Evaluation of the effect of acupuncture on pain of patients with refractory trigeminal neuralgia
2021-12-17FatemehLavaeeFaridehRafieeZahraTabassomZahraRanjbar
Fatemeh Lavaee, Farideh Rafiee, Zahra Tabassom, Zahra Ranjbar
1 Oral and Dental Disease Research Center, Oral and Maxillofacial Disease Department, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran
2 Department of Physical Medicine and Rehabilitation of Shiraz University of Medical Sciences, Shiraz, Iran
3 School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran
Abstract
Keywords: Acupuncture Therapy; Trigeminal Neuralgia; Facial Pain; Pain Measurement; Visual Analog Scale
Trigeminal neuralgia (TN) is a severe electric-like neuropathic pain in the trigeminal nerve branches[1-3]. A non-nocuous stimulus induces TN spontaneous provocation. Another characteristic of TN is a refractory period between two separate attacks[3-5]. Several relapses of TN cause poor quality of life[6]. Recalcitrant TN pain is a major challenge for treatment[7-9]. The routinely prescribed medications for TN, like carbamazepine, gabapentin and baclofen, have different side effects[6]. Some studies reported that 25%-35% of TN patients experience long-term pain relief[10-11]. On the other hand, the side effects of surgery are paresthesia and sensory loss[12].

Ahn CB,et al[18]reported the relieving effect of traditional acupuncture on headache, migraine and TN.Another study concluded that meridian acupuncture is an effective treatment for TN[19].
In order to overcome many drug and surgical methods resistance and side effects[20], evaluate other adjunctive or complementary treatment modalities such as acupuncture can improve TN patients’ quality of life, we aimed to assess the therapeutic effect of acupuncture on patients with refractory TN.
1 Clinical Materials
1.1 Diagnostic criteria
The patients who were referred to the Oral and Maxillofacial Medicine Department of Shiraz Dental Faculty and Emam Reza Clinic were examined by a specialist and if they had refractory TN, they were enrolled in the study.
1.2 Inclusion criteria
The patients with refractory TN, who were under pharmacological treatment (carbamazepine with its therapeutic dosage, gabapentin, baclofen, and other routine pharmacological prescriptions for TN) for at least 3 months in Oral and Maxillofacial Medicine Department of Shiraz Dental Faculty and Emam Reza Clinic and still suffered from TN and signed the written consent form.
1.3 Exclusion criteria
The patients who quit acupuncture treatment sessions; new patients diagnosed with TN but not classified as refractory TN; patients with diabetes mellitus and any cerebrovascular diseases and individuals who had a history of dermal skin problems or hypersensitivity.
1.4 Statistical methods
The data were analyzed using SPSS version 18.0 statistical software. The mean values of visual analog scale (VAS) on evaluation days in normal distribution were described as mean ± standard deviation (±s),while the changes between different evaluation days were described as mean and standard error. Repeated measurement was used for comparing the VAS points and their changes between evaluation days. The mean difference is significant at the 0.05 level (P<0.05).
1.5 General data
This study was a clinical trial that was done on patients with refractory TN between 2018 and 2019 and was not blinded. This study was approved by Ethics Committee at Shiraz University of Medical Sciences(IR.SUMS.REC.1398.100). Also, the study has been registered on Iranian Registry of Clinical Trial (IRCT 20120101008585N8). In this clinical trial with one group(there was no control group), finally 14 patients with refractory TN were enrolled. A total of 18 patients with TN were recruited, while 4 patients did not continue the study because of different reasons including complete pain remission, car accident and the long distance from his living place. Finally, 14 patients completed the study.
2 Treatment Method
2.1 Acupoints
Major acupoints: Baihui (GV 20), Waiguan (TE 5),Fenglong (ST 40), Zusanli (ST 36), and Yintang (EX-HN 3).
Adjunct acupoints: Based on the branches of trigeminal nerve, Cuanzhu (BL 2), Yangbai (GB 14) and Yuyao (EX-HN 4) were used for the orbital branch of trigeminal nerve; Sibai (ST 2), Juliao (ST 3) and Quanliao(SI 18) were for the maxillary branch; Jiache (ST 6),Xiaguan (ST 7) and Chengjiang (CV 24) were for the mandibular branch.
2.2 Method
Acupuncture was performed for participants three sessions in a week for ten sessions. Every treatment session lasted about 30 min. The participants’pharmacological treatment continued during acupuncture therapy. Acupuncture needles of 0.18 mm in diameter and 13 mm in length were used for the face and other typical areas for TN. Needles were not manipulated. The insertion depth of the needles depended on the patients’ tissue; the needles were inserted to a depth until the sense of obstruction.According to Chinese physicians, the sensation felt on needling is named ‘Deqi’. Production of Deqi is important because it indicates correct insertion point and depth of the needle, so that better therapeutic results can be achieved. The patient’s sensations are subjective and are divided into four types: numbness, heaviness, soreness,and distension. One or more of these sensations usually radiate along the meridian and may be felt. This characteristic is known as the phenomenon of propagated sensation along the meridian by modern acupuncturists. Even in the missing part of a limb, this phenomenon can happen, so probably radiation is a central neurological happening. The acupuncturist may also feel Deqi (known as the acupuncturist’s Deqi); local muscle spasm leads to feeling a sense of tightening during needling. Different sensations can be felt in different acupoints. Needling in thin muscles produces distension, while it produces numbness or soreness in thick muscles. When needles are inserted near a nerve,a sensation of ‘electric shock’ may be felt through the nerve. Improper needling leads to pain or discomfort which must be distinguished from the sensation of Deqi[21]. This treatment was done by an expert physiatrist in Emam Reza Clinic. The patients who were not willing to continue the treatment had the opportunity to quit the acupuncture treatment.
3 Therapeutic Effect Observation
3.1 Observation item
The pain severity of patients was evaluated by 10-scaled VAS at days 0, 3, 7, 14, 21 and one month later as a follow-up.
3.2 Efficacy criteria
The mean value of VAS at different days and the value of VAS change between different days were assessed for efficacy evaluation of acupuncture.
3.3 Results
A total of 14 patients completed the study. 64.3% of the participants (9 patients) were women and 35.7%(5 patients) were men. The mean age of the participants was (59.4±13.2) years old in a range of 32-76 years old.The mean values of VAS at evaluation days 0, 3, 7, 14, 21 and one-month follow-up were displayed in Table 1 and Figure 1.
The mean VAS points comparisons between different days by repeated measurement (mean difference = VAS- VAS’) and theirPvalues are presented in Table 2. As the results showed, the amount of VAS decreased by acupuncture emerged more significantly in comparisons between days 0, 3 and days 14, 21, and the one-month follow-up.Pvalues also confirmed these significant differences between VAS points on the mentioned days.
4 Discussion
In this study, the patients with refractory TN reported significant pain relief compared with the primary days(days 0, 3, 7) at the beginning of the acupuncture treatment. This analgesic effect reached a significant level on day 14 and continued up to day 21 and 1-month follow-up. These findings reveal that acupuncture can dominate its analgesic effect after multiple repetitions of therapeutic sessions. Since the analgesic effect of acupuncture is prolonged[15], the therapeutic effect has continued till the next evaluation days (day 14, day 21 and one-month follow-up).
Table 1. Mean values of VAS on evaluation days ( ±s, point)
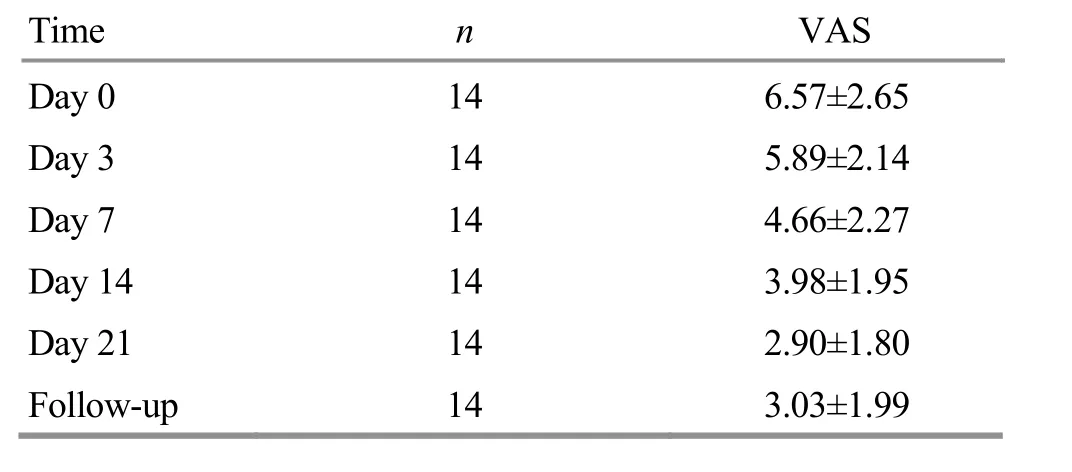
Table 1. Mean values of VAS on evaluation days ( ±s, point)
Time n VAS Day 0 14 6.57±2.65 Day 3 14 5.89±2.14 Day 7 14 4.66±2.27 Day 14 14 3.98±1.95 Day 21 14 2.90±1.80 Follow-up 14 3.03±1.99

Figure 1. Descending trend of VAS changes on evaluation days

Table 2. The mean VAS score comparisons between different days
There are some studies on the analgesic effect of different methods of acupuncture on different causes of headaches and TN. In a study, Shankar A[12]evaluated the effect of acupuncture on patients who had intractable TN. Treatment sessions were three times a week. On day 7 the pain was relieved. On day 15, the patients did not have any pain. After 5 years, just 3 patients had pain.Ichida MC,et al[22]reported TN pain relief even at 6-month follow-up after 10-week sessions of acupuncture.In another study, VAS improvement had been achieved by a 12-session combined traditional acupuncture and ear acupuncture on patients with headache, TN, and retro-auricular pain[19]. Different studies with different methodology have confirmed the analgesic effect of different methods of acupuncture on TN[19,23]. Mo FH[24]reported pain improvement by a different acupuncture protocol, accompanied by electroacupuncture applied for axillary points. They inserted 5 needles into the major acupoint which were manipulated once every 10 min.Literature has concluded the effective rate of 75.0%-95.5%for acupuncture on TN[25-27].
In our study, acupuncture was accomplished for participants by three sessions a week for ten sessions.Every treatment session lasted about 30 min and needles were not manipulated. Insertion depth of needles depended on patients’ tissue; the needles were inserted to a depth with a sense of obstruction. Despite differences in techniques, duration and follow-up, the findings also endorsed the positive effect of acupuncture.Different methods of acupuncture, different acupoints with several depths of insertion and heterogeneity of patients with different head and neck pain in previous studies make the comparison difficult.
Acupuncture can control pain by peripheral and central mechanisms. Peripheral insertion of an acupuncture needle into a specific point causes Deqi sensation and afferent fibers stimulation[28-29]. This nerve stimulation is conducted via interneurons and sensory ganglia to the spinal cord. This can modulate brainstem motor neurons activity, activate the opioid receptors and induce following analgesic effects[29-30]. The analgesic effect of acupuncture which is related to opioid receptor activation is immediate and long-standing[15]. The pathway of diffused noxious inhibitory controls is the possible pathway of immediate pain transmission suppression in trigeminal caudalis and/or spinal horn neurons[31-32]. Endorphin, encephalin and serotonin release in the serum and brain stem, following acupuncture, play important roles for analgesic effect induction[33]. In addition, descendent pain suppression is activated, too[16]. Acupuncture increases the blood flow and oxygenation in cerebellum[34]. This technique changes ionic transmission and concentrations of potassium, sodium and calcium and hyper-polarizes neurons membrane[35]. Also, acupuncture modulates the nociceptive inflammatory reactions, increases adrenocorticotrophic hormones and immunologic responses[36-37]. Acupuncture is a safe modality with few side effects including hematoma, ecchymosis, local infection and metal allergy[22].
Enrolling a large sample size, recruiting some patients as a control group with medication therapy, continuing the treatment session and long-time follow-up are suggested for future research. It seems that since TN has several periods of relapse, continuing the safe treatment sessions of acupuncture can induce more long-standing pain relief periods.
Acupuncture can cause proper pain relief for refractory TN. Acupuncture can induce an analgesic effect after multiple repetitions of therapeutic sessions.
Conflict of Interest
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial or non-financial interest in the subject matter or materials discussed in this manuscript.
Acknowledgement
The authors thank the Vice-Chancellor of Shiraz University of Medical Sciences for supporting this research(Grant No. 18108). This manuscript is based on the thesis by Dr. Zahra Tabassom. The authors also thank Nematollahi of the Center for Research Improvement of the School of Dentistry for the statistical analysis.
Statement of Informed Consent
This study has been registered on Iranian Registry of Clinical Trial (IRCT 20120101008585N8). Informed consent was obtained from all individuals in this study.
Received: 30 January 2021/Accepted: 27 April 2021
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Mild moxibustion plus loratadine tablets for children with allergic rhinitis: a randomized controlled trial
- Therapeutic efficacy observation of Tuina manipulation for pediatric adenoid hypertrophy
- Effect of acupuncture on serum PYY and nesfatin-1 in obese patients with insulin resistance
- Clinical study on Tuina plus umbilical therapy for senile functional constipation
- Evaluation of the clinical efficacy of muscle regions of meridians needling method for refractory facial paralysis based on infrared thermal imaging technology
- Therapeutic efficacy observation of warm needling moxibustion plus spine subtle adjusting manipulation for cervical radiculopathy