Six-minute walking test performance is associated with survival in cirrhotic patients
2021-12-06CarolinaFradePimentelAnaCristinadeCastroAmaralAdrianoMiziaraGonzalezMichelleLaiDanieldeOliveiraMotaMariaLuciaGomesFerrazWilsonMathiasJuniorMarioKondo
Carolina Frade M G Pimentel,Ana Cristina de Castro Amaral,Adriano Miziara Gonzalez,Michelle Lai,Daniel de Oliveira Mota,Maria Lucia Gomes Ferraz,Wilson Mathias Junior,Mario Kondo
Carolina Frade M G Pimentel,Department of Medicine,Federal University of Sao Paulo,Sao Paulo 04026090,Brazil
Ana Cristina de Castro Amaral,Maria Lucia Gomes Ferraz,Mario Kondo,Department of Gastroenterology,Federal University of Sao Paulo,Sao Paulo 04023062,Brazil
Adriano Miziara Gonzalez,Department of Surgery,Liver Transplantation Service,Federal University of Sao Paulo,Sao Paulo 04026090,Brazil
Michelle Lai,Department of Medicine,Division of Gastroenterology and Hepatology,Beth Israel Deaconess Medical Center,Boston,MA 02215,United States
Daniel de Oliveira Mota,Department of Industrial Engineering,University of Sao Paulo,Sao Paulo 05508010,Brazil
Wilson Mathias Junior,Department of Cardiology,Heart Institute,University of Sao Paulo,Sao Paulo 05403900,Brazil
Abstract BACKGROUND Patients with cirrhosis are at risk of cirrhotic cardiomyopathy,with resulting cardiac dysfunction and exercise limitations.Six minute walking test(6MWT)assesses functional status and predicts morbidity and mortality in cardiopulmonary diseases.AIM To determine if it associates with mortality by analyzing 6MWT performance in patients with liver cirrhosis.METHODS A cohort of 106 cirrhotic patients was evaluated in the outpatient setting with echocardiogram and 6MWT and follow up for one year to document hepatic decompensation and mortality.The distance in meters was recorded at the end of 6 min(6MWD).RESULTS This cohort had a mean age of 51 years and 56% male;patients were staged as Child A in 21.7%,B 66% and C 12.3%.Walk distance inversely correlated with Child scores,and was significantly reduced as Child stages progresses.Patients who died(10.4%)showed shorter mean 6MWD(P = 0.006).Low 6MWD was an independent predictor of mortality(P = 0.01).CONCLUSION 6MWT is a noninvasive inexpensive test whose result is related to Child scores and mortality.It is useful to identify patients with liver cirrhosis at high risk of mortality for closer monitoring and potential early intervention.
Key Words:Six-minute walking test;Liver cirrhosis;Hospital admission and mortality;Child score
INTRODUCTION
Liver cirrhosis is related to functional impairment leading to reduction in physical fitness[1,2].Some possible factors implicated in this process are profound muscle wasting(or cirrhotic myopathy)[3],cardiac dysfunction(cirrhotic cardiomyopathy)[4],autonomic dysfunction(chronotropic incompetence)and concurrent pulmonary disease(portopulmonary hypertension and hepatopulmonary syndrome).Recently studies reinforce the importance of frailty scores as a prediction of mortality in liver transplantation list[5,6],giving emphasis in sarcopenia and physical fitness as important factors associated with mortality[7].
The six-minute walk test(6MWT)is a practical simple inexpensive test that provides a global assessment of all systems involved during exercise[8].Although it does not give information about specific organ impairment,it evaluates overall exercise capacity and has been shown,in patients with cardiac disease,to correlate with the maximal oxygen consumption(VO2)and survival[9].
Some studies demonstrated that short distance during 6MWT(6MWD)predicted poorer prognosis and disease outcome in patients with heart failure[10]and chronic obstructive pulmonary disease[11].In addition,this test can be used to assess the overall functional status and quantify response to a certain intervention[8]in a variety of other chronic diseases and in the elderly population[9-12].
Previous studies highlight the importance of 6MWD in predicting survival in cirrhotic and non-cirrhotic patients[13-16].There are also evidences suggesting an association between exercise performance and increase risk of death on the waiting liver transplantation list[15-18].Despite its role in long term survival in different chronic diseases,the impact in mortality prediction in cirrhotic patients is underestimated over years.
The aim of this study was to analyze the association between 6MWT and long-term mortality in a cohort of cirrhotic patients.
MATERIALS AND METHODS
A total of 106 outpatients with liver cirrhosis(57 male,mean age 51.2 ± 12.9 years)was included in the present study.Cirrhosis was defined by clinical history,physical examination,laboratory analysis and at least one imaging data.Disease prognosis and severity were established based on Child and MELD scores,according to original scores definitions[19,20].Exclusion criteria were any previous or current cardiovascular or pulmonary disease,heart failure or diagnosis of hemochromatosis(when cardiac involvement was documented).Patients who had a history of alcohol abuse(more than 20 g and 60 g of ethanol per day for women and men,respectively)[21]were included if they had abstained from alcohol use for at least 6 mo prior to enrollment.Patients with non-sinus rhythm,decompensated arterial hypertension,low peripheral oxygen saturation(SpO2< 90%),recent history(less than 3 mo)of new liver related decompensation or hospitalizations were also excluded(patients with previous ascites or encephalopathy were included,those characterized with chronic decompensated patients).Patients with neuromuscular diseases,myopathy,balance deficits or orthopedic disorders were also excluded.Patients who have previously received a liver transplant were not included.No paracentesis was performed within at least one week prior to exercise,avoiding volume depletion or electrolyte imbalances.
One hundred and sixty-four patients were consecutively screened from two liver transplantation centers between October 2014 and December 2014,58 out of 164 were excluded according to previous criteria,most of the due to cardiovascular disorders(26%)or active alcohol consumption(19%).On the day of enrollment,patients provided written informed consent and had blood samples collected and 6MWT done.Electrocardiogram and transthoracic bubble echocardiogram were performed within 1 mo of enrollment.
Patients were followed-up by clinical visits,hospital records or telephone calls to patients to capture deaths and their causes.Patients were stratified according to their ability to complete 6MWT,whether they achieved or not predicted distance according to gender and age,and pattern of symptom secondary to physical effort due to the test.Patients included were follow-up to one year,main outcomes were defined as death or liver transplantation.
The study has been performed in accordance with the Declaration of Helsinki(2000)and approved by the Ethics Committee of our institution.
6MWT
The 6MWT was conducted according to American Thoracic Society guidelines[8]and supervised by a qualified physician.The test was performed indoors,along a 30 m flat,straight corridor with a hard surface and free of any type of obstacles.Before starting the test,all patients were provided instructions by the evaluator,encouraged to walk as far as possible within 6 min,and instructed to stop if pain,dyspnea,or other symptoms.The distance in meters was recorded at the end of the six minutes(6MWD).Predicted distances were computed according to specific equations for gender,weight,height and age[22].Predicted distance achieved percentage(%6MWD)is then derived by dividing the actual 6MWD divided by the predicted distance.
Statistical analysis
Data were analyzed using a statistical software program(IBM®SPSS®Statistics,version 22.0).Logistic regressions were performed to evaluate the independent association between 6MWD and death.Receiver operating curves(ROC)and the area under ROC(AUROC)were computed to estimate sensitivity,specificity and cut-off points for 6MWD used in regression models,selected by Youden’s index.COX regression analysis and Kaplan-Meier curves were performed and significant differences between the later were assessed by means of the log-rank test.We performed subgroup analysis according achievement of liver transplantation in order to evaluated 6MWT distance as a predictor of death.
RESULTS
Patient characteristics
The main demographic,clinical,and laboratory characteristics of the patients are presented in Table 1.One hundred and six patients were selected from two liver transplantation centers in Sao Paulo,Brazil.The majority was male(56%),and nonalcoholic etiology of the liver disease was the most common(69.8%).The mean MELD was 11.1,Child B more common(66%),and 74% of patients presented a history of at least one liver related decompensation.Ascites was identified in 32.1% and hepatic encephalopathy in 10.4% of patients on the day of the test.
All patients were followed until death,time of transplantation or end of study follow-up(12 mo).During the study period,11 patients died and 3 underwent liver transplantation.All deaths were related to hepatic decompensation.
The majority of this cohort(71.7%)did not achieve the predicted distance adjusted for age and gender according to standardized equations[22](678 ± 131m,402-890 m)(see Figure 1).6MWT performance is demonstrated in Table 2.The mean 6MWD of this cohort was 515 ± 138 m,180-960 m.Not surprisingly,older patients with higher Child score,worse hepatic synthetic function(lower albumin)and anemia performed worse.It was found to be inversely correlated with age(r= -0.391,P< 0.001)and Child score(r= -0.228,P= 0.019),and positively correlated with albumin(r= 0.242,P= 0.012),creatinine(r= 0.242,P= 0.018)and hemoglobin(r= 0.192,P= 0.048).Patients with a history of at least one hepatic decompensation in the past(74.5%)presented with significant shorter 6MWD(496 ± 141 mvs571 ± 115 m,P= 0.015).
The mean 6MWD was progressively shorter among Child classes(A = 570 ± 144 m,B = 504 ± 137 m and C = 471 ± 115 m)and statistical significance was demonstrated between Child A and C(P= 0.04)and when Child A was compared with more advanced stages(B and C),P= 0.02.6MWD was different among compensated(Child Pugh A)and decompensated(Child Pugh B and C)patients(P= 0.031)(see Figure 2).Patients decompensated with ascites or hepatic encephalopathy on the day of the test achieved shorter distances than those who did not have ascites or hepatic encephalopathy(472vs534m,P= 0.03;440vs525m,P= 0.04,respectively).All patients previously included were submitted to 6MWT,even those with hepatic decompensation at the moment of evaluation,ascites or encephalopathy.6MWD did not differ according to the etiologies of cirrhosis(P= 0.08),past history of alcohol abuse(P= 0.58),use of beta-blocker(P= 0.19),tobacco(P= 0.97)and presence of anemia(P= 0.84).
None of the patient presented with liver related decompensation within 2 wk following the exercise,meaning no detectable clinically significant portal hypertension increase induced by exercise.All patients were able to perform exercise adequately,without help,interruptions,or any significantly adverse effect.
To emphasize the role of 6MWD and %6MWD in the prediction mortality,as an additional factor besides liver disease severity,logistic regression models were designed to evaluate if the inclusion of 6MWT parameters improves the model performance and increases the AUROC computed using regression models.MELD and Child score were used to quantify the severity of liver disease.When 6MWT parameters were added to the models designed to predicted mortality using MELD or Child score,we observed an improvement in model performance,defined as a significant difference according to Omnibus Chi-square test(P= 0.01)and higher AUROCs in combining models(see Figure 3).
Cutoff points associated with mortality was 387 m for 6MWD(sensibility 90.9 and specificity 88.4)and 0.82 for %6MWD(sensibility 100 and specificity 83.2).After exclusion of patients who were submitted to liver transplantation,patients who died(11,10.4%)had a shorter mean 6MWD(423 mvs526 m,P= 0.006)and lower %6MWD(0.72vs0.92,P= 0.004).Just one of them achieved the predicted distance during 6MWT.6MWD and %6MWD were independent predictors of mortality,after adjusted for Child scores,according to multivariate regression model analysis(Table 3).Patients who achieved distances shorter than 387 m or %6MWD < 0.82 presented higher mortality,and statistical difference according to Kaplan-Meier and log-rank analysis(P= 0.004 andP= 0.006,respectively)(Figure 4).
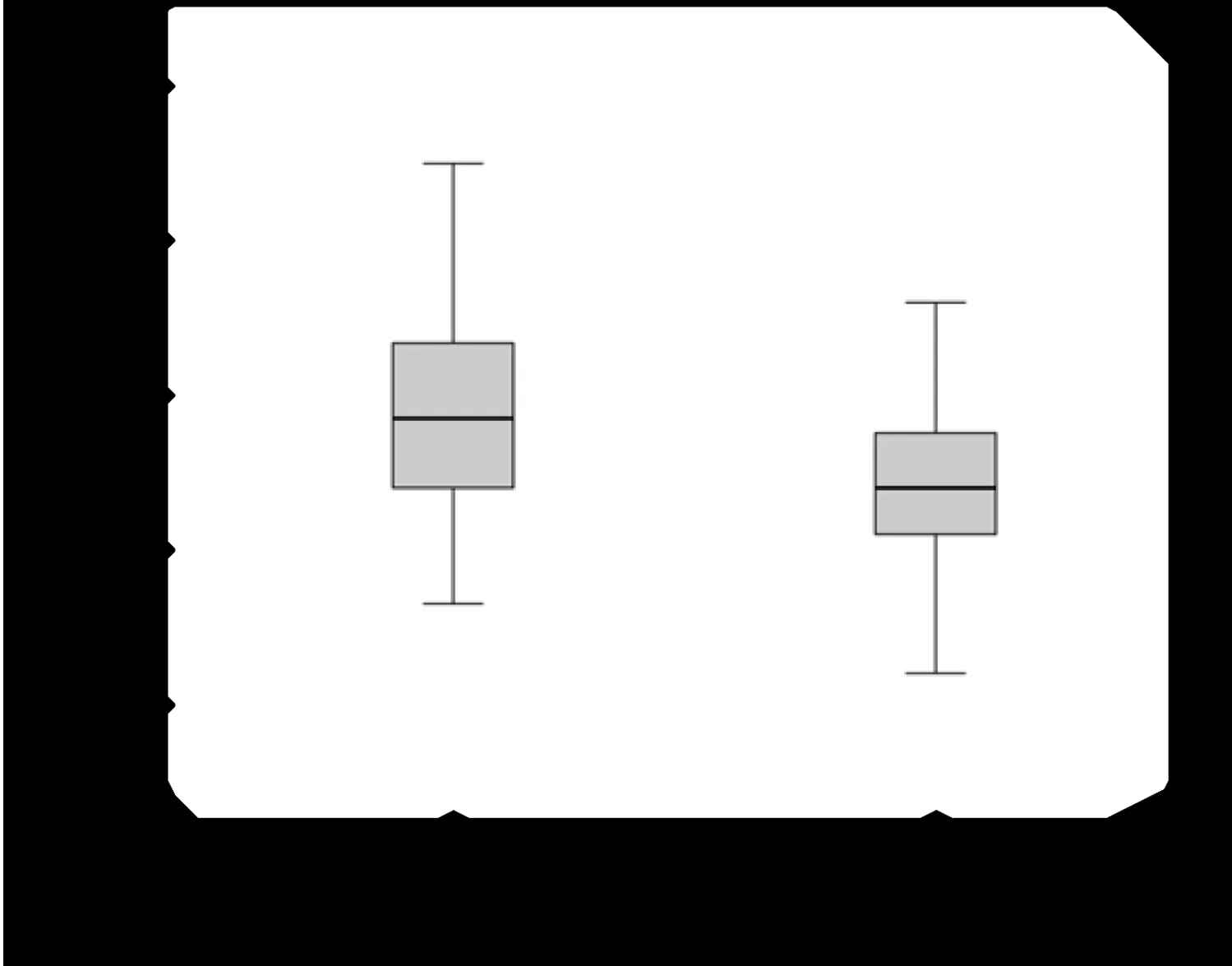
Figure 2 Distance in meters was recorded at the end of the six minutes among compensated(Child Pugh A)and decompensated(Child Pugh B and C)patients
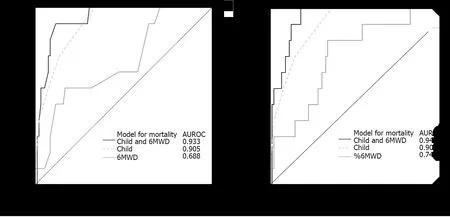
Figure 3 Progressive improvement in prediction of mortality using models combing six minute walking test parameters and Child scores.6MWD:Six minute walking distance.
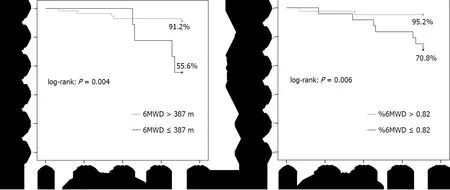
Figure 4 Kaplan Meier analysis for overall survival.

Table 3 Association between six-minute walking test parameters and unfavorable clinical outcomes(hospital admissions and mortality)using logistic regression models

Figure 1 Relationship between predicted(line)and performed(bars)walking distance during six minute walking test.6MWD:Six minute walking distance.

Table 1 Patients’ characteristics(n = 106),n(%)

Table 2 Six minute walking test performance in 106 patients with liver cirrhosis
DISCUSSION
6MWT is a safe,easy-to-administer,and inexpensive test to determine the functional capacity of cirrhotic patients and also has prognostic value.We found that a decreased6MWD,as a marker of impaired exercise capacity,is associated with hepatic dysfunction.In addition,6MWD and %6MWD performed as independent predictors of mortality,becoming an important tool during risk evaluation of severe complications and death in liver cirrhosis.Also,this study reinforces the key importance of physical evaluation during cirrhotic patients,especially those referred to liver transplantation team.
Basal exercise capacity was significantly impaired in our patients,as only 28.3% achieved the pre-test predicted distance.The 6MWD results in our cohort of patients was similar to previous studies in patients with cirrhosis which found a significantly lower 6MWD values than expected for healthy population[22].Our cohort had a mean 89.7%(34.8%-149%)of predicted 6MWD(vs63% found by Románet al[18],and a mean6MWD of 515 m(180-960 m),compared to 306 m in Alameriet al[14]‘s cohort of 98 patients with cirrhosis.The poor performance during 6MW T meets with the current knowledge about the abnormal exercise capacity in cirrhotic patients.Future studies should verify those findings and evaluate if 6MWD can be used as a more general tool able to evaluate outcomes and quality of life in this group[15].
We reported a weak inverse correlation between 6MW D and Child scores(r= -0.228,P= 0.019),although it was clear the tendency in walk distance reduction along Child classes.Careyet al[15],studying 121 cirrhotic patients,showed a strong correlation with MELD.In this particular study,all patients were listed for liver transplant,denoting a population with more advanced disease,making us understand that this stronger correlation reflects a major prevalence of their patient’s overall disability when comparing to our study group.In the same way,by comparing subjects with advanced disease(Child B and C)and those without it(Child A),we detected a significant difference between these groups(P= 0.02),supporting the previous interpretation.Furthermore,patients with a history of at least one hepatic decompensation in the past,presented shorter 6MW D(P= 0.015)and subjects presenting with ascites or encephalopathy at the moment of evaluation performed worse,these facts highlight the relationship between shorter distances and severity of liver disease in our study.Similarly,W onget al[23]reported that patients with decompensated cirrhosis with ascites performed worse during cycle ergometer evaluation when compared to well compensated patients,however,no specific data is available regarding 6MWT.
Although the gold standard measurement of exercise capacity is maximal VO2[24]measurement during treadmill or cycle ergometer tests,6MW T is a cheap and simple test found to correlate with oxygen consumption that can be administered without special equipment or skilled staff that you can perform in clinic to give an immediate result.Noticeable that all patients in our study completed the full test,independently of the presence of ascites or encephalopathy,demonstrating one great advantage above other exercise tests,that sometimes require a more complex adaptation and comprehension about the technique.Cahalinet al[9]performed 6MWT and symptomlimited cardiopulmonary exercise testing in patients with heart failure during cardiac transplant evaluation.The authors described a significant correlation between 6MWD and peak VO2(r= 0.64,P< 0.001),concluding that 6MWT is a valuable tool to predict VO2and short-term survival.These results should be validated in cirrhotic population,but represent a good evidence that 6MWT could be introduced in routine practice without loss of diagnostic accuracy in exercise capacity estimation.While our study did not evaluate the association between VO2and 6MWD,it did show the safety and practicality of this procedure.García-Pagànet al[25]reported that moderate exercise(30% of the maximum)significantly increases portal pressure in patients with portal hypertension,and,therefore,could increase the risk of variceal bleeding,ascites and encephalopathy.Although 6MWT is a submaximal exercise,we did not identify any clinical event directly associated with it during the period following the test.Recent studies do not mention the prevalence of adverse events induced by exercise,and more studies designed to respond this issue should be carried out.
Previously studies who reported the relationship between 6MWT and mortality were conducted with small populations and during a short period of followup[11,12].Poor performance during 6MWT may warrant that the at-risk patients should be followed more closely due to the risk of adverse events.Notwithstanding,6MWT has been proposed as a tool during frailty status evaluation,giving emphasis in this role as a practical and cheap method for this proposal.This study reinforces this importance,adding more powerful results due to our long period of follow-up,demonstrating how physical exercise evaluation may be an interesting long predictor of prognosis in cirrhotic patients.
In our study,6MWD was an independent predictor of death,consistent with findings from previous studies by Alameriet al[14],and Careyet al[15].In the first study,mortality was evaluated in the whole group,including patients with noncirrhotic chronic hepatitis,which may bias the interpretation about causality between 6MWD and cirrhosis.Also,Careyet al[15]studied a population with more advanced disease,all of them on the liver transplant waiting list with a high frequency of liver transplantation(50.4%)performed in a short period of time(5-6 mo).The statistical power of 6MWT in predicting mortality could be affected by pulling out so many patients after transplant from this cohort.
The role of 6MWD and %6MWD in the prediction of mortality were independently of Child scores as demonstrated by multivariate logistic regression analysis.These facts highlight the association of 6MWT parameters with disease progression and adverse outcomes,despite the severity of liver disease.
There are several limitations to our study.First,we did not proceed an external validation of 6MWD cutoffs used in our study,although our main objectives were focused in the transversal and descriptive characterization of study population.Second,we did neither evaluated nutritional status nor calculate the Frailty score of our patients.When study was designed there were no clear parameters specific settle for this diagnosis and a retrospective evaluation was not possible due to lack of complete data.Although recent studies suggest a close relationship between malnourished patients and physical capacity,in order to better evaluate this relationship,another specific protocol must be designed,which was not in accordance with our main objectives.Finally,we did not submit this cohort to a second phase 6MWT to evaluate the relationship between test performance and disease progression.Maybe this analysis could enhance the comprehension about the association of shorter 6MWD and severity of liver disease and its role as a marker of liver decompensation episodes.As we proposed a sectional evaluation of cirrhotic patients with 6MWT,future prospective studies should be able to better answer the previous questions.
CONCLUSION
In summary,6MWT is a very simple,inexpensive,well tolerated,noninvasive test to assess exercise capacity and the result of which is related to MELD and Child scores.The present study showed that 6MWD is an independent predictor of mortality in this population.6MWT is a promising prognostic marker in patients with liver cirrhosis and should be considered as part of liver transplantation evaluation especially in those referred for the liver transplantation team.
ARTICLE HIGHLIGHTS
Research background
Patients with cirrhosis are at risk of exercise limitations due to progressive limitations related to liver dysfunction.Sarcopenia and cirrhotic cardiomyopathy may be possible related factors.The six-minute walking test(6MWT)is a known simple and practical tool used to evaluate patients with cardiopulmonary disease.
Research motivation
In face of limited diagnosis tools focused on exercise capacity,we purposed to evaluate the role of 6MWT in this population.
Research objectives
The aim of our study was to analyzed 6MWT performance in patients with liver cirrhosis to determine if it associates with mortality.
Research methods
We analyzed 6MWT performance in 106 cirrhotic patients.They were evaluated in the outpatient setting with 6MWT and follow up for one year.Hepatic decompensation and mortality were documented.
Research results
This cohort had a mean age of 51 years and 56% male;patients were staged as Child A in 21.7%,B 66%,and C 12.3%.Walk distance inversely correlated with Child scores,and was significantly reduced as Child stages progress.Patients who died(10.4%)showed a shorter mean 6MWD(P= 0.006).Low 6MWD was an independent predictor of mortality(P= 0.01).
Research conclusions
6MWT is a noninvasive inexpensive test whose result is related to Child scores and mortality.
Research perspectives
It is a useful,simple,practical test that can be incorporated into cirrhotic evaluation due to its relation with mortality for closer monitoring and potential early intervention.
ACKNOWLEDGEMENTS
This study was supported by Sao Luis Hospital,D'Or Institute of Research and Education(IDOR),and Fleury Institution.The content is solely the responsibility of the authors and does not necessarily represent the official views of these institutions.
杂志排行

World Journal of Hepatology的其它文章
- Incidence of umbilical vein catheter-associated thrombosis of the portal system:A systematic review and meta-analysis
- Role of endoscopic ultrasound in the field of hepatology:Recent advances and future trends
- Porta-caval fibrous connections—the lesser-known structure of intrahepatic connective-tissue framework:A unified view of liver extracellular matrix
- Promising diagnostic biomarkers of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis:From clinical proteomics to microbiome
- Fatty acid metabolism and acyl-CoA synthetases in the liver-gut axis
- Liver involvement in inflammatory bowel disease:What should the clinician know?