Clinical efficacy of sticking-needle acupuncture plus tendon-regulating manipulation in the treatment of acute ankle sprain
2021-12-17ZhaoYan赵岩ZhaoYunzhen赵云珍YuShengdong余晟东
Zhao Yan (赵岩), Zhao Yun-zhen (赵云珍), Yu Sheng-dong (余晟东)
1 Jinhua Hospital of Traditional Chinese Medicine, Zhejiang Province, Jinhua 321017, China
2 Panhuo Community Health Service Centre in Yinzhou District of Ningbo City, Zhejiang Province, Ningbo 315000, China
Abstract
Keywords: Acupuncture Therapy; Sticking Needle; Tuina; Massage; Pain Measurement; Visual Analog Scale; Sprains and Strains; Ankle Injuries
Ankle sprain is one of the common injuries in daily life and sports[1-2]. However, in most cases, ankle sprain is not combined with rupture of tendons or fracture.Standardized treatment is often neglected by patients,leading to synovitis, tendinopathy, joint stiffness, loss of muscle strength, joint instability or persistent pain and swelling in some patients, which increases the incidence of traumatic arthritis[3-4]. Therefore, it is important to provide patients with an effective treatment modality that relieves pain and swelling more quickly and facilitates the recovery of ankle function, thereby reducing the occurrence of sequelae. Sticking-needle acupuncture has significant clinical efficacy in the treatment of painful soft tissue disorders, such as humeral epicondylitis, frozen shoulder, and myofascitis[5-6], but its reports in ankle sprain are limited.Since tendon-regulating manipulation has definite efficacy in the treatment of ankle sprain, we used sticking-needle acupuncture plus tendon-regulating manipulation to treat acute ankle sprain, expecting that it would have better clinical efficacy. It is reported as follows.
1 Clinical Materials
1.1 Sample size calculation
Based on previous literature, the sample size was estimated using the differences between groups in visual analog scale (VAS) for pain due to acute ankle sprain after treatment[7]. The estimated VAS difference was taken as 1 with a standard deviation of 0.8. Type Ⅰ error and statistic power were set at 0.05 and 80%, respectively.The superiority bound was considered as 0.5. Thirtythree cases per group were then calculated using PASS software. Considering a dropout rate of about 17%, we planned to recruit 80 patients into this study.
1.2 Diagnostic criteria
Grades Ⅰ and Ⅱ ankle sprain: Clear history of ankle injury, no ankle fracture or ligament rupture found on imaging, and meeting the diagnostic criteria for gradesⅠ and Ⅱ injury developed by Kaikkonen A,et al[8].
1.3 Inclusion criteria
Met diagnostic criteria for grades Ⅰ and Ⅱ ankle sprain; aged between 20 and 40 years; within 24 h after injury; signed informed consent.
1.4 Exclusion criteria
Combined fracture or presence of definite ligament rupture; presence of peri-ankle skin disease or damaged skin; presence of psychiatric disorders; with limb mobility impairment of the affected side before ankle sprain.
1.5 Criteria for elimination and dropout
Those who were unable to cooperate with the treatment; chose to drop out due to fainting during the treatment.
1.6 Statistical analysis
SPSS version 19.0 statistical software was used for statistical analysis. The measurement data were expressed as mean ± standard deviation (±sif they conformed to a normal distribution. Thet-test was used for comparisons between groups, and the repeated measures analysis of variance (ANOVA) was used for the repeated measures data. If they did not conform to normal distribution, median (lower quartile, upper quartile) [M (QL, QU)] were used; non-parametric ranksum test was used for comparisons between groups, and repeated measures ANOVA was used for repeated measures data after transformation of variables.Qualitative data were expressed as frequencies (n) and percentages (%), and the Chi-square test was used for comparisons between groups.P<0.05 was taken as statistically significant.
1.7 General data
A total of 80 patients with acute ankle sprain were recruited from Jinhua Hospital of Traditional Chinese Medicine, Zhejiang Province between May 2019 and May 2020, and divided into two groups according to the random number table method. Unduplicated numbers between 1 and 60 were generated using Microsoft Excel,and patients were included starting with the first number in the random number table, with odd numbers in the control group and even numbers in the treatment group.One case in the control group and two cases in the treatment group withdrew due to poor cooperation with the treatment, and another case in the treatment group withdrew due to fainting during the treatment. There were no statistically significant differences between the two groups in baseline characteristics (P>0.05),indicating that the two groups were appropriately comparable (Table 1).
2 Treatment Methods
2.1 Control group
Early management was based on the “RICE” principle:rest, ice application, compression bandage and elevation of the affected limb within 24 h. After 24 h, tendonregulating manipulation was applied as follows.

Table 1. Baseline characteristics between the two groups
The patient took a supine position. The doctor held the affected heel in one hand to fix the ankle joint, and the other hand Tui-Pushed and Rou-Kneaded the tendons with the thumb radiating out from the swollen center for about 10 min.
The doctor held the patient's affected heel in one hand and the front part of the foot in the other, and performed pulling and stretching traction as well as small foot loops, dorsiflexion, plantarflexion, inversion, and eversion manipulations for about 10 min.
The doctor An-Pressed and Rou-Kneaded the tendons around the ankle joint starting from the lower middle of the calf for about 10 min.
The above manipulations were performed once every 2 d for a total of 2 weeks.
2.2 Treatment group
On the basis of intervention in the control group, the treatment group received additional sticking-needle acupuncture.
Acupoints: Taixi (KI 3), Kunlun (BL 60) and Jiexi (ST 41)on the affected side.
Methods:Filiform acupuncture needles (0.30 mm in diameter and 40 mm in length) were used to puncture the above acupoints perpendicularly. After needling sensation was achieved (Deqi), the needle handle was twisted clockwise until the needle body appeared to be tight and stuck. Then the doctor gave a small-amplitude,fast-frequency lifting thrusting manipulation for 1 min.Before withdrawing the needle, the doctor twisted the needle in a counterclockwise direction until the needle body was free. Treatment was given once every 2 d for a total of 2 weeks.
All patients were operated on by the same group of doctors, and the doctors had been trained before the operation on specific details such as the treatment and the locations of acupoints.
3 Observation of Therapeutic Efficacy
3.1 Observation items
3.1.1 Primary efficacy measures
The primary efficacy measures were pain and swelling,which were assessed before treatment and after 3 d, 7 d and 14 d of treatment.
Pain was scored using the VAS[9], with a score of 0 point representing no pain and 10 points representing the most severe pain.
The degree of swelling was measured using a modified“8” ankle measurement including the circumference of the affected and the healthy ankle[10]. The degree of swelling was defined as the difference between the affected and healthy ankle circumferences. Two measures were obtained and averaged.
3.1.2 Secondary efficacy measure
The secondary efficacy measure was the function of ankle, assessed before treatment and after 3 d, 7 d and 14 d of treatment.
The function of ankle was assessed by the American Orthopedic Foot Ankle Society (AOFAS) ankle-hindfoot scale score, with a higher score indicating better ankle function[11].
3.2 Results
3.2.1 Comparison of the VAS score
Before treatment, there was no statistically significant difference in the VAS score of pain between the two groups (P>0.05). After treatment, the VAS scores of both groups showed a decreasing trend over time, and all the differences within the groups were statistically significant (P<0.05). After 3 d, 7 d and 14 d of treatment,the VAS scores in the treatment group were lower than those in the control group, with statistically significant differences (P<0.05). The test of model effect suggested a significant time × intervention interaction effect(F=22.734,P<0.001). See Table 2 for details.
3.2.2 Comparison of the degree of swelling
Before treatment, there was no statistically significant difference in the degree of swelling between the two groups (P>0.05). After treatment, the degrees of swelling in both groups showed a decreasing trend over time, and all the differences within the groups were statistically significant (P<0.05). After 3 d and 7 d of treatment, the degrees of swelling in the treatment group were lower than those in the control group, with statistically significant differences (P<0.05). There was no statistical difference in the degree of swelling between the two groups after 14 d of treatment (P>0.05). The tests of model effect suggested a significant time × intervention interaction effect (F=34.572,P<0.001). See Table 3 for details.
3.2.3 Comparison of the function of ankle
Before treatment, there was no statistically significant difference in the AOFAS ankle-hindfoot scale score between the two groups (P>0.05). After treatment, the AOFAS ankle-hindfoot scale scores of both groups showed an increasing trend over time, and all the differences within the groups were statistically significant (P<0.05). After 3 d, 7 d and 14 d of treatment,the AOFAS ankle-hindfoot scale scores in the treatment group were higher than those in the control group, with statistically significant differences (P<0.05). The test of model effect suggested a significant time × intervention interaction effect (F=38.348,P<0.001). See Table 4 for details.
Table 2. Comparison of the VAS score between the two groups ( ±s point)
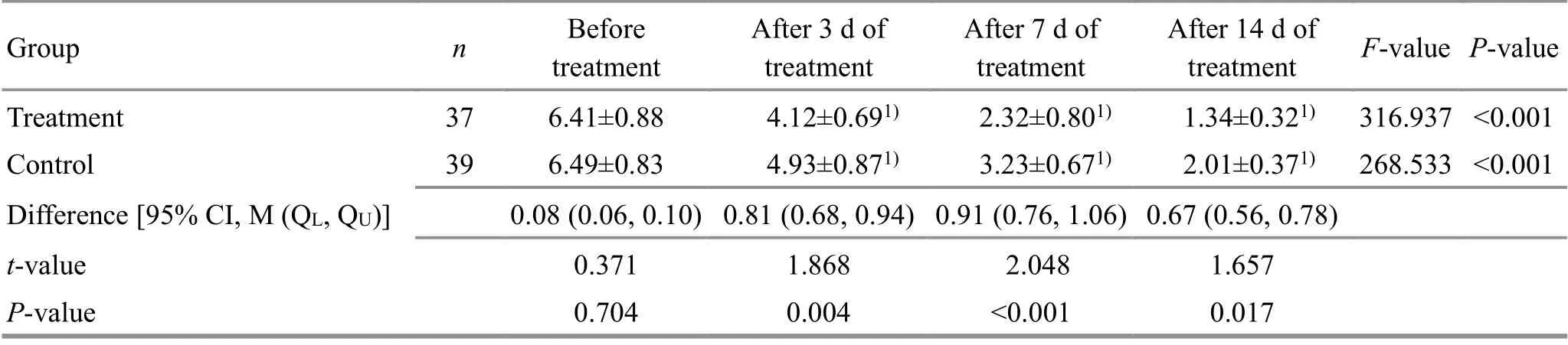
Table 2. Comparison of the VAS score between the two groups ( ±s point)
Note: CI=Confidence interval; compared with the same group before treatment, 1) P<0.05
Group n Before treatment After 3 d of treatment After 7 d of treatment After 14 d of treatment F-value P-value Treatment 37 6.41±0.88 4.12±0.691) 2.32±0.801) 1.34±0.321) 316.937 <0.001 Control 39 6.49±0.83 4.93±0.871) 3.23±0.671) 2.01±0.371) 268.533 <0.001 Difference [95% CI, M (QL, QU)] 0.08 (0.06, 0.10) 0.81 (0.68, 0.94) 0.91 (0.76, 1.06) 0.67 (0.56, 0.78)t-value 0.371 1.868 2.048 1.657 P-value 0.704 0.004 <0.001 0.017
Table 3. Comparison of the degree of swelling between the two groups ( ±s cm)

Table 3. Comparison of the degree of swelling between the two groups ( ±s cm)
Note: CI=Confidence interval
Group n Before treatment After 3 d of treatment After 7 d of treatment After 14 d of treatment F-value P-value Treatment 37 4.46±0.45 2.04±0.761) 0.52±0.141) 0.33±0.071) 436.463 <0.001 Control 39 4.23±0.64 3.09±0.811) 1.23±0.221) 0.41±0.061) 410.741 <0.001 Difference [95% CI, M (QL, QU)] -0.23 (-0.27, -0.19) 1.05 (0.88, 1.22) 0.71 (0.60, 0.82) 0.08 (0.06, 0.10)t-value 0.171 3.367 2.162 0.783 P-value 0.847 <0.001 <0.001 0.319
Table 4. Comparison of the AOFAS ankle-hindfoot scale score between the two groups ( ±s point)
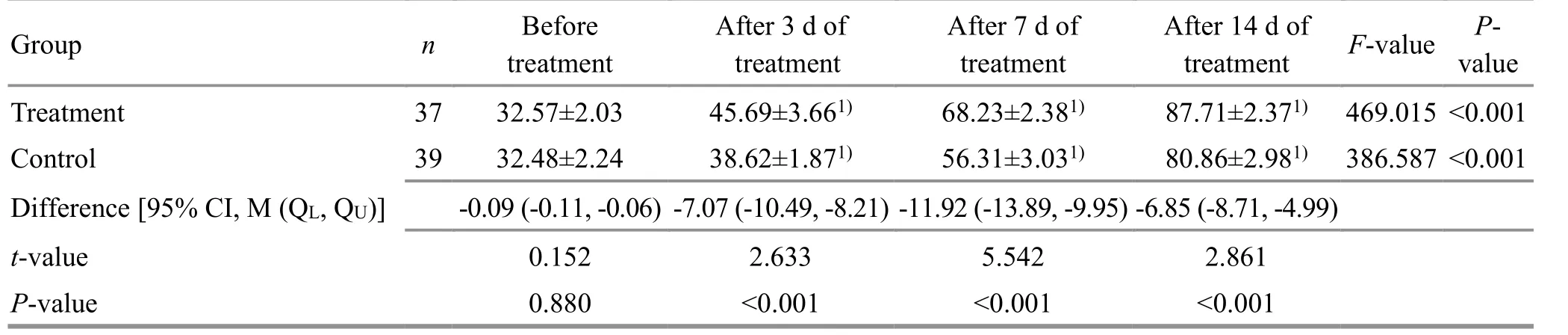
Table 4. Comparison of the AOFAS ankle-hindfoot scale score between the two groups ( ±s point)
Note: CI=Confidence interval
After 14 d of treatment F-value Pvalue Treatment 37 32.57±2.03 45.69±3.661) 68.23±2.381) 87.71±2.371) 469.015 <0.001 Control 39 32.48±2.24 38.62±1.871) 56.31±3.031) 80.86±2.981) 386.587 <0.001 Difference [95% CI, M (QL, QU)] -0.09 (-0.11, -0.06) -7.07 (-10.49, -8.21) -11.92 (-13.89, -9.95) -6.85 (-8.71, -4.99)t-value 0.152 2.633 5.542 2.861 P-value 0.880 <0.001 <0.001 <0.001
4 Discussion
Acute ankle sprain is a common orthopedic disorder in the emergency department, with the prevalence of 1 in 10 000 people every day. Surveys found that up to 50%-60% of patients experienced long-term ankle instability,which not only affected the patient's daily work but also increased the medical burden on society. Among them,a high proportion of patients failed to receive appropriate treatment[12-13].
Grades Ⅰ and Ⅱ acute ankle sprains are caused by trauma which damages the tendons and veins and leads to blood overflowing outside the veins. Blood stasis accumulates and makes local Qi and blood run poorly,blocks the meridians and causes pain. The location of the disease is mainly in the tendons. “Joint subluxation and tendon off-position” are the basic theory of soft tissue injury in traditional Chinese medicine (TCM). Joint subluxation refers to the imbalance of joint stability caused by trauma; tendon off-position refers to the abnormality of tendon form, structure, position or function[14]. Tendon-regulating is a skillful manipulation on meridians, acupoints, and tendons of the injured area,which has the effect of activating blood circulation,resolving blood stasis, relieving spasm and pain, and can play a role in reducing local soft tissue tension and restoring joint balance[15-16]. This study combined modern anatomy with tendon-regulating manipulation.Firstly, through gentle Tui-Pushing and Rou-Kneading techniques, static blood in the swollen area was allowed to enter the surrounding soft tissue interspaces to promote dissipation of static blood. This was followed by pulling and stretching traction and small-range ankle joint movement manipulation. They could both improve the tension of the surrounding soft tissues and promote local metabolism in the ankle. The local pain in the ankle was reduced after the above manipulations. Finally, the tendons around the ankle were An-Pressed and Rou-Kneaded to further eliminate local soft tissue spasm,loosen tendon adhesions and restore the normal position of the joint. This helped to repair the injured soft tissues at the correct site, restore the pre-injury tension,maintain the balance of the ankle, prevent further ankle sprains caused by ankle instability, and reduce the risk of later osteoarthritis. Studies showed that tendonregulating manipulation could reduce oxidative stress at the injury site, alleviate sterile inflammation, improve local blood circulation, facilitate the dissipation of stasis,and promote the self-healing ability of the injured tissue[17-19]. Lei L[20]applied tendon-regulating manipulation combined with ointment to treat patients with ankle sprain and showed that tendon-regulating manipulation was more effective in relieving pain and swelling after 7 d and 14 d of treatment compared with ointment alone. Liu FL,et al[21]observed the efficacy of tendon-regulating manipulation combined with external herbal wash versus external herbal wash alone in the treatment of acute ankle sprain, and the patients treated with the combination therapy had better pain reduction and higher Kofoed ankle score than those with external herbal wash alone. The results of this study also showed that patients with acute ankle sprain experienced significant improvement in swelling and pain symptoms after receiving tendon-regulating manipulation.
Acupuncture is a classic treatment method in TCM. It belongs to minimally invasive treatment modality and is featured by less pain, high safety and few side effects. It has evident efficacy in the treatment of soft tissue disorders, and is widely used in clinical practice. TCM theory believes that acupuncture works by stimulating the meridian points, activating the meridian qi,promoting the operation of the meridian Qi and blood,and restoring the normal physiological function of Zang-Fu organs, therefore achieving the therapeutic effect on the tissues. Modern research on acupuncture for soft tissue injury found that, acupuncture played a regulatory role on neurohumoral by stimulating local nerve receptors, reducing local inflammatory response and promoting tissue repair; acupuncture can increase the pain threshold and reduce patients' pain sensation[22-24].Sticking-needle acupuncture is a method of acupuncture in which the needle body is twisted with the surrounding soft tissues in one direction after the filiform needle is inserted into the body, and then applied with the manipulation. This technique is more conducive to stimulating the meridian Qi, thus enhancing the needling sensation and allowing for better regulation of the acupoints. Compared with conventional acupuncture,sticking-needle acupuncture has a better analgesic effect.Nie B,et al[25]applied sticking-needle acupuncture to treat knee osteoarthritis. The results showed that 2-week sticking-needle acupuncture was superior to conventional acupuncture in improving symptoms. Fu YQ,et al[26]compared the clinical efficacy of stickingneedle acupuncture with electroacupuncture in the treatment of humeral epicondylitis, and sticking-needle acupuncture was better in pain relief and function restoration. Thus, the present study used sticking-needle acupuncture plus tendon-regulating manipulation to treat acute ankle sprain. Taixi (KI 3), Kunlun (BL 60) and Jiexi (ST 41) were selected for sticking-needle acupuncture treatment. They are located on the inner,anterior, and outer sides of the ankle joint, respectively,so that they can better exert the effect of draining the meridians and relieving pain through stimulation. The results showed that the combination of sticking-needle acupuncture and tendon-regulating manipulation was more effective in alleviating the pain and swelling after ankle sprain and was more conducive to the recovery of ankle function than tendon-regulating manipulation alone.
In conclusion, sticking-needle acupuncture plus tendon-regulating manipulation can effectively alleviate pain and swelling and lead to faster recovery of joint function in patients with acute ankle sprain.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
This work was supported by Science and Technology Planning Project of Traditional Chinese Medicine, Zhejiang Province (浙江省中医药科技计划, No. 2019ZB135).
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received: 10 April 2020/Accepted: 19 December 2020
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Evaluation of the effect of acupuncture on pain of patients with refractory trigeminal neuralgia
- Mild moxibustion plus loratadine tablets for children with allergic rhinitis: a randomized controlled trial
- Therapeutic efficacy observation of Tuina manipulation for pediatric adenoid hypertrophy
- Effect of acupuncture on serum PYY and nesfatin-1 in obese patients with insulin resistance
- Clinical study on Tuina plus umbilical therapy for senile functional constipation
- Evaluation of the clinical efficacy of muscle regions of meridians needling method for refractory facial paralysis based on infrared thermal imaging technology