The East–West Divide in Response to COVID-19
2021-12-25DeanJamisonKinBingWu
Dean T. Jamison*, Kin Bing Wu
a Department of Epidemiology and Biostatistics, University of California, San Francisco, CA 98158, USA
b Independent Consultant, Atherton, CA 94027, USA
Keywords:Coronavirus disease 2019 Isolation Non-pharmaceutical interventions Pandemic Vaccination
ABSTRACT Coronavirus disease 2019 (COVID-19) deaths per million population in the countries of the West had often exceeded those in the countries of the East by factor of 100 by May 2021. In this paper, we refer to the West as represented by the United States plus the five most populous countries of Western Europe (France, Germany, Italy, Spain, and the United Kingdom), and the East as the 15 countries in East Asia and Oceania that are members of the Regional Comprehensive Economic Partnership, RCEP(Australia, Brunei, Cambodia, China, Indonesia, Japan, the Republic of Korea, Laos, Malaysia, Myanmar,New Zealand, Philippines, Singapore, Thailand, and Vietnam). This paper argues that currently available information points to the factors most responsible for the East–West divide. Warnings by early January 2020 about an atypical viral pneumonia in Wuhan, China, prompted rapid responses in many jurisdictions in East Asia. Publication of the virus’s genome on 10 January 2020 provided essential information for making diagnostic tests and launching vaccine development. China’s lockdown of Wuhan on 23 January 2020 provided a final, decisive signal of the danger of the new disease. By late March 2020,China had fully controlled its epidemic,and many other RCEP countries had taken early and decisive measures, including restrictions on travel, that aborted serious outcomes. Inaction during the critical month of February 2020 in the United States and most other Western countries allowed the disease to take hold and spread. In both the East and the West,stringent population-wide non-pharmaceutical interventions were widely implemented at great cost to societies,economies,and school systems.Without these measures, the outcomes could have been even worse. Most countries in the East also implemented tightly focused policies to isolate infectious individuals.Even today,most countries in the West allow infectious individuals to mingle with their families, coworkers, and communities. Much of the East–West divide plausibly results from failure in the West to implement the basic public health policies of early action and the isolation of infectious individuals. Widespread immunization in some RCEP and high-income countries will soon attenuate their outbreaks, while the slow rollout of vaccines in lower income countries is replacing the East–West divide in outcomes with a North–South one.The South is thus replacing the West as the breeding ground for more dangerous variants as exemplified by the highly contagious Delta variant, which may undermine hitherto successful control strategies in many countries.
1. Introduction
Policies for the control of coronavirus disease 2019 (COVID-19)fall into four categories. First, countries can seek to reduce transmission by non-pharmaceutical measures that separate all members of the population from each other. Mechanisms include physical distancing, stay-at-home orders, closures of schools and non-essential services,border controls,and mandatory face covering.Second,countries can seek to reduce transmission by separating infectious individuals from the rest. Since many potentially infectious individuals will develop symptoms only after they become infectious, an isolation strategy entails contact tracing and providing means and incentives for individuals to be isolated.If COVID-19 incidence is substantial, high-frequency mass testing may be needed. Third, countries can use mass immunization to provide individual protection and slow transmission, ideally to the point of herd immunity. And fourth, countries can seek to reduce harm by isolating highly vulnerable groups and providing treatment and supportive care for patients. Scientific advances underpin each approach. In practice, combinations of these four approaches are utilized.
To a reasonable first approximation, the countries of the East have chosen consistently different mixes of approaches than have the countries of the West, and they have achieved very different outcomes. By ‘‘countries of the East,” we refer to 15 countries in the Regional Comprehensive Economic Partnership (RCEP):Australia, Brunei, Cambodia, China, Indonesia, Japan, the Republic of Korea, Laos, Malaysia, Myanmar, New Zealand, Philippines,Singapore, Thailand, and Vietnam. The 14 RCEP countries other than China have a total population of 875 million.Including China’s 1.4 billion, RCEP accounted for nearly 30% of the world’s population in 2020 [1]. This paper examines China’s response separately from the 14 other RCEP countries (RCEP 14). By ‘‘countries of the West,” we refer to the United States and the five large and populous countries in Western Europe (Europe 5): France, Germany,Italy, Spain, and the United Kingdom. The population of Europe 5 is 323 million, roughly equal to the United States’ 331 million[1]. Countries in Africa, Latin America, the Middle East, and South Asia have had outcomes closer to those of the West than of the East. Clearly, countries within the ‘‘East” and ‘‘West” display marked heterogeneity, and generalizations are made with that caveat.
Cumulative COVID-19 deaths per million population in the countries of the West had often exceeded those of the East by factor of 100 by May 2021. Understanding the extent to which the East–West divide explains the divide in outcomes in terms of COVID-19 response is a question that is likely to engage scholars for years to come. Our purpose in this paper is to assess explanations that have been advanced so far. We begin by placing the COVID-19 pandemic into recent historical context.We then discuss the evolution of the pandemic in phases leading up to the emergence of the East–West divide.Next,we turn to the likelihood that inequitable access to vaccines will transform the current East–West divide into a North–South one with the risks inherent in continued viral evolution.
Our approach describes the pandemic in the following five phases:
· Phase 1: The COVID-19 epidemic in China (December 2019–March 2020);
· Phase 2: The world is warned (January 2020);
· Phase 3: Emergence of an East–West divide (February–July 2020);
· Phase 4: Second waves and beyond (August 2020 on);
· Phase 5:Vaccines and a North–South divide(December 2020 on).
Our intent in identifying five phases is not to suggest sharp boundaries, either between countries or between phases; rather,it is to provide broad organizing principles,albeit with exceptions,for thinking about where the world had arrived by May 2021 (the cut off date of our analysis).
2. The historical context
Over 3.5 million people around the world have died from COVID-19 by May 2021 [2]. How do these numbers compare with the other epidemics and pandemics in the previous hundred years that were similarly transmitted through the respiratory system?Table 1 [2–4] provides the numbers of deaths from four influenza epidemics and pandemics (H1N1 in 1918–1919, H2N2 in 1957–1958,H3N2 in 1968–1969,and H1N1 in 2009–2010),two previous coronavirus epidemics (severe acute respiratory syndrome (SARS)in 2003–2004 and the Middle East respiratory syndrome (MERS)in 2012+), and the current novel coronavirus pandemic (COVID-19 in 2019+) [4]. It should be noted that the flu virus mutation often starts in birds (hence the name ‘‘avian flu”), then jumps to pigs(‘‘swine flu”),and then to humans[5].The 1918–1919 flu pandemic was misnamed the‘‘Spanish flu”because it broke out during the final year of the First World War, when participating countries—but not neutral Spain—were censoring news about the flu[6].
The last column in Table 1 [2–4] allows direct comparisons of pandemic mortalities from these events by listing deaths per million population. It should be clearly stated at this point that much uncertainty accompanies the estimates of epidemic and pandemic mortality numbers.The Economist has presented analyses suggesting that COVID-19 deaths may be 2–4 times greater than the reported totals[7].The generally agreed-upon view that the numbers reported in standard sources are underestimates, particularly for India, parts of South America, and Sub-Saharan Africa.
Consider as a benchmark the approximately 450 reported deaths per million population globally from COVID-19 by mid-May 2021. The great flu pandemic of 1918–1919 was accelerated by wartime conditions and the troop movements of World War I.It eventually infected nearly one-third of the world’s 1.8 billion population and caused a staggering 27 000 deaths per million globally and 6600 per million in the United States. In comparison, the US COVID-19 cumulative deaths of 600 000 within 17 months from the time of the outbreak were approaching the total American deaths of 680 000 in the 1918–1919 pandemicac. Although SARS and MERS inflicted far fewer total deaths, their very high casefatality rates (13% and 35%, respectively, compared with about 2%for the recent flu pandemics and COVID-19)were major sources of fear and disruption.
This history of recurrent flu and coronavirus epidemics and pandemics, with their zoonotic origins, points to the plausibility that pandemics with the severity of COVID-19 could recur one or more times in the remaining decades of the 21st century. And the range of zoonotic threats goes beyond those with respiratory transmission: As of 2019, the human immunodeficiency virus(HIV)/acquired immune deficiency syndrome (AIDS) pandemic had killed almost 35 million people and, in the year of its peak mortality in 2004, deaths from HIV/AIDS totaled 1.7 million, or270 per million of the world’s population [8]. COVID-19’s enormous disruption of economies, societies, and education systems in much of the world underlines that 1918–1919 death levels are not required for a pandemic to have catastrophic impact. Drawing lessons from the East–West differences in response to COVID-19 is thus important,not only to help nations control COVID-19,but also to guide preparation for the future. Among other initiatives, the World Health Organization(WHO)convened a high-level independent panel—co-chaired by former Prime Minister Helen Clark and former President Ellen Johnson Sirleaf—to draw interim lessons from the world’s experiences with COVID-19. Its report was published in May 2021 [9]. The Lancet convened a commission for broadly similar purposes, chaired by economist Jeffrey Sachs; the Lancet Commission prepared an initial statement for the UN General Assembly’s meeting in October 2020 and an update in March 2021 [10,11].

Table 1 Mortality from selected epidemics and pandemics affecting the respiratory system, 1918–2019+.a
3. Phase 1: The COVID-19 epidemic in China (December 2019–March 2020)
China’s response to severe acute respiratory syndrome coronavirus 2(SARS-CoV-2),the virus causing COVID-19,has often been compared with its response to the SARS virus(SARS-CoV)in 2003–2004.Both were unknown viruses.While the country’s response to SARS was delayed,its response to SARS-CoV-2 has been faster and far more robust.
The first known hospitalized case of COVID-19 was reported in the city of Wuhan, in Hubei Province, on 8 December 2019 [12].Clinicians in Wuhan hospitals could not identify other diseases that displayed similar features on the lungs under computed tomography (CT) scans. On 27 December 2019, a hospital in Wuhan reported to the Wuhan Centers for Disease Prevention and Control (CDC) cases of pneumonia of unknown cause, leading to the latter’s investigation and subsequent classification of the disease as viral pneumonia[13]. On 30 December 2019,the Hubei CDC reported cases to the National CDC,and the Wuhan Municipal Health Commission (WMHC) issued an urgent notice to its hospitals [14]. On 31 December 2019, the WMHC released a briefing on its website about an outbreak of 27 cases of viral pneumonia,and advised the public to not go to enclosed public places and to wear masks. On the same day, the Chinese National Health Commission (NHC) sent an expert team from Beijing to Wuhan to investigate. Some early cases were associated with the Huanan Seafood Market, which sold mostly frozen seafood and wild and farmed live animals.On 1 January 2020,the Huanan Seafood Market was closed and the NHC convened a leading group to meet daily.
A WHO–China joint study in early 2021 found that the SARSCoV-2 virus had circulated widely in Wuhan (and Hubei Province)by mid-December 2019 before the major outbreak; however, the question of whether identifiable cases appeared earlier than December 2019 will await further scientific investigation [15].The possible presence of SARS-CoV-2 in France, Italy, and the United States (based on antibodies identified in blood and tissue samples) before the emergence of the disease in Wuhan, points to the difficulty of using surveillance systems to detect a new but initially silent virus [16–21]. For these reasons elucidating the origins of viral disease has frequently taken many years. To take two prominent examples, the genome of the virus causing SARS was only traced to a specific group of bats in Yunnan 14 years after the outbreak [22]. Similarly, the virus causing the HIV/AIDS epidemic was isolated in 1984. Yet, it was not until 15 years later that Gao et al. [23] and Hahn et al. [24] traced the origin to a specific group of chimpanzees and the associated transmission mechanism.
Understanding the origins of COVID-19 will provide knowledge relevant to the prevention of future pandemics. That said, the degree of political attention to the origins of COVID-19 (and the visibility that the WHO has conferred on that attention) well exceeds the question’s current relevance. In marked contrast,understanding where, when, and how new variants have evolved—in Brazil, India, South Africa, and the United Kingdom—can point to the importance of (and perhaps to mechanisms for)slowing or countering dangerous viral evolution.
This section now turns to examine the timeline of China’s response to the outbreak and the policies that then brought and kept the outbreak under control. The Lancet’s Editor-in-Chief Richard Horton and the WHO Independent Panel provide detailed but broadly similar timelines to the one provided here [25,26].
Scientific investigation played a key role in China’s response.In late December 2019, in order to understand the nature of this unknown virus,some Wuhan hospitals commissioned private biotech firms to undertake genetic analyses, while the Central Hospital of Wuhan collaborated with the Shanghai Public Health Clinical Center and Fudan University.The Wuhan CDC requested researchers to sequence the genome, while the National CDC undertook independent genetic analyses [27]. Genome sequencing of different virus samples by multiple research groups enabled the definitive identification of the novel coronavirus as the cause of the outbreak by 7 January 2020, and this news was released two days later. Genome availability facilitated the rapid development,approval, manufacturing, and distribution of diagnostics domestically.The first polymerase chain reaction(PCR)tests became available for use in Wuhan on 16 January 2020, thereby distinguishing the laboratory-confirmed cases from suspected cases identified by means of clinical features.
By mid-January 2020, the number of serious cases began to increase rapidly,including health care workers[28,29].Individuals infected with SARS-CoV-2 become infectious before they become sick and indeed frequently show only mild symptoms or none at all. Hence, by the time the hospitals started to become crowded,large numbers of infectious individuals must have been dispersed throughout Wuhan. These factors no doubt amplified the early spread of COVID-19.
Starting from 14 January 2020, the NHC organized the first national teleconference on the disease, issued the first guidelines on its diagnosis and prevention(with multiple revisions afterward,as new knowledge emerged), dispatched seven technical teams,and distributed testing reagents for diagnostics to the provinces.Dr. Nanshan Zhong, the respected expert who led China to eliminate SARS in 2004, was sent to Wuhan on 18 January 2020.
Although Wuhan reported only 198 confirmed cases and three deaths by 19 January 2020, cases had been reported in other provinces and neighboring Thailand,the Republic of Korea,and Japan.During the Chinese New Year holiday,an estimated 15 million trips in and out of Wuhan and three billion trips nationwide would take place[28].By 20 January 2020,the central government—recognizing the potential magnitude of the threat to the nation—took charge of the response. The turning point was marked by Dr.Zhong’s televised confirmation of the novel coronavirus’s humanto-human transmission and President Jinping Xi’s directive to make fighting the virus a top national priority. On 23 January 2020 (just two days before the Chinese New Year), Wuhan, a city of 11 million people, was locked down to stem transmission and to buy time for Hubei Province and other provinces to build a disease control and treatment infrastructure [30,31]. All forms of transportation in,out,and within the city were stopped;residents were ordered to stay home;and schools and non-essential services were closed.Vice Premier Chunlan Sun moved to Wuhan from late January to April 2020 to coordinate the fight against the virus.The People’s Liberation Army was mobilized to distribute supplies.Hubei,a province of 60 million people,was later placed under lockdown as well.
Hospital and caretaker capacity was ramped up through the construction of two field hospitals for severe and critical cases within about ten days. At the same time, 16 convention centers and sporting venues were converted to facilitate the isolation and treatment of mild cases. These health facilities, known as the Fangcang shelter hospitals, made it possible to isolate mild cases(and,later,pre-and asymptomatic cases)from the rest of the population [32,33]. Caretaker capacity grew rapidly with the deployment of some 42 000 medical personnel from 19 provinces,resulting in an average ratio of 1 medical staff to 1.2 patients at the height of the response. All COVID-19 related medical and health services were provided free of charge.
The outcomes quickly reflected the impact of this intensive control.Enhanced medical capacity and the effective triage function of the Fangcang shelter hospitals sharply reduced the case-fatality rates. Travel and social restrictions and, in particular, the isolation of identified infections and the quarantine of close contacts quickly pushed transmission to well below levels that could sustain the outbreak. According to the WHO, new cases (based on the date of onset) peaked and plateaued between 23 and 27 January 2020[12].Cases then declined steadily to the single digits by late March 2020. Deaths peaked and began to decline about ten days later[34]. Other provinces adopted varying degrees of restrictions and treatment,and their case-fatality rates ranged from zero in Jiangsu Province to 2.7% in Heilongjiang Province—much lower than the 4.6% case-fatality rate in Hubei Province by mid-March 2020[35]. About 83% of China’s cumulative cases and 98% of deaths were contained in Hubei Province. China eliminated the domestic transmission of SARS-CoV-2 by 8 April 2020 and, then, Wuhan lifted its lockdown.The remaining tasks were to contain imported cases, identify asymptomatic cases, conduct mass testing whenever sporadic community transmissions arose, and conduct mass vaccination.
4. Phase 2: The world is warned (January 2020)
Multiple disease outbreaks occur every year, and the WHO reports and tracks them in its‘‘Disease Outbreak News.”The WHO listed about 120 outbreaks globally in 2019, including outbreaks of MERS, Ebola, yellow fever, cholera, and measles, to name just a few [36]. Each of these outbreaks merits some local or regional response,but few merit or receive a global response.Although the appropriate magnitude of response may be clear to the WHO and to others in retrospect, much uncertainty typically surrounds the decisions that are made early in an outbreak.SARS-CoV-2 is contagious in pre-symptomatic and mildly symptomatic cases which,as noted previously, made it harder to detect before mounting numbers of seriously ill patients called attention to the outbreak.
How did China share the rapidly evolving information with the world? The WMHC’s notice about viral pneumonia on 30 December 2019 and its warning to the public on its website a day later were picked up by domestic journalists, neighboring health authorities, and the WHO’s Beijing Office and its headquarters in Geneva (the last through ProMed’s machine translation). This led to an inquiry from the WHO’s Beijing Office to the Chinese authorities on 31 December 2019 [37]. The WHO shared information about the clusters of cases through its information system and advised member countries to take precaution against acute respiratory infections on 5 January 2020. China maintained regular communications with the WHO in the new year and provided updates as new knowledge accumulated. On 20–21 January 2020,a team from the WHO’s Beijing Office visited Wuhan to learn about its disease control and treatment protocols [38].
Having picked up public warnings from Wuhan on 31 December 2019, Hong Kong’s health authorities immediately stepped up border screening and put hospitals on alert [39], while the Taiwan CDC undertook similar actions starting on 2 January 2020[40]. Thailand’s Ministry of Health set up an Emergency Operating Center on 4 January 2020 [41]. By 20 January 2020, Japan,Malaysia, Singapore, and the Philippines had implemented border control measures [26].
The National CDC informed Taiwan about the identification of the novel coronavirus on 9 January 2020. Wuhan then hosted fact-finding visits by experts and officials from Hong Kong,Macao,and Taiwan on 13–14 January 2020.The Taiwan CDC posted warnings about the new virus on its website on 15 January 2020[42,43].Starting on 21 January 2020,the NHC’s‘‘Daily Briefing”on its website began reporting statistics on cases and deaths in Chinese mainland,and eventually extended coverage to Hong Kong,Macao,and Taiwan [44].
Official contact between the Chinese government and the United States was frequent in the early days of the COVID-19 pandemic. On 4 January 2020, the director of the China CDC,Dr. George Gao, spoke to his counterpart, Dr. Robert Redfield, the director of the US CDC at that time.In a follow-up call on 8 January 2020,Dr.Gao conveyed his growing worry about the virus’s transmissibility between people [45]. Dr. Gao is a member of the US National Academy of Sciences and is respected in the US scientific community. His concerns would have been taken seriously.Chinese President Jinping Xi spoke with German Chancellor Angela Merkel and French President Emmanuel Macron about the disease on 22 January 2020,and with the US President Donald Trump on 7 February 2020 [14].
On the scientific side,the virus’s genome was transmitted to the WHO on 11 January 2020.The lead scientist from Fudan University posted the genome on the US National Institute of Health (NIH)’s GenBank[46]for peer review and had it released on the Virological online discussion forum[47].The availability of the genome in the relatively early stage of the pandemic enabled scientists in Germany and the Republic of Korea to develop diagnostic tests quickly[48,49].The Republic of Korea was able to use free mass testing to control the disease [50], and Germany made its test available to other countries through the WHO.
Chinese clinicians and scientists had submitted papers on the epidemiology, clinical features, and management of COVID-19 to The Lancet [28,51] and to the New England Journal of Medicine[52]. The peer review, revision, and editorial process for these initial papers among a series was completed in time for publications on 24 January and 29 January 2020, respectively, suggesting that the editors of these journals understood the gravity and urgency of the situation.In one of the 24 January 2020 papers in The Lancet,Wang et al. [28] warned explicitly, ‘‘As an RNA virus, 2019-nCov still has the inherent feature of a high mutation rate...(and) the possibility to become more efficiently transmitted from person to person and possibly become more virulent....We need to be wary of the current outbreak turning into a sustained epidemic or even a pandemic.”
Dr.Ugur Sahin and Dr.Ozlem Tureci,the lead scientists and cofounders of the German company BioNTech, pivoted immediately to COVID vaccine development after reading the 24 January 2020 The Lancet paper on COVID, which resulted in the first vaccine becoming available in ten months [53]. Virologist Dr. Robert Gallo[54] has pointed to the benefits from the deep and longstanding ties between Chinese,European,and US scientists.A salient example is the Global Virus Network(GVN).Gallo and many others have urged continued close collaboration on COVID-19 in order to take advantage of medical and scientific ties.Unfortunately,as The Lancet editor Richard Horton put it, ‘‘Too few people paid attention to China’s well-documented clinical experience” [55].
In summary, regular contact with the WHO, early phone conversations with Western health officials and political leaders, and the hosting of delegations from Hong Kong, Macao, and Taiwan informed the world of the serious and growing concerns of Chinese scientists and health officials. China’s lockdown of Wuhan on 23 January 2020 was on such an unprecedented scale that no country could continue to ignore the potential danger of COVID-19. Yet most of the West barely reacted to the January warnings.The final report of the Independent Panel drew the following blunt conclusion: ‘‘It is glaringly obvious to the Panel that February 2020 was a lost month...” [9]. By mid-March 2020, it became clear that the Western failure to take advantage of the warnings from Asia had led to a bifurcation of the outcomes experienced by the West and those experienced by the East.
5. Phase 3: Emergence of an East–West divide (February–July 2020)
The courses taken by the pandemic in the first half of 2020 diverged sharply between China and RCEP 14 (the East) and the United States and Europe 5(the West).Figs.1 and 2[2]summarize the differing experiences. Although it is difficult to overstate the magnitude of the difference between East and West, exceptions exist. Norway and Finland, for example, had 143 and 168 deaths per million population, respectively, as of mid-May 2021 while the RCEP members Indonesia and the Philippines each had 178[2].
We make no claim that this ‘‘East–West” characterization is a complete one,only that it provides a useful framework.Responses in the Western Hemisphere countries of Latin America align closely with those of Europe 5, as do the responses of most Eastern European countries.Countries in Africa,the Middle East,and South Asia contain substantial diversity. Few, however, have had outcomes that would fit well in the ‘‘East” category.
One critical difference between East and West was in the quickness and magnitude of the response. Yet there have been both domestic and international criticisms of China’s health system for having had a slow initial response. This raises the question: slow relative to what?
Table 2 [2] shows that China and many RCEP countries acted sufficiently swiftly, relative to any of the countries of the West,to have brought the daily new cases(based on a seven-day moving average) under control within just a few months. The columns in bold in Table 2 [2] thus answer the question of ‘‘speed relative to what?”by comparing how promptly countries introduced effective responses from looking at their impact on cases. Taking Wuhan’s lockdown on 23 January 2020 as the sounding of the global alarm,all countries outside China had time for preparation from at least that date. By 1 April 2020, ten weeks after Wuhan locked down,new cases in Europe 5 rose to several thousands per day (on a seven-day moving average) and those in the United States surged to about 23 000,while most of the RCEP had only several hundred new cases per day at the maximum (and zero cases in Vietnam,Laos, Cambodia, and Brunei) (Table 2 [2]).
Despite its lower income and high level of cross-border trade and movement of people with China, Vietnam provides a good example of a rapid response. This country began its preparation long before its first case appeared on 23 January 2020. Vietnam’s health officials organized a teleconference with the WHO and 700 hospitals nationwide on prevention and launched a website to disseminate public information on 7 February 2020. It also developed its own test kits[56].Vietnam also effectively used border control, contact tracing, the isolation of infectious individuals and targeted community quarantine. The country imposed national isolation for its 96 million people for 15 days in April 2020 to eliminate the disease, resulting in 99 days free of new cases [57]. Its first death only occurred on 31 July 2020.
Australia, and New Zealand also performed very well, showing that different political systems can fight the pandemic effectively.
Attempting to explain the East–West divergence will provide a research agenda for many years to come. That said, three reasonably consistent differences in approach—beyond the timeliness of response—characterize the two groups.
·Public health systems in China and in many of the other RCEP countries had been primed by the experiences of SARS,MERS,and avian and swine flus to invest heavily in public health response capacity and, perhaps more importantly, in readiness to use that capacity [58,59]. For the most part, the RCEP countries immediately placed COVID-19 at their highest level of public health risk and introduced restrictions on travel.Although some European delegations to the European Commission(EC)had argued that SARS-CoV-2 should be classified as a group 4 (high risk) agent, the EC continued to label it a group 3 agent as late as June 2020. This rating slowed the national public health and clinical responses [60].· In many RCEP countries, people’s high level of compliance to social and physical restrictions and masking orders stems from cultural values that emphasize the common good. The converse was initially true in the West, partly due to liberal concerns about human rights and privacy and a conservative focus on individual prerogatives. Even compliance to mask wearing became a political issue in some Western countries,and contacts were difficult to trace due to concerns about privacy. Population-wide separation of individuals—the first of the four policy directions listed at the beginning of this paper—thus played a critical role in the countries of the East.Ultimately,most Western populations realized the need for major behavioral changes. After major changes in behavior had already begun,Western governments eventually adopted stay-at-home orders, the closing of schools and enterprises,and mandatory social distancing and mask wearing [61]. As the pandemic has been prolonged, the economic cost of these measures continues to rise, and people’s fatigue with restrictions has led to periodic protests and even violence.
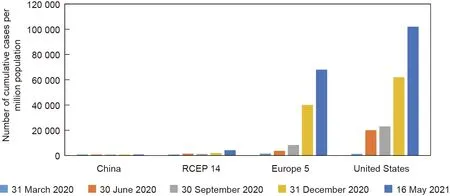
Fig.1. Cumulative cases per million population in China,the RCEP 14(comprising 14 Eastern countries in the RCEP minus China),Europe 5(comprising five large countries in Europe),and the United States.Because China’s cumulative cases ranged from 58 to 63 per million population during this period,its bars do not show up in the graph.Source:Worldometers.info [2].

Fig. 2. Cumulative deaths per million population in China, the RCEP 14, Europe 5, and the United States. Because China’s cumulative deaths are about three per million population, its bars do not show up in the graph. Source: Worldometers.info [2].

Table 2 Seven-day moving average of daily new cases in China, the United States, European 5, and RCEP 14.
· Countries in the East complemented population-wide control measures with the second policy approach listed at the beginning of the paper:measures focused on identifying and isolating COVID-positive individuals. Effective programs provided infectious individuals both the means and incentives to isolate[62], including institutional isolation when home circumstances were insufficient. Efficient diagnostic tests underpin effective policies for contact tracing and isolation of infected individuals. Most countries of the East moved rapidly to acquire this capacity, while the United States and many (but not all) Western countries lagged behind. When numbers become large, both timely isolation and the end of isolation are likely to require high-frequency use of lateral-flow antigen testing (LFT). Mina et al. [63] and Peto [64] summarized the technical arguments underlying the use of LFT in this public health context,while Chen et al.[33]presented an epidemiological model showing the potential impact.
At the time of writing,it appears unlikely that more than a few countries of the West will adopt serious isolation measures(beyond those for hospitalized patients). In London, for example,large numbers of infectious people remain in the community with minimal efforts to isolate them [65]. Instead, the countries of the West appear likely to continue to rely on unpopular and poorly targeted population-wide measures while expecting widespread immunization to eventually control their outbreaks. The United States provides an example of this approach. In April 2021, harsh measures remained in place in many US states, although an effective vaccination program was well underway.
The East–West distinctions drawn above simplify what are, in fact, rich diversities in policy within and across all countries. Yet this simplification makes it possible to highlight the extremely different approaches that have been taken,and points to explanations for differences in performance.
6. Phase 4: Second waves and beyond (August 2020 on)
By the summer of 2020, most European countries had brought the number of daily new cases down to very low levels. A first wave could reasonably be considered over.While the United States never completed a first wave, new infections remained at an approximately stable—although still high—level from early July through early October 2020. In mid-October 2020, the number of new cases per day in the United States began to grow rapidly and,at about the same time,second waves began in most European countries.Many RCEP 14 countries also began modest but real second waves,while China continued to contain incidence at very low levels. Table 2 [2] documents these trends, among which the second waves are generally much bigger than the first waves. However, the increase in deaths in the second wave tends to be far less pronounced than the increase in cases,probably due to greatly improved supportive care.
Why were the second waves so much larger in Europe 5, relative to the RCEP 14? And why was there an even larger difference between the United States and China? Again, answers to these questions will likely be debated for a long time and may never be fully elucidated.That said,the following are three plausibly significant explanations for differences in the second wave between Europe 5 and the RCEP 14.
·Countries in the East had largely sought the complete elimination of domestically transmitted SARS-CoV-2, whereas those in the West generally only sought to bring the pandemic under control at a level at which the hospitals could cope.For a period of time, infections in Sweden and the United Kingdom were even allowed to spread toward the (hoped for) level that would confer herd immunity.
·As was the case with the first waves,the countries of the East responded rapidly to indications of a nascent second wave,whereas Western countries were often slow to recognize or respond to a re-emerging outbreak.
· In retrospect, it seems likely that the Europeans simply relaxed their control measures prematurely, as restriction fatigue set in among the people and the pressure to restart the economy rose,whereas earlier restrictions in many RCEP 14 countries had driven down the reproductive rate of the virus to such a low level that the countries could use a more targeted approach to maintain vigilance afterward.Nevertheless, by early May 2021, outbreaks in a number of RCEP 14 countries that had been highly successful in their early pandemic control were leading to renewed and strong efforts at control on the part of governments.
The United States–China differences remain far more pronounced than the Europe 5–RCEP 14 differences.The above points concerning Europe 5 and RCEP 14 are likely to help explain the differences between the United States and China as well. An additional and important factor lies in the quality of leadership.China’s leaders took early, strong, and consistent action, whereas former US President Donald Trump deliberately underplayed the severity of the pandemic in the United States[66–68].Trump publicly and frequently advocated hydroxychloroquine as a treatment,even after trials had showed it to be ineffective.He sidelined technical experts in the CDC and NIH,withdrew the United States from the WHO,and accused hospitals of over-reporting deaths to make a profit. He frequently hosted superspreading re-election rallies,mocked the wearing of face masks, and encouraged armed antimask rioters at the Michigan State Capitol. His administration offered no national plan,as Trump considered it the responsibility of the states, not the federal government, to fight against COVID-19. Trump attempted to transfer blame for the US outcomes to China and to the US states led by politicians in the Democratic Party. Among other adverse consequences, blaming China has stimulated rapidly rising anti-Asian and anti-Chinese prejudices and violence in the United States.After a gunman killed eight people, including six women of Asian descent, in Atlanta, USA, in March 2021, a poll linked to Telegram (a website favored by the political Right) found that 84% of respondents answered that the violence was ‘‘justified retaliation for COVID” [69].
No explanation for the performance of the United States can be complete without paying explicit attention to this leadership failure, which was amplified by scores of millions in the population who were unconditionally willing to take Trump both seriously and literally. The Scottish historian Niall Ferguson [70] cautions,however, against exaggerating the impact of what he also views as very real leadership failures. He points to institutional inadequacy and long-term funding shortfalls as additional and significant factors that inhibited the delivery of public health basics.
There is a common feature in the second-wave resurgence of the virus in both the East and the West: Neglecting to protect disadvantaged groups left such groups vulnerable and caused them to become sources of infection. An outbreak among seasonal agricultural workers in Spain in the summer of 2020 led to the virus’s further spread to the general population in Spain and elsewhere in Europe, contributing to the second wave [71]. Singapore, which had done a remarkable job in keeping the virus at bay in the early months, overlooked the crammed living conditions of migrant workers from South Asia, resulting in almost half of the 300 000 migrant workers being infected by the end of 2020 [72]. Thailand,which had also very effectively controlled COVID-19, saw an outbreak among migrant workers from Myanmar at the beginning of 2021,followed by a spread into a slum area in April 2021 and then into the prisons,which accounted for more than 70%of a new daily spike of nearly 10 000 cases [73].
In Florida,USA,the infection of migrant agricultural workers led to rising case numbers[74].In California,the infection of prisoners,some of whom had been relied upon to fight wildfires, led to a shortage of fire fighters during the fire season in late 2020 [75].In the United States as a whole,COVID-19 death rates among Hispanics and Native Americans were 2.3–2.4 times higher than those among non-Hispanic-whites.The corresponding figure for African-Americans was nearly two times greater than that for non-Hispanic whites [76]. COVID-19 exposes deep inequities in societies [77]. The remaining pools of infection—in both East and West—amplify the inequalities in other dimensions, but also remain continuous sources for viral resurgence throughout society.
Second waves have moved on to third and fourth waves in some countries,including among the RCEP 14.Differential access to vaccines across countries points to the likelihood that the East–West divide of 2020 will become a North–South divide in 2021 and beyond.
7. Phase 5: Vaccines and a North–South divide(December 2020 on)
Vaccine development has been proceeding at record speed.Whereas normally it takes years to develop a vaccine, vaccines against COVID-19 were ready for approval for emergency use within less than a year of the outbreak [78]. Major progress has been made on four distinct types of vaccines:inactivated or attenuated whole virus, protein subunit, viral vector, and nucleic acid(ribonucleic acid (RNA) and deoxyribonucleic acid (DNA)) [79].All four aim to stimulate an immune response to an antigen (a molecule typically characterized by the spike protein on the coronavirus that invades human cells).By May 2021,over 100 vaccines are under various phases of development,of which 11 were authorized for emergency use by national governments [80].
In anticipation of the need in the developing world, the WHO formed a partnership known as COVID-19 Vaccines Global Access(COVAX). The Vaccine Alliance (GAVI) and the Coalition for Epidemic Preparedness Innovation (CEPI) joined the effort to secure COVID vaccines through COVAX for 92 countries that have a gross national income per capita under 4000 USD[81].The priority is to vaccinate health care workers and vulnerable groups,with the target of covering 20%of the population.The WHO undertook technical review of vaccines’ efficacy and safety, and production standards. COVAX can procure the WHO-approved vaccines and United Nations International Childrens’ Emergency Fund (UNICEF)will distribute it. Sinopharm and Sinovac are the first two non-Western vaccines approved by the WHO,along with BioNtech/Pfizer, Moderna, Oxford/AstraZeneca which is also produced in India and the Republic of Korea, and Johnson and Johnson [82]. Some vaccines are remarkably effective, and some are well-suited to meet the logistical challenges of delivery in remote and difficult environments [83].
Interestingly, there has been little effort to explore the known potential for existing live attenuated vaccines(LAVs)to act against diseases other than the one they target. Chumakov et al. [84]reviewed the evidence for this potential and pointed to the low cost and speed with which trials to test the impact of selected existing vaccines against COVID-19 could be done.
Early in the pandemic, the now Director-General of the World Trade Organization (WTO), Ngozi Okonjo-Iweala warned against the potential for high-income countries to place large,early orders that would impede vaccine access for others[85].Vaccine delivery to low-income countries only began on 24 February 2021, two months after vaccinations had begun in the West [82]. The fastest progress in vaccination has been made in the global North.By mid-May 2021, the United Kingdom, the United States and the European Union had administered about 85, 82, and 60 doses, respectively, for every 100 persons [86]. The availability of effective vaccines is clearly changing the trajectory of the pandemic in the global North,as is evident from the rapid decline of daily new cases(Table 2 [2], the column for May 2021). However, there remains a substantial number of people in the West who are resistant to vaccination and become reservoirs of infection and mutation.
The countries of the East, in large part due to their success in pandemic control, are being slower to secure vaccines which are still in short supply [87]. By mid-May 2021, the number of doses administered per 100 people averaged 16 in Asia, to 22 in South America, and 1.8 in Africa [86]. China as a vaccine developer and manufacturer, administered about 29% per 100 people as it supplied nearly half of its vaccines to other countries.
The populations in the wealthiest countries are being vaccinated about 30 times faster than those in the poorest countries[88]. By May 2021, UNICEF had distributed vaccines to nearly 130 countries,but the shipment accounted for only 4%of the delivery target of 2 billion doses for 2021[82].Moreover,shipments do not automatically translate into vaccinations, as there have been inevitable organizational, logistical, and financial challenges [83].Various types of vaccines with different requirements for cold chain storage complicated the logistics. Rumors about harmful effects of vaccines and delays in transport within countries and in training of vaccination staff at times led to expiration and destruction of delivered vaccines.
There are at least three barriers to achieving global vaccination coverage.The first is finance.Vaccines cost between 3–37 USD per dose [81]. Exceptionally among Western manufacturers, Oxford/AstraZeneca has priced its vaccine at cost and has facilitated a licensing arrangement that will lead to increased supplies of vaccines at cost [89]. Still, meeting the target dosage will require resources beyond the currently available funds, even including(relatively modest) commitments from the Group of 7 of highincome countries.
In addition, COVAX recipient countries must bear the cost of hiring additional vaccination workers, providing in-country transport, and covering the remaining 80% of the population. About 80 other developing countries are ineligible for COVAX financing due to their higher per capita income, and must self-finance their vaccine purchases. Financial constraints on vaccine availability could hold back both pandemic control and development for many countries for years to come.
To address the financial shortfall, the International Monetary Fund (IMF) has made a three-point proposal to vaccinate 40% of the world’s population by the end of 2021 and 60% by mid-2022[90]. The IMF’s estimated cost is 5 × 1010USD, but its estimates of narrowly economic benefits far exceed these costs. Focusing only on public-sector budgets in high-income countries, the increase in tax revenue from widespread vaccination could be as much as 1×1012USD.The IMF estimates that the currently unmet need is 1.3 × 1010USD out of the estimated 5 × 1010USD total.However, the remaining need for 1.3 × 1010USD is now, not in the form of commitment to future finance. These resources are needed for vaccines and to insure against downside risks by increasing production capacity [91].
The second barrier to vaccine availability results from intellectual property (IP) rights being held by private manufacturers of vaccines, with attendant non-transparent contracts and pricing.The lack of technical infrastructure in many countries implies that‘‘know-how”transfer will also be needed in many cases in order to shore up local capacity; indeed, the pharmaceutical industry suggests that the current lack of know-how implies that lessening IP restrictions might have little effect.Ord[92]has,however,pointed to the extreme rapidity with which biological science and knowhow can spread, and many of the patented vaccines use familiar technology.
India and South Africa have taken the lead in approaching the WTO to use emergency waiver options to relax the IP protection for COVID-19 vaccines [93]. The European Union and the United States initially objected to a waiver on the (generally reasonable)grounds that the monopolies provided by patents stimulate innovation. (The United States now favors the proposed waiver, as do France and China.) What is clear is that patents failed to provide sufficient incentives for the private sector to develop COVID-19 vaccines. Major government subsidies and government advance market commitments have provided incentives where patents have failed to do so. The protection of patent profitability for corporate shareholders under these circumstances could plausibly lead to widespread feelings of injustice—both on the part of the taxpayers who covered the costs and risks associated with development and on the part of citizens around the world whose lives continue to be at risk as immunization is postponed.
Despite the central role that government investments and purchase commitments have played in COVID vaccine development, the industry has argued that relaxing patent protection on IP that was paid for in substantial part by the public sector could lead to competition for scarce vaccine ingredients and set a precedent that would be harmful to industry profitability[94]. They further argue that messenger ribonucleic acid (mRNA)technology has potential applications beyond making COVID-19 vaccines, and waiving IP rights could accelerate the development of innovative medical products in China and Russia [95]. While the pharmaceutical industry may well be correct about potential reductions in their profits, it is difficult to be convinced, for example, that the faster development of drugs that could potentially benefit people everywhere would be a negative consequence.
The critical need for vaccines has provided impetus to a number of countries to develop their own manufacturing capacity.Argentina,India,Mexico,the Republic of Korea,and Thailand have negotiated licensing agreements to produce Western-patented vaccines. Bangladesh, Brazil, Egypt, Indonesia, Pakistan, Serbia,and the United Arab Emirates,some of which hosted phase 3 trials of Chinese vaccines,are negotiating or have reached an agreement to produce or package Chinese vaccines. Serbia and Bangladesh have also negotiated with Russia to produce its vaccine [96–104].
These licensing arrangements can be expected to increase manufacturing capacity and vaccine availability.At the same time,they leave in place the IP deterrents to many potential producers around the world. Innovation and investment would be discouraged by the threat of legal action from the holders of current IP or by political action from their governments. COVID-19 may well remain a threat for many years, during which time constructive innovation and investment could occur around the world if the threat of IP action were relaxed.
The third barrier to vaccine availability lies in export restrictions on vaccines or on critical ingredients to make them.Examples come from the European Union and from the denial by the United States of access for India to vaccines and vaccine constituents(until a policy reversal in late April 2021) [105]. India is a very big licensed producer and exporter of COVAX-approved vaccines. As the result of the recent surge in domestic infection and demand for vaccines, India, too, has suspended vaccine exports, further adversely affecting vaccination in the global South [106]. Jha et al. [107] point to directions for addressing vaccine nationalism in the long term.
Granted many caveats,it was at least plausible that 2021 would witness, for all practical purposes, the end of the COVID-19 pandemic in the global North. For the three reasons discussed above,adequate vaccine coverage is likely to arrive much later in many parts of the South, with continued loss of life and income. A high volume of new cases in the South would entail not only losses for the South, but risks for all. One risk is that of providing a continued source for the spillover of SARS-CoV-2 into countries everywhere.A second risk is that viral evolution may continue to create SARS-CoV-2 variants that are more transmissible, more deadly, or both.
Two threats—spillover and evolution—are threats to other countries, not just to countries with active cases. As economists put it,these threats constitute major,negative,cross-border externalities.At any given time,the global risk potentially posed by a country is likely to be roughly proportional to the number of new cases there.Thus,continuation of the pandemic in the South will pose an ongoing threat to the North—just as huge case numbers in the Western hemisphere and in Europe have had major negative consequences far outside their borders. One significant example was the emergence of the virus lineage B.1.1.7(Alpha)in late 2020 as a‘‘variant of concern,” a variant estimated to have a reproduction number 43%–90% higher than the initial variant of SARS-CoV-2 [108,109].By March 2021, the Alpha variant had spread from its origin—believed to be in England—to 114 other countries, including India,as previously noted.
Due in part to the rapid pace of vaccination, daily new cases in the United States declined from 34% of those of the world in early January 2021 to under 5% by May 2021, whereas those in India grew to account for about 45% of new cases worldwide (Fig. 3[2]).The rapid increase of cases in India exemplifies the risk posed to other countries by high domestic case numbers. The exceptionally transmissible B.1.617 variant (which mutated from Alpha and is known as Delta) had spread from India to over 30 countries by early May [109]. As Yamey [110] has pointed out, global justice and solidarity provide more than sufficient reasons for the North to help ensure vaccination success in the South. Self-interest amplifies these arguments.
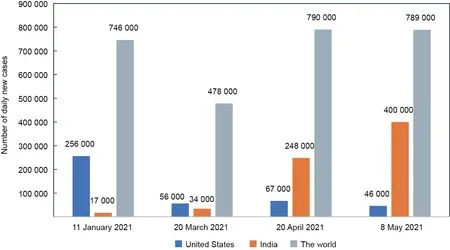
Fig.3. Sources of risks for viral spillover and evolution:daily new cases(seven-day average)in India,the United States,and the world.Daily new cases in the world includes those in India and the United States. Source: Worldometers.info [2].
8. Conclusions
The ‘‘East–West” characterization used in this paper inevitably simplified diversity within each group and only imperfectly characterized the full range of countries. That said, the East–West divide in terms of responses to COVID-19, and the outcomes from such responses, constitutes what is perhaps the most salient feature of the COVID-19 pandemic.Quick action and the effective isolation of infectious individuals characterized the responses in much of the East. Failure to adopt these basic public health measures in all likelihood contributed substantially to the far higher mortality levels in the West—mortality levels that were suffered despite harsh lockdowns in many countries. Early vaccination may provide the tool that Europe and the United States can use to partially close their gaps with the East in terms of new cases and deaths. At the same time, inequities in vaccine access are creating a North–South divide that replaces the East–West one, even though the IMF has estimated that the cost of rapid movement toward global vaccine coverage would be modest. The enormous global setbacks potentially resulting from the Delta variant underscore the magnitude of the risks from spillovers and viral evolution will persist as long as the North–South divide continues.
Acknowledgements
The authors acknowledge helpful comments by Simiao Chen,Lawrence Lau, Anthony Measham, Richard Skolnik, and Nathan Wolfe. Robert Gallo provided particularly detailed and helpful comments.The views expressed are,however,those of the authors.The contribution of Dean T.Jamison was supported through grants from the Trond Mohn Foundation, Norway(BF2019MT02)and the Norwegian Agency for Development Cooperation(Norad), Norway(RAF-18/0009)to the Bergen Centre for Ethics and Priority Setting.
Compliance with ethics guidelines
Dean T.Jamison and Kin Bing Wu declare that they have no conflict of interest or financial conflicts to disclose.
杂志排行

Engineering的其它文章
- Facilities for Centralized Isolation and Quarantine for the Observation and Treatment of Patients with COVID-19
- Quantitative Investigation of Tomographic Effects in Abnormal Regions of Complex Structures
- Fast Marching Method for Microseismic Source Location in Cavern-Containing Rockmass: Performance Analysis and Engineering Application
- Non-Communicable Diseases During the COVID-19 Pandemic and Beyond
- Next Steps for Efficacy Evaluation in Clinical Trials of COVID-19 Vaccines
- Temporal Profiles of Antibody Responses, Cytokines, and Survival of COVID-19 Patients: A Retrospective Cohort