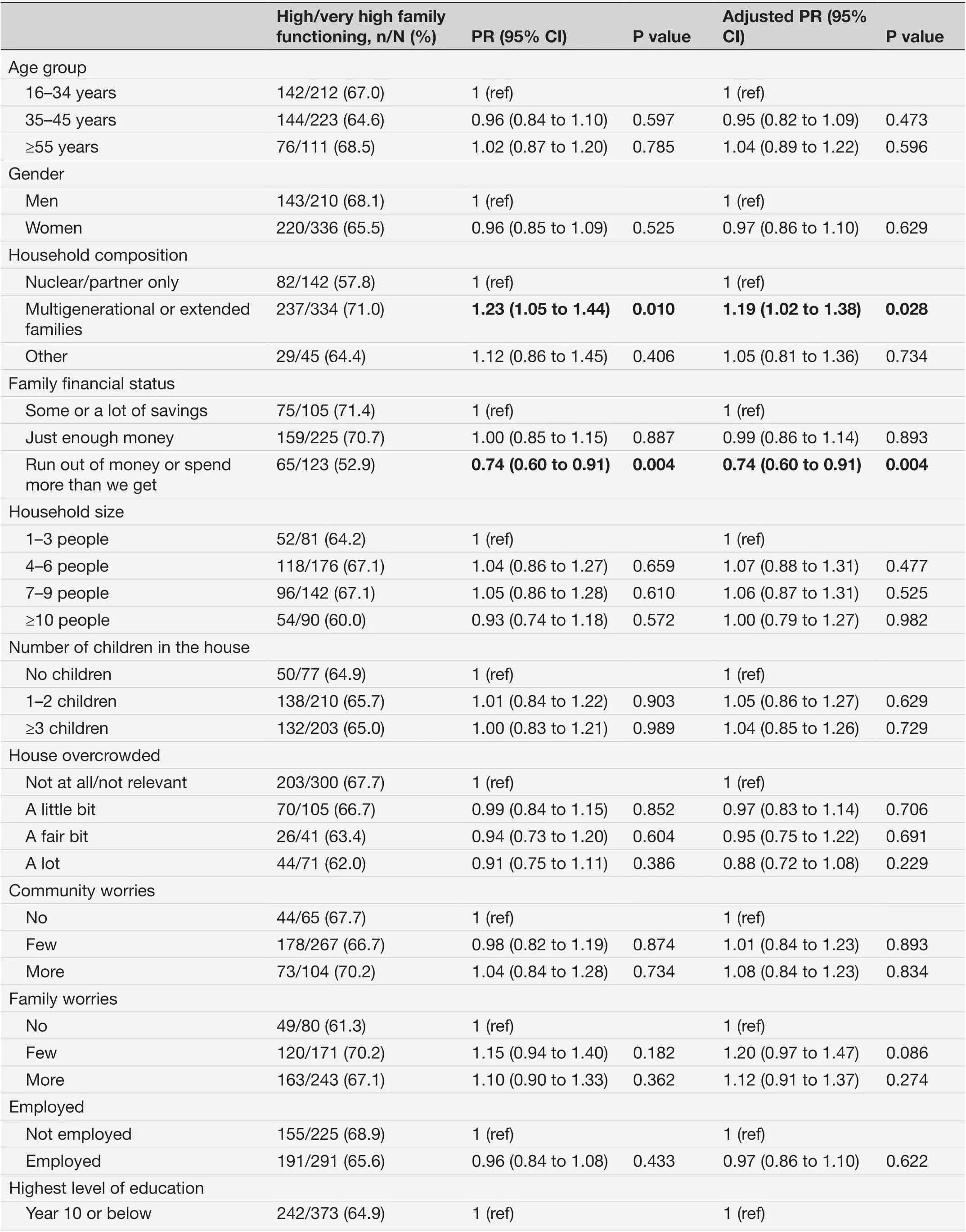
TabIe 4 Associations between high family functioning and social determinants among Mayi Kuwayu participants, Central Australia

TabIe 4 Continued
We did not observe a significant statistical relation—ship between high family functioning and living on your country; spending time on country; knowing your skin name; having cultural responsibilities for country;other family speaking language; knowing your mob;and knowing your mob’s country. One Waltja Director observed:
I think it’s [the research is] sort of boxing things up:culture, land, language, as individual things you see.This Kanyini, Ngura, Waltja and Tjukurpa, they are all connected. For one to flourish, you need to have the other parts. I think this is a good story, but I am thinking about the connections, how one thing is re—lated to another and what it means, Anangu way.
DISCUSSION
The overwhelming majority of Central Australian partici—pants reported high family functioning, with no observed differences in family functioning by age, gender or house—hold size. The importance of respect and caring in the family is attested by the high proportion of participants who responded ‘A lot’ across the positive individual family functioning items and the overall high propor—tion with high/very high family functioning. High family functioning was associated with cultural factors such as knowing and speaking your Aboriginal language, higher community cohesion, high cultural practice and higher individual agency. Consistent with prior evidence, the findings indicate that culture and family are recognised strengths of Aboriginal communities534—38contrary to the deficit framing of family in the media. These results in part are driven by a very unique ‘social structure of Indigenous communities’ and systems of connectedness and kinship which define relations between individuals,families and communities.5Wilson provides an important summary of this signalling “…the relational way of being is at the heart of what it means to be Indigenous” (Wilson,p80).39
Waltja’s framework (Tjukurpa,Kanyi,Walta and Ngura)for working with family and children suggest that these relationships are not simply about people, but encom—pass relationships with land, spirituality and Indige—nous knowledge.40While we did not find an association between connection to country measures and family functioning, feedback from Waltja Directors suggest that people’s connection with country is a critical backbone in supporting other cultural factors, including learning kinship responsibilities and understanding Aboriginal law (Tjukurpa). A lack of statistical significance does not mean no association; the small sample may mean that some associations were not detectable. Given the explor—atory nature of this study, the comments from Aboriginal collaborators are particularly pertinent as they suggest there are complex and potential multidirectional rela—tionships between and among the cultural determinants and family functioning, warranting further longitudinal investigation among the Mayi Kuwayu Study cohort. The findings warrant further exploration with the national level data to explore differences and similarities based on remoteness geography.
Of the social factors considered in this paper, house—hold composition, family financial status and receiving welfare were associated with high family functioning.A potential novel finding of this study is that living in a multigenerational or extended family household was associated with higher family functioning compared with living in nuclear household. As identified by Waltja Directors, there is potentially an underlining link back to culture because households containing multigenerational or extended family may be in a better position to facil—itate cultural knowledge transfer and teaching and use of Aboriginal language than less diverse households. This warrants further research and investigation, including better understanding why we observed an association in household composition and family functioning, but did not find this in relation to household size or perceived overcrowding. Given that reducing overcrowding and household sizes is pursued by primary healthcare experts as a response to high infections rates of commonpreventable disease (for example trachoma, rheumatic fever, otitis media and most recently COVID— 19),41—43there is a need to better understand and address tensions that arise between Aboriginal preferences in living among large family groups, and the guidance provided in clinical primary and public healthcare.44The nexus between housing and primary healthcare delivery needs to consider the importance of family, environmental health and the factors that contribute to wellbeing. This includes understanding the mechanisms that culture and family may have in reducing health inequities.
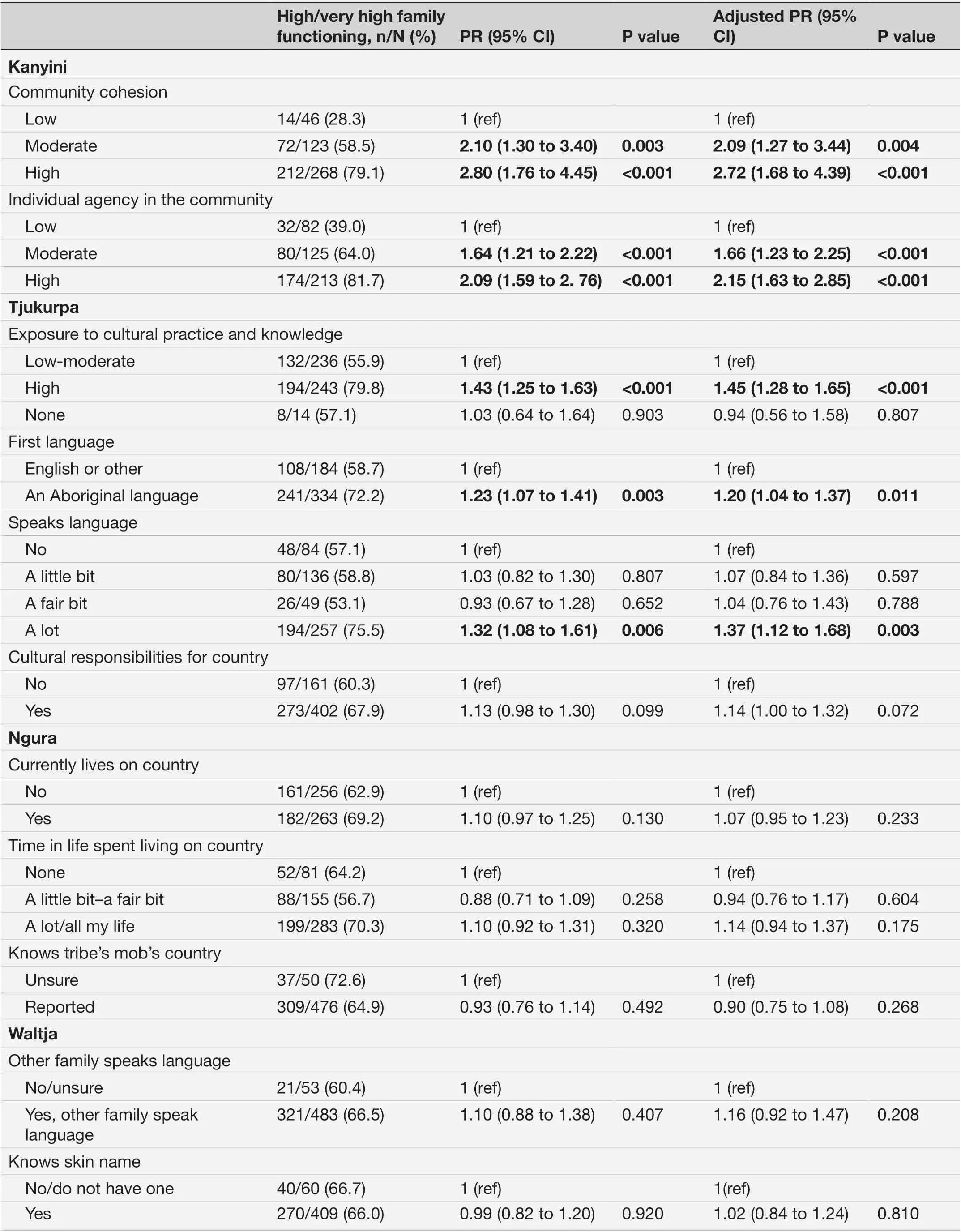
TabIe 5 Associations between high family functioning and cultural determinants among Mayi Kuwayu participants, Central Australia

TabIe 5 Continued
Consistent with other research, lower family func—tioning was associated with receiving welfare and lower family financial status.4546Low income results in consider—able stress on families47and could be compounded in the context of Central Australia by poorer social housing and infrastructure conditions.44Further, the levels of socioeco—nomic disadvantage experienced by Aboriginal families may mean the scale of benefit from increased household incomes are considerable in this context compared with urban locations.24Importantly, our findings are consis—tent with others who have argued that supporting Aborig—inal families requires more than just improvements in social conditions48and is deeply connected with cultural determinants.
This study is the first quantifiable evidence from Central Australia demonstrating important associations between high family functioning and aspects of culture.The strength associated with Aboriginal families and culture provides an alternative narrative to the deficit public discourse. Working in partnership with Aborig—inal leaders in this research has led to a deeper and more nuanced consideration of the findings that highlight complexities in how social and cultural determinants relate to family functioning. It seems important that future analysis give consideration to the interconnections between various factors of culture rather than simply their independent associations with family functioning.Further, the observed associations do not imply causality,and several aspects warrant further investigation to deter—mine causal pathways. A limitation of the study is the non— random sampling strategy used by Mayi Kuwayu and the potential clustering of individual respondents in the same household or community, which was not accounted for in the analysis. This may mean the prevalence is over—estimated as survey respondents are more likely to have positively responded to questions about their family rela—tions. Despite this, there is considerable diversity of the participants in the sample and it is one of the largest recorded samples for a study of the Aboriginal popula—tion in Central Australia. The sample size was sufficient to allow adjustment for age and gender across the asso—ciations explored, demonstrating no material changes in the findings. It is likely that similar findings may be found for other regions of Australia and potentially other Indig—enous and First Nations groups globally; given the novel findings presented, further analyses at the national level are warranted.
Overall, being responsive to families and the commu—nity is a fundamental principle of primary healthcare as it was originally conceived.49As such, there is a need to think more broadly about how primary health can extend beyond clinical services and what investments could support this. This paper suggests working with fami—lies and with culture can support wellbeing outcomes.This finding reinforces what others have described as the critical need for Aboriginal— led services. Applying this principle to comprehensive primary healthcare requires services to establish a deeper connection with the Aboriginal culture, family and community which may already being occurring in some Aboriginal Community Controlled Health Services despite a lack of investment.Future research working with the Aboriginal Commu—nity Controlled Health Services is needed to identify case studies that demonstrate these ways of working. Integra—tion of the family and community into healthcare services may be part of the transformative change needed to better serve Aboriginal and Torres Strait Islander people across the healthcare sector. The wellbeing benefits asso—ciated with cultural and social outcomes for Aboriginal and Torres Strait Islander peoples are enough to warrant strong government commitment and investment. Such investment should include rigorous research and evalua—tion to optimise the impacts on people.
CONCLUSION
This study found high family functioning among Aborig—inal people in Central Australia, despite the impact of considerable health and social inequalities. Given the enormous power of state decision— making over Aborig—inal lives, the family is a unit which bonds individuals and collectively provides a source of empowerment. Family functioning is interconnected with a number of cultural and social determinants. Building on foundations of culture and family is likely to be an important approach to improving wellbeing in this region and could be better used in the delivery of primary healthcare services for Indigenous peoples.
AcknowledgementsThe authors acknowledge all Aboriginal and Torres Strait Islander peoples and their continuing connection to culture, land and seas. This work was primarily undertaken on Arrernte Country and we acknowledge the Traditional Owners of this Country, who have remained strong custodians of their land despite the impacts of colonisation and associated trauma. We are grateful to the participants of Mayi Kuwayu from Central Australia and Directors and Researchers involved in the workshops and feedback session. We extend our thanks to Waltja Tjutangku Aboriginal Corporation, Tangentyere Council and the Mayi Kuwayu Data Governance Committee who provided guidance, engaged with the content of the study and approved outputs prior to submission for publication.
ContributorsThe authors contributed to study in the following manner: study design (RL, AW, VND); analysis (AW, M- MB); drafting manuscript (AW); interpretation(AW, VND); statistical review (JT, EB); revision to manuscript (all authors).
FundingThe Mayi Kuwayu Study was supported by the National Health and Medical Research Council of Australia (ref: 1122273). AW is supported by an Australian Government Research Training Program Scholarship and an ANU Dean’s Award Scholarship. RL and EB are supported by the National Health and Medical Research Council of Australia (reference numbers 1088366 and 1136128,respectively).
Competing interestsNone declared.
Patient consent for publicationConsent obtained directly from patient(s)
Ethics approvalThis study involves human participants and was approved by Australian National University Human Research Ethics Committee (Ref Number:2016/767), Central Australian Human Research Ethics Committee (Ref Number:19- 3315). Participants gave informed consent to participate in the study before taking part.
Provenance and peer reviewNot commissioned; externally peer reviewed.
Data availability statementData may be obtained from a third party and are not publicly available. The Mayi Kuwayu dataset is governed by senior Aboriginal people based on principles of Indigenous data sovereignty. Requests on data access can be made to the Mayi Kuwayu Data Governance group.
Author note‘Waltja tjutangku nyakunytjaku’: Luritja language meaning ‘to be surrounded by family’.
Supplemental materialThis content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer- reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines,terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Open accessThis is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially,and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
ORCID iDAlyson Wright http://orcid.org/0000-0001-7321-8922
杂志排行
Family Medicine and Community Health的其它文章
- COP27 climate change conference:urgent action needed for Africa and the world
- General practitioners’ (GPs) experience,attitudes and needs on clinical genetic services: a systematic review
- Impact of COVID- 19 infection rates on admissions for ambulatory care sensitive conditions: nationwide difference- in- difference design in Japan
- Healthcare use among people with diabetes mellitus in Europe: a population- based cross- sectional study