Hepatocellular carcinoma:Understanding molecular mechanisms for defining potential clinical modalities
2021-12-06AbhiramNatuAnjaliSinghSanjayGupta
Abhiram Natu,Anjali Singh,Sanjay Gupta
Abhiram Natu,Anjali Singh,Sanjay Gupta,Epigenetics and Chromatin Biology Group,Gupta Laboratory,Cancer Research Institute,Advanced Centre for Treatment,Research and Education in Cancer,Tata Memorial Centre,Kharghar,Navi Mumbai 410210,Maharashtra,India
Abhiram Natu,Anjali Singh,Sanjay Gupta,Homi Bhabha National Institute,Training School Complex,Anushakti Nagar,Mumbai 400085,Maharashtra,India
Abstract Liver cancer is the sixth most commonly occurring cancer and costs millions of lives per year.The diagnosis of hepatocellular carcinoma(HCC)has relied on scanning techniques and serum-based markers such as α-fetoprotein.These measures have limitations due to their detection limits and asymptomatic conditions during the early stages,resulting in late-stage cancer diagnosis where targeted chemotherapy or systemic treatment with sorafenib is offered.However,the aid of conventional therapy for patients in the advanced stage of HCC has limited outcomes.Thus,it is essential to seek a new treatment strategy and improve the diagnostic techniques to manage the disease.Researchers have used the omics profile of HCC patients for sub-classification of tissues into different groups,which has helped us with prognosis.Despite these efforts,a promising target for treatment has not been identified.The hurdle in this situation is genetic and epigenetic variations in the tumor,leading to disparities in response to treatment.Understanding reversible epigenetic changes along with clinical traits help to define new markers for patient categorization and design personalized therapy.Many clinical trials of inhibitors of epigenetic modifiers(also known as epi-drugs)are in progress.Epi-drugs like azacytidine or belinostat are already approved for other cancer treatments.Furthermore,epigenetic changes have also been observed in drug-resistant HCC tumors.In such cases,combinatorial treatment of epi-drugs with systemic therapy or trans-arterial chemoembolization might re-sensitize resistant cells.
Key Words:Hepatocellular carcinoma;Diagnosis;Treatment;Epigenetics;Epi-drugs;Drug resistance
INTRODUCTION
Liver cancer ranks sixth in cancer incidence globally and accounts for 8.2% of total cancer deaths.The different categories of primary liver cancer are intrahepatic cholangiocarcinoma,hepatocellular carcinoma(HCC),fibrolamellar carcinoma,and hepatoblastoma.These categories have distinct changes in their molecular,histological,and pathological features.HCC alone accounts for 85%-90% of liver cancer cases[1].Almost 2/3 of the population affected by HCC is found in east Asian and south-east Asian countries,making this disease endemic to the region[2].Globally,5-year median survival is below 20% for HCC[3].Major risk factors for HCC include chronic infection with hepatitis B virus and hepatitis C virus,excessive consumption of alcohol,exposure to aflatoxin,physiological state such as non-alcoholic fatty liver disease,and diabetes[4].According to the Barcelona Clinic Cancer Liver Classification(BCLC)algorithm,curative care for HCC involves tumor resection,ablation,and liver transplantation[5].However,this mode of treatment is offered to patients diagnosed in an early stage of the disease.Current research suggests that only 20% of patients are diagnosed in the early stage[6].The lacunae in diagnosis are the unavailability of promising liquid-based biomarkers and detection limits of scanning techniques.Palliative care involving chemo/radiation-based treatment is given to patients with intermediate and advanced stage disease.Following this,70% of patients come back with a relapse of disease and suffer treatment side effects[7,8].
A new approach should be considered to identify diagnostic markers and achieve better therapy response to overcome disease management challenges.Recent advances in the omics field shed light on the pathogenesis and molecular classification of HCC[9-11].The omics approach can help to investigate new markers to improve the therapeutic outcome.Liver carcinogenesis involves both genetic and epigenetic changes.It is impossible to target all genetic variations due to tumor heterogeneity,but gene signature can be manipulated as epigenetic changes are reversible[12].Therefore,epi-drug-based treatment may act as an alternate treatment strategy instead of targeting a single protein or molecular pathway.Epi-drugs can be beneficial not only for the treatment of HCC but also for dealing with cancer resistance[13,14].
This article focuses on the existing approach for diagnosis and treatment in the management of HCC.We also review transcriptomic-based signatures of HCC for patient sub-categorization and their potential implications for diagnosis and therapy.Finally,we propose an epi-drug based treatment strategy based on the epigenetic landscape of HCC.
DIAGNOSIS OF LIVER CANCER
Five standard WHO-approved guidelines include the European Association for the Study of Liver Disease(EASL)[15],American Association for the Study of Liver Diseases(AASLD)[16],Asia-Pacific Association Study of the Liver[17],EASL-EORTC Clinical Practice Guidelines[18],and the updated AASLD guidelines are used for diagnosis of liver cancer.The diagnosis is primarily based on imaging techniques such as ultrasound,computed tomography(CT)scan,and conventional magnetic resonance imaging(MRI)[19].Invasive biopsies are not helpful for the diagnosis of liver tumors.The myriad risk factors involved in biopsy are the local spread of HCC along the needle track and different complications observed in individual patients[20].The early-stage diagnosis of HCC continues to be crucial due to reduced sensitivity and specificity of the diagnostic methods,due to which an ample number of tumors are undetected.The complete list of diagnostic methods with detection limits is shown in Table 1.The various factors responsible for undetectable tumors involve a lack of specific markers and asymptomatic condition during the early stages of HCC[21].Thus,the diagnosis of tumor occurs when it has spread and has reached an advanced stage.

Table 1 Utility and detection limits of existing diagnostic measures of hepatocellular carcinoma
The diagnostic marker used most frequently is serum α-fetoprotein(AFP)[22].AFP level increases beyond 20 ng/mL in more than 70% of patients with HCC.However,AFP elevations are not explicitly associated with HCC as AFP levels from 10-500 ng/mL and even occasionally to 1000 ng/mL may be seen in patients with a high degree of necro-inflammatory activity such as chronic viral hepatitis[23].Chanet al[24]in 2008 have shown that AFP could be better used as a prognostic marker to evaluate response to treatment and detection of recurrence instead of diagnosis[25].Studies have shown that multiple combinations of markers provide more appropriate results in diagnosis than a single marker.A recent study investigated the use of HSP90α(heat shock protein 90)combined with AFP and thymidine kinase 1 to diagnose HCC with more efficiency[26].A study from Beijing YouAn Hospital found that for early diagnosis of HBV-related HCC,a combination of AFP,GPC3,and GP73 had the highest diagnostic value[27].Ghoshet al[28]have shown that the exosome encapsulated microRNAs could be used as a circulating diagnostic marker for HCC with low AFP levels.
Another marker,α-L-fucosidase(AFU),is expressed in liver cirrhosis patients[29].However,limited research is available regarding the utility of AFU in the diagnosis of HCC.In the liver and gallbladder,cell membrane protein 5’-nucleotidase(5’-NT)is released into the blood during hepatic injury or obstruction[30].It has been observed that 5’-NT levels also increase with age and during pregnancy[31].Other markers such as AFP-L3,glypican-3,and des-γ-carboxy prothrombin also show inconsistent data due to low sensitivity and specificity.Hence,the discovery of putative liquid biomarkers is required,which can associate with tumor progression,recurrence,and effectiveness of therapeutic programs.
TREATMENT REGIME AND LIMITATIONS OF CHEMOTHERAPY IN LIVER CANCER
Treatment of HCC is decided based on different stages of tumor detection[32].The BCLC algorithm is widely used for treatment as it considers tumor stage,liver function,performance status,and treatment impact(Figure 1).Early-stage cases are treated with surgery,ablation,or liver transplantation.The patients undergoing surgery showed 70% recurrence within five years[33].The currently used methods for tumor ablation in HCC are percutaneous ethanol injection(PEI)and radiofrequency ablation(RFA).PEI consists of the direct injection of absolute ethanol into HCC nodules[34].RFA is responsive in tumors > 4 cm in size.It involves necrosis of the tumor using a needle tip electrode that reaches temperatures up to 100°C[35].Microwave ablation and irreversible electroporation have shown more promising results than tumor removal with PEI[36].

Figure 1 Treatment modalities for hepatocellular carcinoma based on tumor-node-metastasis staging.HCC:Hepatocellular carcinoma.
Patients with an intermediate stage having a tumor size greater than 5 cm or multinodular HCC with no vascular invasion are treated with trans-arterial chemoembolization(TACE).TACE is used to obstruct the nutrient supply to the tumor using the occlusion of arterial blood vessels[37].Chemotherapeutic drugs such as doxorubicin or cisplatin are given during embolization,allowing prolonged exposure of the drug to tumor cells,resulting in tumor reduction.Yeoet al[38]showed that the overall response rate for doxorubicin-treated patients was 10.5%.Moreover,doxorubicin alone and combined with PIAF had no significant difference in response rate but showed treatment-associated toxicity in patients.Another study showed that combinatorial treatment of fluorouracil,leucovorin,and oxaliplatin failed to improve survival compared to doxorubicin[39].In a multicohort study involving patients with unresectable tumors treated with TACE,overall survival(OS)was approximately 26-40 mo,with only 52% of patients achieving treatment benefits[40,41].In some cases,selective internal radiation therapy is used in patients with intermediate-stage HCC.Intraarterial infusion of radioisotope labeled microspheres is carried out in this modality.Another radiation-based technique known as stereotactic body radiation is used for patients with > 3 cm of the tumor.
Systemic chemotherapy is given for advanced stages of HCC.NCCN Clinical Practice Guidelines in Oncology(NCCN Guidelines)have recommended sorafenib and lenvatinib as first-line systemic therapy for patients with unresectable HCC[42].Brivanib,sunitinib,erlotinib,and regorafenib are other preferred drugs for late-stage HCC treatment.Kudoet al[43]observed that treatment with lenvatinib results in significantly higher OS than sorafenib and improvement in all secondary efficacy endpoints.This trial further results in FDA approval of lenvatinib as the first line of therapy for HCC[43].Sorafenib and sunitinib are protein kinase inhibitors targeting VEGFR,PDGFR,and the Raf kinase pathway.However,a study suggested that sunitinib had an adverse effect in these patients and had no advantage over sorafenib[44].Moreover,sorafenib has been extensively explored in the systemic treatment of advanced stage HCC and combination with TACE,but it provided contradictory results[45,46].Brivanib is an inhibitor of FGF1 and VEGFR2.Phase II clinical trials of brivanib showed the ineffectiveness of the drug compared to sorafenib for improving OS[47,48].The EGFR inhibitor erlotinib or cetuximab was administered in phase II clinical trials of advanced stages of HCC.However,the trial results did not show the anti-tumor effect of cetuximab in HCC patients[49].Interestingly,erlotinib showed a positive response in treatment by increasing OS to 13 mo and a response rate of 59%[50].
As discussed earlier,ablation treatment is possible in less than 40% of patients due to late diagnosis,and only 20% are treated with TACE.For the patients with advanced stages of HCC,treatment modalities are limited to systemic therapy,and response rates are also significantly less due to resistance towards available chemotherapy.Multimodal treatment involving more than one therapeutic drug has also failed in different combinations due to cytotoxicity and poor trial outcomes.Despite the significant research in targeted therapy of HCC management,a promising drug is yet to be identified.Thus,the hunt for combinatorial treatment with different therapeutic agents continues(Figure 2).
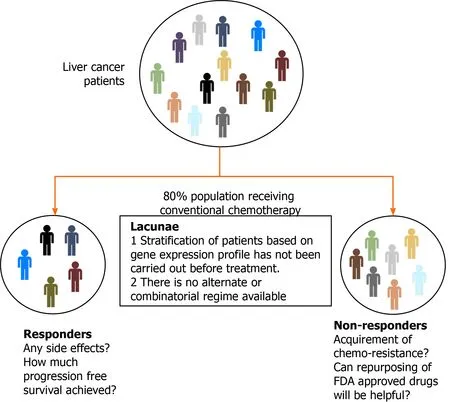
Figure 2 Challenges in the treatment of hepatocellular carcinoma.
MOLECULAR LANDSCAPE OF LIVER TUMOR TISSUE FOR PATIENT STRATIFICATION AND IDENTIFICATION OF ALTERNATE TARGETS
Over the past years,HCC classification has mainly focused on histological analysis of tumor tissues.However,the molecular profile and clinical attributes have a significant impact on the prognosis of the disease,thereby redefining HCC into several subgroups.Boyaultet al[51]published molecular classification systems for HCC composed of 6 groups.The groups were based on mutation profile,disease prognosis,and transcription landscape.The first group included patients with hepatitis B infection and low viral load,increased AFP levels,and high IGF2 expression,whereas the second group included patients with a high viral titer and associated microvascular invasion(MVI)and satellitosis.However,the difference in groups 3 and 4 was based on histological parameters.The third group consisted of poorly differentiated tumors with the worst prognosis;on the other hand,group 4 had well-differentiated tumors.Group 5 and 6 had a low proliferation rate and activated Wnt-signaling pathway.Moreover,pathways are differentially activated in different groups.Another group classified HCC into three groups based on histology and expression analysis of the tumor[52].In this study,the first group showed the presence of satellitosis and MVI.Group 2 had high AFP expression,and the third group consisted of well-differentiated tumors with a low proliferation rate.
Tumor morphology-based classification has been proposed by Murakataet al[53].The nodal status of the tumor was correlated with survival and recurrence of the disease.Moreover,the miRNA profile of HCC patients has been used to classify sorafenib responders[54].c-mycsignaling and EB-1 protein were functionally linked with HCC[55].Similar findings were observed by Leeet al[56]in progenitor-like HCC,which correlated with poor prognosis.In another study,HCC progenitor-like signature consisting of CK-19,Ep-CAM,and CD133 was seen by Wooet al[57].Morofujiet al[58]identified the gene signature of early recurrent HCC,including ERK1,PKG,Apaf1,and Bcl-X.Furthermore,ERK1 and Bcl-X were identified as genes associated with the poor prognosis of HCC[58].However,these studies did not consider the survival status of an individual while proposing subtypes.
Jianget al[59]showed that heterogeneity exists in proteomic profiling of paired early-stage HCC patients.The tumors were segregated into three subtypes:S-I,S-II,and S-III.S-I tumors had increased expression of liver-associated functional proteins.In contrast,S-II and S-III had a more proliferative nature due to overexpression of cellcycle-related proteins.Furthermore,S-III were more aggressive and had a high expression of KRT19 and MMP9,associated with poor prognosis.Gaoet al[60]subgrouped 159 HBV infected patients based on survival,tumor thrombus,and multiomics profile.These sub-groups were classified based on metabolic rewiring,alterations in the microenvironment,and cellular proliferation.Moreover,the study proposed two prognostic markers PYCR2 and ADH1A.
In the past decade,data generated under the TCGA consortium can be used to understand the gene expression profile of patients and obtain correlations with clinical attributes[9].Machine learning algorithms are necessary to analyze such multivariate data.The molecular alterations obtained from the cancer genome atlas liver hepatocellular carcinoma(TCGA-LIHC)cohort(423 patients)can be explored to predict new targets and rationalize the combinatorial therapy.Transcriptome data generated from TCGA-LIHC identified over 13000 differentially expressed genes compared to cutmargin samples,and around 3330 genes correlated with poor survival(Pvalue < 0.05).Furthermore,1730 genes overlapped between the DE gene list and genes correlated with patient survival.The majority of overlapped genes showed more than 30% alteration compared to adjacent normal in this cohort and had a significant association with OS.Patients were categorized into different groups using clustering analysis of gene expression.It was observed that these genes belong to metabolism-related pathways and the cellular proliferation-related family(Figure 3).Deep learning computational framework on the TCGA-LIHC dataset suggested that aggressive subtype has TP53 inactivation with high expression of KRT10,EPCAM,and active AKT,WNT signaling[61].Furthermore,drugs and small molecular compounds are available to target these genes.Schulzeet al[62]reported that potential gene targets have FDA-approved drugs in 28% of liver tumors.Therefore,these genes can be used for prognosis of the disease,and targeting them may improve patient survival.
Gene expression analysis of liver cancer samples can also be utilized to identify new markers for diagnostic purposes.For example,SPP2 is downregulated at the transcript level in HCC.This gene is deregulated in multiple HCC cohorts.Moreover,a stagewise decrease at the transcript level was observed in HCC TCGA data.Also,the downregulation of SPP2 leads to a significant decrease in patient survival(Figure 4).This observation indicates that SPP2 level is associated with normal liver function,and a change in levels can be a measure of liver carcinogenesis.

Figure 3 The cancer genome atlas liver hepatocellular carcinoma data analysis.A:Volcano plot representing differential gene expression between 373 tumor samples and 50 normal samples.Genes colored with red or green are most significantly altered;B:Venn diagram showing overlap between differentially expressed gene list and genes affecting survival of patients upon alteration(survival);C:Normalized expression of top 300 genes associated with overall survival represented using heatmap.Patients with overall survival below the median are marked with a red bar while those above the median are marked with a green bar;D:Altered biological process from overlap gene.Upregulated processes highlighted with red and downregulated processes are depicted as blue;E:Pathways analysis for overlap genes.Deregulated KEGG pathways shown by yellow bars and reactome pathways displayed using green bars.DE:Differentially expressed gene list.
EPI-DRUG BASED TREATMENT FOR IMPROVEMENT OF THERAPEUTIC OUTCOME
The lack of success in disease management can be explained by the multifactorial nature of carcinogenesis involving multiple mutations and global level epigenome alterations[63-65].Epigenetic changes being reversible can be useful to understand the relationship between tumor biology and help in redefining therapeutic response[12].Epigenetics deals with changes in gene expression without change in the DNA sequences[66].Despite all cells having the same DNA sequence,the epigenome decides cell fate regarding differentiation,cell proliferation,and cell death[67,68].The widely studied epigenetic marks are DNA methylation,histone post-translational modifications,and non-coding RNAs.DNA methylation is the most characterized heritable epigenetic mark.This is where a methyl group is transferred onto the cytosine of the CpG di-nucleotide-rich region in DNA by DNMT enzymes[69].DNA methylation plays a vital role in gene inactivation,genomic imprinting,attaining tissue-specific gene expression,and X chromosome inactivation[69].
Similar to DNA modification,histone proteins also undergo post-translational modifications carried out by chromatin modifiers,namely writers,readers,and erasers[70].The well-studied modifications include methylation,acetylation,phosphorylation,and ubiquitination.Histone methylation involves the addition of a methyl group at the lysine or arginine residue on the protruding histone tails.Histone methylation marks can result in repression of transcription or gene activation[71].A typical example of gene suppression is trimethylation at H3K9,and H3K27 whereas methylation at H3K4,H3K36,and H3K79 enhance transcriptional activity[71].Histone acetylation is the transfer of an acetyl group from acetyl CoA.This reaction leads to a change in electrostatic interaction between DNA and histones,resulting in the unwinding of chromatin and enhances gene transcription[72].Histone phosphorylation has an essential role in DNA damage repair,gene transcription,and chromatin condensation during mitosis[72].An illustration of chromatin-associated modifications and the role of epigenetic modifiers is shown in Figure 5.Non-coding RNAs are the transcribed intragenic regions of the DNA that are not translated into proteins.These entities govern gene silencingviaRISC and RNA-induced transcriptional silencing complex formation[73].
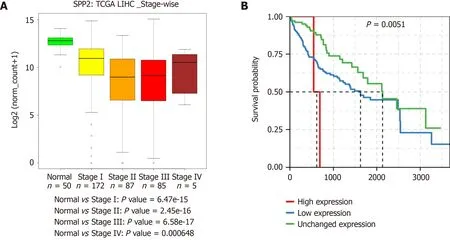
Figure 4 Expression of SPP2 in the cancer genome atlas liver cancer cohort.A:Stage-wise expression of SPP2;B:Patient survival associated with SPP2 expression.TCGA:The cancer genome atlas;LIHC:Liver hepatocellular carcinoma.

Figure 5 Schematic illustration of epigenetic modifications observed in hepatocellular carcinoma and chromatin modifiers targeted by epi-drugs.The figure represents general epigenetic alterations observed in hepatocellular carcinoma and different epigenetic modifiers that can be targeted via small molecule inhibitors.Moreover,DNA and chromatin mediated alterations observed in tumors are highlighted.Changes in DNA methylation and histone posttranslational modifications levels inside normal cells lead to tumor formation.HCC:Hepatocellular carcinoma;HDM:Histone demethylase;HDAC:Histone deacetylase;HMT:Histone methyltransferase;DNMT:DNA methyltransferase;HAT:Histone acetyltransferase.
Different research groups have extensively studied the epigenetic landscape of liver carcinogenesis.Moreover,in the past few years,researchers are investigating the epigenetic basis of chemoresistance in HCC.Lieet al[74]showed that lysine-specific demethylase 1(LSD1)is upregulated in LGR5+ cells contributing to stemness and chemoresistance properties.Mechanistically,LSD1 removes the H3K4 methylation mark from the promoter of genes which inhibit Wnt-signaling.Thus,promoting pathway activation,which is essential for stemness and chemoresistance[74].EpCAM+ liver cancer cells have high expression of chromodomain helicase DNA binding protein(CHD4),a DNA damage response protein.The abundance of CHD4 in liver cancer cells leads to epirubicin resistance[75].Zinc-fingers and homeoboxes 2(ZHX2)is one of the signature proteins which is downregulated in liver CSCs and is associated with tumor progression.It has been found that low expression of ZHX2 is correlated with epigenetic regulation of OCT4,SOX4,and NANOG by H3K36 methylation[76].Oriana Lo Reet al[77]observed that low expression of MacroH2A1 leads to paracrine mediated chemoresistance and imparts CSCs properties to the tumor cells.Another study showed that the regulator of chromosome condensation 2 promotes metastasis and cisplatin resistance in HCC[78].Linget al[79]discovered that USP22 helps to attain chemoresistance by hypoxia-driven p53 mutant tumors.Hypoxia-induced expression of carbonyl reductase 1 leading to chemoresistance in HCC was observed by Taket al[80].H19 long non-coding(lnc)RNA has been shown to sensitize sorafenib or doxorubicin-resistant liver cancer cells[81].The lncRNA CRNDE has been shown to interact with histone methyltransferase to enhance their effect on the inhibition of tumor suppressors and induce resistance in tumor cells[82].
Epigenetic alterations can be targeted by the class of small-molecule inhibitors that specifically inhibit or reverse the changes[83].This class of inhibitors are referred to as epi-drugs.Different research groups have synthesized epi-drugs for all three prominent families of epigenetic modifiers- readers,writers,and erasers.Many epidrugs have cleared pre-clinical trials,and initial phase trials have shown promising results.Few epi-drugs are clinically approved for the treatment of hematological malignancies.In some studies,treatment of solid tumors with an epi-drug helps in sensitizing tumor cells to chemotherapy[84,85].These findings have promoted the research on inhibitors of HDAC,HAT,and DNMTs in combination with chemotherapeutic drugs.In HCC and gastric cancer,the inactive or suppressed state of tumor suppressor genes(TSGs)is mainly attributed to the overexpression of DNMTs and HDACs,leading to heterochromatinization.Reversion of the chromatin state using epi-drugs further leads to activation of TSGs and prevents tumor growth[86].Ongoing pre-clinical trials have been carried out with HDAC and DNMT inhibitors in combination or in comparison with each other to study the anti-tumor effects of the drugs.Guadecitabine(SGI-110),a DNMT inhibitor with sorafenib and oxaliplatin,is in phase II clinical trials for HCC(NCT01752933).Multicenter phase I/II clinical trials using belinostat(HDAC inhibitor)in patients with unresectable HCC showed a tumor stabilization effect[87].One study showed that the combination of panobinostat and sorafenib significantly decreased tumor volume by inducing apoptosis in the tumor[88].A group of researchers observed that the DNMT inhibitor 5’-aza-2’ deoxycytidine and HDAC inhibitor SAHA down-regulated DNMT1,DNMT3a,DNMT3b,and HDAC1 and upregulated GSTP1 and SOCS1 gene expression,which further resulted in inhibition of cell viability and induced apoptosis[89].A detailed list of potential epidrugs is given in Table 2.These findings indicate the ability of epi-drugs,which can restructure the treatment strategy for HCC.
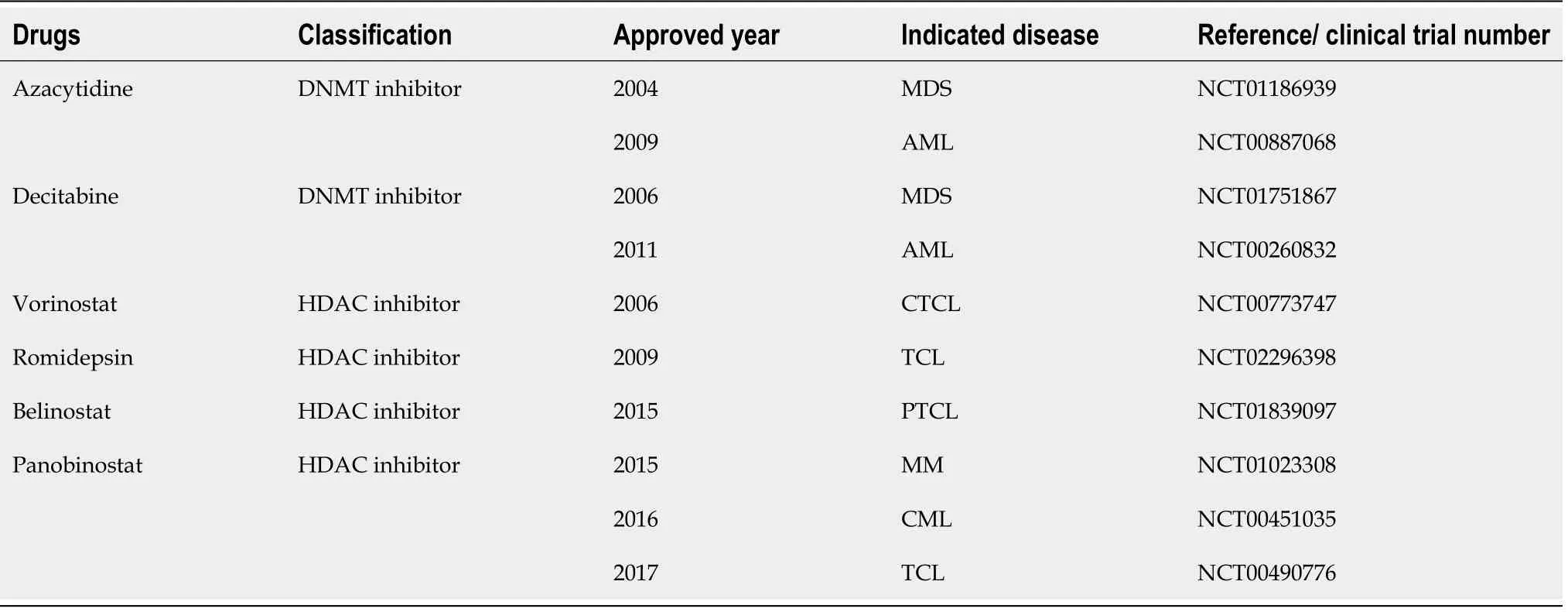
Table 2 List of Food and Drug Administration approved/under trial epi-drugs
Future perspectives
The most effective way of controlling HCC is preventing the disease by spreading knowledge of etiological agents and hepatitis B vaccination.An increase in surveillance is one of the strategies to achieve better survival.This practice helps in the early diagnosis of HCC,monitors progression-free survival,and improves quality of life.Diagnosis of HCC at an early stage is crucial in order to start treatment at the right time and improve patient survival.Due to the reduced sensitivity of current diagnostic techniques,ultrasound scanning of high-risk individuals should be carried out every three months.Although ultrasound is cost-effective compared to MRI and CT scans,there is scope for developing more advanced MRI or CT versions to detect small lesions in the liver.Similarly,there is a need for an appropriate combination of liquid biomarkers used for the investigation of liver carcinogenesis.From a treatment perspective,upon early diagnosis,liver transplantation is preferred over surgical removal or ablation as it is has less than 15% chance of recurrence[90].
The primary cause of treatment failure in cancer is resistance to available chemotherapy,which results in relapse.From heterogeneous tumors,cells respond to treatment differently,and a rare small percentage of cells found in the quiescent G0 state of the cell cycle can escape treatment.These cells are inherently resistant tochemotherapy and involved in relapse.Studies have shown that tumor cells maintain the drug-tolerant stateviachromatin-mediated changes after drug treatment[13].The drug-tolerant persister(DTP)stage is reversible;however,prolonged exposure to chemotherapeutic drugs results in stable drug resistance properties[91-93].DTP cells have non-random differential gene expressions,implicating chromatin-mediated changes leading to hetero-chromatinization of the transposable elements such as LINE1[94].Recent findings suggest that ablation of the DTP cell population with FDAapproved epi-drugs impedes the development of resistance and relapse[13,94].Hangaueret al[95]have shown DTP cells dependence on mesenchymal state and GPX4(lipid hydroperoxide)for survival.Furthermore,inhibition of GPX4 triggers cell death of DTP cellsviathe ferroptosis pathway,indicating ferroptosis is required for the survival of DTP cells[95].Thus,targeting inherently resistant residual cells could be helpful in reducing relapse in patients.However,more research on the identification and characterization of DTP cells is required to choose the appropriate drug combination for treatment purposes.
Targeted drug delivery is the critical factor in improving treatment outcomes and reducing the drug's side effects.Currently,researchers are investigating nanoparticlemediated drug delivery.In addition,modified liposomal formulation showed a successful therapeutic response in HCC due to tumor-directed delivery and low drug load in the system[96].Albumin is also a suitable drug-carrier molecule.An albumintagged drug has more potent effects compared to the drug alone[97].Other materials such as dendrimers,micelles,polysaccharides,and silica are also used as carrier molecules[98-100].Still,the hunt for an effective delivery system continues for targeted delivery.
CONCLUSION
Existing diagnostic methods are inadequate for the early detection of HCC.Similarly,implemented treatment modalities are unsuccessful in improving the survival of patients and result in cytotoxicity in normal cells.The use of credible biomarkers in the prognosis of HCC is essential to reduce mortality due to the disease.In the future,clinicians should focus on patient stratification based on molecular signatures and decide the treatment strategy to achieve maximum therapy outcome.The development of a combinatorial regime consisting of epi-drugs is urgently needed to treat the tumor mass.
ACKNOWLEDGEMENTS
Natu A and Singh A thank ACTREC-TMC for the research fellowship.We thank Gupta laboratory members for valuable discussions and inputs.
杂志排行

World Journal of Hepatology的其它文章
- Incidence of umbilical vein catheter-associated thrombosis of the portal system:A systematic review and meta-analysis
- Role of endoscopic ultrasound in the field of hepatology:Recent advances and future trends
- Porta-caval fibrous connections—the lesser-known structure of intrahepatic connective-tissue framework:A unified view of liver extracellular matrix
- Promising diagnostic biomarkers of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis:From clinical proteomics to microbiome
- Fatty acid metabolism and acyl-CoA synthetases in the liver-gut axis
- Liver involvement in inflammatory bowel disease:What should the clinician know?