rbFGF联合脱细胞异体真皮和自体超薄皮片复合移植修复大面积烧伤创面
2021-12-14徐文虎赵鹏孟素玉马雅宁曹丽莎
徐文虎 赵鹏 孟素玉 马雅宁 曹丽莎
[摘要]目的:探討重组碱性成纤维细胞生长因子(Recombinant basic fibroblast growth factor,rbFGF)+脱细胞异体真皮+自体超薄皮片复合移植修复大面积烧伤深部创面的效果。方法:回顾性分析2017年10月-2020年10月在笔者医院进行治疗的116例大面积烧伤患者一般临床资料,根据患者治疗方式进行分组,将采用rbFGF+自体超薄皮片修复者纳入对照组(n=55),将采用rbFGF+脱细胞异体真皮+自体超薄皮片复合移植修复者纳入实验组(n=61),探讨不同治疗方式对患者深部创面的影响。结果:两组创面愈合后疗效比较差异无统计学意义(95.08% vs 90.91%,P>0.05),但实验组肉芽生长评分明显高于对照组,创面无渗出液时间、结痂时间、创面愈合时间、住院时间均明显短于对照组,差异有统计学意义(P<0.05)。治疗后实验组色泽、柔软度、厚度、血管分布评分均明显低于对照组,差异有统计学意义(P<0.05)。治疗后两组超敏C反应蛋白(hs-CRP)、白介素-6(IL-6)、肿瘤坏死因子(TNF-α)水平均显著降低,且实验组均明显低于对照组,差异有统计学意义(P<0.05)。治疗后两组血管内皮生长因子(VEGF)、表皮细胞生长因子(EGF)水平均显著升高,且实验组均明显高于对照组,差异有统计学意义(P<0.05)。治疗后两组琥珀酸脱氢酶(SDH)、组织液氧分压水平均显著升高,乳酸脱氢酶(LDH)降低,且实验组治疗后SDH、组织液氧分压水平明显高于对照组,LDH低于对照组,差异有统计学意义(P<0.05)。结论:rbFGF+脱细胞异体真皮+自体超薄皮片复合移植在修复大面积烧伤深部创面中应用较佳,创面修复效果良好,抗炎效果较佳,可有效促进肉芽组织生长成熟,缩短创面愈合时间,值得在临床推广应用。
[关键词]rbFGF;脱细胞异体真皮;自体超薄皮片;移植修复;大面积烧伤;深部创面
[中图分类号]R644 [文献标志码]A [文章编号]1008-6455(2021)10-0032-05
Effects of rbFGF Combined with Acellular Allogeneic Dermis and Autologous Ultra-thin Skin Composite Graft in Repairing Deep Wounds of Extensive Burns
XU Wen-hu,ZHAO Peng,MENG Su-yu,MA Ya-ning,CAO Li-sha
(Department of Burn and Plastic Surgery,the Fifth Hospital of Xingtai,Xingtai 054000,Hebei,China)
Abstract: Objective This research aims to investigate the effects of recombinant basic fibroblast growth factor combined with acellular allogeneic dermis and autologous ultra-thin skin composite graft in repairing deep wounds of extensive burns. Methods The general clinical data of 116 patients with extensive burns treated in the hospital from October 2017 to October 2020 were retrospectively analyzed. According to the treatment method, the patients were divided into the control group (rbFGF+autologous ultra-thin skin repair, n=55) and the experimental group (rbFGF+acellular allogeneic dermis+autologous ultra-thin skin composite graft, n=61). Effect of different treatment methods on deep wounds was discussed. Results There was no significant difference in curative effect between the two groups(95.08% vs 90.91%, P>0.05). The granulation growth score of the experimental group was significantly higher than that of the control group, and the time of no exudation, scab formation, wound healing and hospital stay in the experimental group were significantly shorter than those in the control group, the differences were statistically significant (P<0.05). After treatment, the scores of color, softness, thickness and vascular distribution in the experimental group were significantly lower than those in the control group (P<0.05). After treatment, hs-CRP, IL-6 and TNF-α were detected in the two groups, and the levels in the experimental group were significantly lower than those in the control group (P<0.05). After treatment, the levels of VEGF and EGF increased significantly in two groups, the levels o in the experimental group were significantly higher than those in the control group (P<0.05). After treatment, the levels of SDH and tissue liquid oxygen partial pressure increased significantly and LDH decreased in the two groups (P<0.05). After treatment, the levels of SDH and tissue liquid oxygen partial pressure in the experimental group were significantly higher than those in the control group and LDH was lower than those in the control group (P<0.05). Conclusion Applying combined with acellular allogeneic dermis and autologous ultra-thin skin composite graft in repairing deep wounds of extensive burns can achieve good repairing effects,and the anti-inflammatory effect is better.It can effectively promote the growth and maturity of granulation.
Key words: rbFGF; acellular allogeneic dermis; autologous ultra-thin skin; graft repair; extensive burns; deep wound
火焰、蒸汽、热液均会引起皮肤组织烧伤,严重者会导致皮下组织损伤,且烧伤会导致创面缺血、渗出液、水肿,一旦出现感染则会影响创面愈合,且烧伤创面的恢复需要经历体液渗出期、急性感染期、修复期、康复期,前两个时期是影响愈合的主要阶段[1]。为防止大面积烧伤患者出现感染,多采用手术植皮修复创面,另外烧伤后瘢痕挛缩也会影响部分器官功能,导致美学缺陷,手术治疗原则是切除瘢痕、松懈痉挛,并取皮覆盖创面,但皮源有限,部分患者因烧伤面积较大,自身皮源应用面积有限,因此如何应用较少的自体皮肤覆盖烧伤创面是当前临床较为重视的问题[2-3]。近年来,采用邮票皮植皮、Meek植皮、异体皮移植均有一定临床疗效,但不同植皮方式疗效及安全性均有不同[4]。大面积烧伤患者在进行植皮治疗后往往需要采用辅助药物促进烧伤创面愈合、恢复。重组碱性成纤维细胞生长因子(Recombinant basic fibroblast growth factor,rbFGF)是多功能细胞生长因子,且在急性感染期会刺激血管内皮细胞及成纤维细胞,在康复期、修复期可有效促进成纤维细胞及毛细血管生长,进一步改善创面微循环[5]。近年来,rbFGF逐渐应用在创伤、烧伤中。本研究拟分析rbFGF+脱细胞异体真皮+自体超薄皮片复合移植在大面积烧伤创面中的应用价值,旨在为临床美容修复提供有效依据。
1 资料和方法
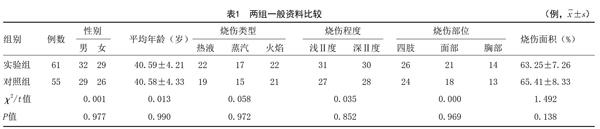
1.1 一般资料:回顾性分析2017年10月-2020年10月在笔者医院进行治疗的116例大面积烧伤患者一般临床资料,根据患者治療方式进行分组,将采用rbFGF+自体超薄皮片修复者纳入对照组(n=55),将采用rbFGF+脱细胞异体真皮+自体超薄皮片复合移植修复者纳入实验组(n=61),两组一般资料有可比性(P>0.05),见表1。
1.2 纳入及排除标准:纳入标准:①所有患者均诊断为Ⅱ度烧伤[6];②患者及家属均知情同意;③均需进行植皮治疗者;④均签署医院伦理委员会出具的知情同意书。排除标准:①合并严重心、肝、肾器质性疾病者;②创面存在大面积出血者。
1.3 方法:对照组采用rbFGF+自体超薄皮片移植修复:给予全身麻醉,电凝止血,根据自身皮源选择侧胸、大腿、上臂外侧、背部的真皮,并用电动取皮刀在供皮区取超薄皮片覆盖创面,丝线固定,并采用1~4支rbFGF与溶媒混合后均匀喷洒在纱布上,采用石膏固定功能部位,2~3周拆线。
实验组采用rbFGF+脱细胞异体真皮+自体超薄皮片复合移植修复:给予全身麻醉,电凝止血,采用无菌液洗脱细胞异体真皮3次,在移植时确保异体真皮粗糙面朝下贴敷创面,光洁基底膜面朝上,并确保异体真皮与创面无褶皱、气泡、渗液,开放网眼,使用丝线间断缝合固定异体真皮在创面边缘,并在丝线固定后于上层覆盖自体超薄皮片进行复合移植,采用丝线固定后纱布加压包扎,并采用1~4支rbFGF与溶媒混合后均匀喷洒在纱布上,采用石膏固定功能部位,2~3周拆线。两组均定期更换敷料,积极行抗感染治疗。
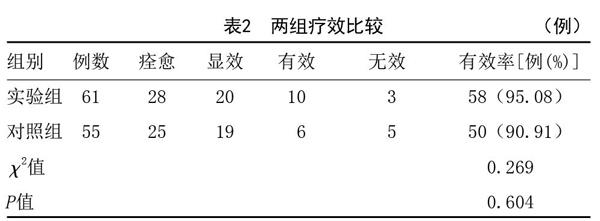
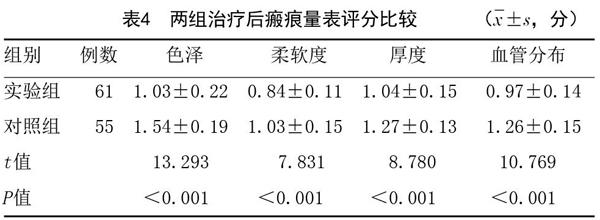
1.4 观察指标:①依据文献[7]比较两组疗效,痊愈:创面愈合率在90%及以上;显效:创面面积明显缩小,且肉芽组织新鲜红色上皮爬行良好,无坏死组织及脓苔无浸润,创面愈合率60%~89%;有效:创面面积缩小,肉芽组织存在轻度水肿,伴随少量脓苔及坏死组织,创面愈合率30%~59%;无效:创面无明显好转,创面愈合率在30%以下;治疗有效率为痊愈、显效、有效例数;②记录两组肉芽生长评分、创面无渗出液时间、结痂时间、创面愈合时间、住院时间:其中肉芽生长评分:0分(有明显肉芽组织生长,且覆盖面积在1/4以下)、1分(肉芽组织生长且覆盖创面1/4~1/2)、2分(肉芽组织生长较好且覆盖创面1/2以上,颜色鲜红)、3分(肉芽组织生长较好,覆盖全部创面,鲜红色);③采用温哥华瘢痕量表((Vancouver scar scale,VSS)对患者愈后创面瘢痕进行评分,主要包括色泽、血管分布、厚度、柔软度,色泽评分:瘢痕皮肤颜色与其他部位颜色接近记0分,瘢痕色泽变浅记1分,瘢痕色泽混合记2分,瘢痕色泽变深记3分;血管分布评分:血管分布与其他部位相近记0分,血管偏粉色记1分,血管偏红色记2分,血管呈现紫色记3分;柔软度评分:柔软度正常记0分,柔软度有较小阻力导致皮肤变形记1分,在压力下皮肤出现变形记2分,瘢痕处皮肤呈硬块记3分;厚度评分:瘢痕厚度正常记0分,瘢痕厚度为1mm记1分,瘢痕厚度1~2mm记2分,瘢痕厚度2~4mm记3分,瘢痕厚度>4mm记4分;④在治疗前及治疗结束时将残留药物及分泌物清除干净后选取创面基底部组织,并采用眼科剪取少许创面组织,充分碾碎后制成匀浆,离心后取上清液保存待检,采用ELISA法检测患者治疗前后血管内皮生长因子(Vascular endothelial growth factor,VEGF)、表皮细胞生长因子(Epidermal growth factor,EGF)及炎症因子水平,炎症因子包含超敏C反应蛋白(High sensitivity C-reactive protein,hs-CRP)、白介素-6(Interleukin-6,IL-6)、肿瘤坏死因子(Tumor necrosis factor,TNF-α);⑤在治疗前后清洗创面,并夹闭引流管后采用肝素湿润的注射器抽取0.5~1.0ml组织新鲜渗出液,并采用血气分析仪检测组织液氧分压,并于创面处取出肉芽组织,融化后加入PBS液,离心后采用ELISA法检测乳酸脱氢酶(Lactate dehydrogenase,LDH)、琥珀酸脱氢酶(Succinate dehydrogenase,SDH)。
[3]Song CL,Yao M.Advances in the research of relationshipbetween CD26 and hypeatrophic scar and keloid[J].Zhonghua Shaoshang Zazhi,2018,34(1):54-56.
[4]Houschyar KS,Tapking C,Nietzschmann I,et al.Five years experience with meek grafting in the management of extensive burns in an adult burn center[J].Plast Surg(Oakv),2019,27(1):44-48.
[5]向光俊.rbFGF联合负压引流对Ⅱ度烧伤患者创面愈合的影响[J].河北医学,2018,24(8):1343-1346.
[6]吴在德,吴肇汉.外科学[M].7版.北京:人民卫生出版社,2008:180-181.
[7]付小兵,王德文.現代创伤修复学[M].北京:人民军医出版社,1999:23.
[8]Mai B,Gao Y,Min L,et al.Photodynamic antimicrobial chemotherapy for Staphylococcus aureus and multidrug-resistant bacterial burn infection in vitro and in vivo[J].Int J Nanomedicine,2017,12:5915-5931.
[9]Plichta JK,Gao X,Lin H,et al.Cutaneous burn injury promotes shifts in the bacterial microbiome in autologous donor skin: implications for skin grafting outcomes[J].Shock,2017,48(4):441-448.
[10]肖昌明,银西洋,刘玉文.复合皮移植技术与传统方法治疗烧伤后大面积瘢痕效果比较[J].医学与哲学,2018,39(16):32-34.
[11]周丽娜,张斌杰.持续封闭负压引流技术联合rb-bFGF冲管治疗在慢性创面修复中的临床效果[J].广西医科大学学报,2018,35(8):1100-1104.
[12]Majid I,Imran S.Ultrathin skin grafting in resistant stable vitiligo[J].Dermatol Surg,2017,43(2):218-225.
[13]刘明,唐乾利,李杰辉,等.烧伤湿润暴露疗法及湿润烧伤膏治疗糖尿病足的效果及对创面组织血管内皮生长因子和表皮细胞生长因子水平的影响[J].广西医学,2018,40(11):1157-1160,1171.
[14]邓斌,李蔓青,张拥军,等.Meek植皮与邮票植皮在大面积深度烧伤创面修复中的疗效比较[J].中国美容医学,2019,28(7):66-69.
[15]石聪,王东凯,耿志辉.龙血竭联合重组牛碱性成纤维细胞生长因子凝胶治疗烧烫伤临床研究[J].河北医科大学学报,2018,39(10):1217-1220.
[16]陈志兵,周建文,王晓,等.复合皮移植术对大面积烧伤患者血管紧张素Ⅱ、CD46及炎症因子水平及愈合的影响[J].检验医学与临床,2019,16(17):2513-2515.
[17]黄晓栋,陈晓武,万里,等.自体皮片移植结合异体真皮在烧伤致功能部位瘢痕挛缩畸形中的应用[J].中国美容整形外科杂志,2020,31(11):650-652,697.
[18]杨薛康,陈俏华,张月,等.颞浅筋膜瓣游离移植联合皮片移植修复大面积烧伤患者踝后区深度创面的效果[J].中华烧伤杂志,2019,35(1):62-64.
[19]郭海雷,凌翔伟,刘政军,等.刃厚头皮与异体脱细胞真皮基质复合移植修复特大面积烧伤患者手部深度创面[J].中华烧伤杂志,2019,35(12):876-878.
[20]李文生,徐银兰,武延朋,等.脱细胞异体真皮与自体瘢痕组织联合自体刃厚皮复合移植修复大面积烧伤后畸形的疗效比较[J].新乡医学院学报,2019,36(12):1175-1178.
[收稿日期]2021-03-16
本文引用格式:徐文虎,赵鹏,孟素玉,等.rbFGF联合脱细胞异体真皮和自体超薄皮片复合移植修复大面积烧伤创面[J].中国美容医学,2021,30(10):32-36.
