Adherence to Mediterranean diet and advanced glycation endproducts in patients with diabetes
2021-11-23MarkoGrahovacMarkoKumricMarinoVilovicDinkoMartinovicAnteKresoTinaTicinovicKurirJosipVrdoljakKarloPrizmicJokoBo
Marko Grahovac,Marko Kumric,Marino Vilovic,Dinko Martinovic,Ante Kreso,Tina Ticinovic Kurir,Josip Vrdoljak,Karlo Prizmic,Joško Božić
Marko Grahovac,Department of Pharmacology,University of Split School of Medicine,Split 21000,Croatia
Marko Kumric,Marino Vilovic,Dinko Martinovic,Ante Kreso,Tina Ticinovic Kurir,Josip Vrdoljak,Karlo Prizmic,Joško Božić,Department of Pathophysiology,University of Split School of Medicine,Split 21000,Croatia
Tina Ticinovic Kurir,Department of Endocrinology,University Hospital of Split,Split 21000,Croatia
Abstract BACKGROUND In recent years,American Diabetes Association started to strongly advocate the Mediterranean diet(MD)over other diets in patients with diabetes mellitus(DM)because of its beneficial effects on glycemic control and cardiovascular(CV)risk factors.Tissue levels of advanced glycation endproducts(AGEs)emerged as an indicator of CV risk in DM.Skin biopsy being invasive,the use of AGE Reader has been shown to reflect tissue AGEs reliably.AIM To examine the association between adherence to MD and AGEs in patients with DM type II.METHODS This cross-sectional study was conducted on 273 patients with DM type II.A survey questionnaire was composed of 3 separate sections.The first part of the questionnaire included general data and the habits of the participants.The second part aimed to assess the basic parameters of participants’ diseases and associated conditions.The third part of the questionnaire was the Croatian version of the 14-item MD service score(MDSS).AGEs levels and associated CV risk were measured using AGE Reader(DiagnOptics Technologies BV,Groningen,The Netherlands).RESULTSA total of 27(9.9%)patients fulfilled criteria for adherence to MD,with a median score of 8.0(6.0-10.0).Patients with none/limited CV risk had significantly higher percentage of MD adherence in comparison to patients with increased/definite CV risk(15.2% vs 6.9%,P = 0.028),as well as better adherence to guidelines for nuts(23.2% vs 12.6%,P = 0.023)and legumes(40.4% vs 25.9%,P = 0.013)consumption.Higher number of patients with glycated hemoglobin(HbA1c)< 7% adhered to MD when compared to patients with HbA1c > 7%(14.9% vs 7.3%,P = 0.045).Moreover,those patients followed the MDSS guidelines for eggs(33.0% vs 46.8%,P = 0.025)and wine(15.6% vs 29.8%,P = 0.006)consumption more frequently.MDSS score had significant positive correlation with disease duration(r = 0.179,P = 0.003)and negative correlation with body mass index(BMI)values(r= -0.159,P = 0.008).In the multiple linear regression model,BMI(β ± SE,-0.09 ± 0.04,P = 0.037)and disease duration(β ± SE,0.07 ± 0.02,P< 0.001)remained significant independent correlates of the MDSS score.Patients with HbA1c > 7% think that educational programs on nutrition would be useful for patients in significantly more cases than patients with HbA1c < 7%(98.9% vs 92.6%,P = 0.009).CONCLUSION Although adherence to MD was very low among people with diabetes,we demonstrated that adherence to MD is greater in patients with lower CV risk,longer disease duration,and well-controlled glycaemia.
Key Words:Mediterranean diet;Cardiovascular disease;Diabetes mellitus;Advanced glycation endproducts;Dietary habits;Atherosclerosis
INTRODUCTION
Diabetes mellitus(DM)is a group of chronic disorders of carbohydrate,fat and protein metabolism caused by defects of insulin secretion,action,or both[1].Among two of the most prominent types,DM type II accounts for 90%-95% of people with DM[2].Around 462 million individuals worldwide are affected by DM type II,corresponding to 6.28% of the world's population[3].The rising incidence is even more staggering,as recent estimates point that 1 in 3 people in the world will have DM type II by 2050[4].Even though immense efforts in terms of public health measures were made,developed regions,such as Western Europe and the United States,show considerably higher prevalence rates of DM in contrast to Third World countries[4].This highlights the implication of socio-economic development and concomitant lifestyle in the pathophysiology of DM.Hence,lifestyle changes,particularly diet,seem to be an essential cornerstone of DM management.
In fact,according to the American Diabetes Association(ADA),nutritional therapy is of particular importance in the treatment of DM[5].Lately,ADA strongly advocates the Mediterranean diet(MD)over other diets because of its beneficial effects on glycaemic control and cardiovascular(CV)risk factors[5].MD is a characteristic dietary pattern established in the coastal areas of the Mediterranean basin[6].By definition,MD consists of three to nine servings of vegetables,one to thirteen servings of cereals,half to two servings of fruits,and up to eight servings of olive oil a day[6].The recommended total fat intake is about 37%,18% of which are monounsaturated and 9% saturated fats,whereas the recommended fibre intake is 33 gperday[6].Furthermore,moderate consumption of red wine,especially during meals,and rare consumption of red meat are also important factors of this diet[6-8].
Pathophysiology of DM includes a myriad of detrimental molecular processes.Perhaps the critical effector arm of damage in the setting of DM is hyperglycaemiainduced overproduction of reactive oxygen species(ROS).Among multiple other effects,ROS production results in the up-regulated formation of intracellular advanced glycation endproducts(AGEs)[9].AGEs are typically accumulated slowly in the human body during life,mostly in tissues with slow metabolism[10].This process is accelerated in some diseases such as DM,renal failure,and various CV diseases[10].Previous studies have shown that the values of AGEs are elevated in patients with DM and are at least in part the cause of DM-associated CV complications[11,12].The receptors for advanced glycation endproducts(RAGEs)are found on inflammatory cells(T-lymphocytes and macrophages),endothelial cells and vascular smooth muscle cells.The binding of AGEs to RAGEs stimulates the release of proinflammatory cytokines and growth factors from macrophages,the formation of ROS from the endothelium,the procoagulant action of endothelium and macrophages,as well as interconnection of extracellular matrix proteins[10].Previous studies have clearly shown that AGE quantity measured from skin tissue is a solid and independent predictor of CV complications,as well as CV morbidity and mortality in DM[13-15].Unlike skin biopsy,AGE Reader recently emerged as a non-invasive yet reliable instrument for the measurement of AGEs tissue levels[14].In addition,it has been shown that the AGEs reader has a significant additional value in determining the degree of CV risk in patients with DM[14,15].In a study by Liet al[16],it was demonstrated that patients who had higher values of AGEs also had higher values of glycated hemoglobin(HbA1c),whereas the results of a cross-sectional study by Coupp éet al[17]show that different long-term exercise regimens can slow down the normal process of AGEs accumulation[16,17].
Although MD and AGEs levels have already been investigated in patients with DM,there is scarce information regarding their mutual interconnections.Hence,the main aim of this study was to examine the association between adherence to the MD and CV risk/AGEs skin levels,in patients with DM type II[18,19].In addition,we examined the association of anthropometric characteristics,glycaemic control,and physical activity with AGEs levels in the same group of patients.Finally,we examined dietary attitudes and characteristics of the studied population according to DM management.In this study,we hypothesized that patients with DM type II who adhere more to the MD would have lower AGEs skin levels,reflecting lower CV risk.
MATERIALS AND METHODS
Study design and ethical considerations
This study was performed at the Regional Center for Diabetes,Endocrinology and Metabolic Diseases of the University of Split School of Medicine from 1 March 2019 to 1 June 2019.The study was approved by the Ethics Committee of the University of Split School of Medicine.The researchers informed the participants about the procedures and purpose of the study,after which all involved participants signed informed consent.
Subjects
A total of 273 patients(137 men and 136 women)with DM type II participated in this study.DM type II was diagnosed according to the criteria of the ADA[1].All included participants were treated at the Regional Center for Diabetes,Endocrinology and Metabolic Diseases of the University Hospital of Split,and were interviewed during regular check-ups by a diabetologist.The inclusion criteria was that DM type II is diagnosed for at least a year.On the other hand,newly diagnosed DM type II,DM type I and other types of diabetes were excluded from the study.For the present study,we initially screened 347 patients.Nineteen patients were excluded because their DM type II diagnosis was established in the past year,37 patients were excluded because they had DM type I,whereas 10 patients were excluded because they had other types of DM.Finally,among 281 eligible patients,eight refused to participate in the study,yielding an overall acceptance rate of 97%.For the purpose of this study,we performed sample size analysis using MedCalc software.We used an estimated difference in the proportion of the adherence to MD of 0.1,with α error set at 0.05 and study power of 90%.The calculated sample size was 158 participants.To ensure additional power to the study,we collected a substantially larger sample of diabetes patients.Relevant clinical information on each participant was collected by taking anamnesis and checking their medical documentation.Participants also completed a survey on their life habits and the MD service score(MDSS)questionnaire to assess adherence to the MD.Finally,all participants were subjected to measurements of relevant anthropometric features and AGEs value using AGEs reader.
Anthropometric measurements
Participants were subjected to the following measurements of anthropometric features:Body weight and height,neck,waist and hip circumference.A calibrated medical scale with an altimeter(Seca,Birmingham,United Kingdom)was used to measure body weight and height.Body mass index(BMI)was calculated by dividing the value of body weight(kg)by the square of the value of body height(m2).Waist circumference was measured at the upright standing position at the midline level between the bottom of the costal arch in the mid-axillary line and the apex of the iliac ridges.In the same position,the hip circumference was measured at the level of the largest circumference of the gluteal muscles,above the line connecting the large trochanters of the femur.The waist-to-hip ratio is determined by dividing the waist circumference(cm)by the hip circumference(cm).Neck circumference was measured at the midway of the neck,between the mid-cervical spine and mid anterior neck.All circumferences were measured using the same centimetre ribbon with 0.5 cm precision.
Survey
After an extensive literature review,a survey questionnaire that included 27 items divided into three main parts was compiled.
The first part consisted of 7 items that included general patients’ information and basic parameters of their disease.The questions included were about:Gender,year of birth,physical activity,smoking status,year of DM diagnosis,last HbA1c levels,and type of DM therapy.
The second part of the questionnaire was MDSS,a useful instrument often used to measure overall diet quality according to the principles of the MD[20].MDSS is based on the recommended intake of 14 food groups in the Mediterranean food pyramid[18].While scoring the questionnaire,three points were awarded to those participants who met the appropriate recommended frequency of consumption of the following food groups:Fruits,vegetables,cereals(bread,pasta,rice),and olive oil.Two points were given to those who met the appropriate recommended frequency of dairy products and nuts consumption.Finally,one point was given to those who met the appropriate recommended frequency of consumption of potatoes,legumes,fish,eggs,red meat,white meat,sweets and wine.A score of zero was given if the number of servings of a particular food did not meet the MD recommendations.With this scoring,most points(3 points)are earned by consuming enough food that should be an integral part of every meal in the MD diet.The rest of the points are awarded for foods recommended for intake on a daily(2 points)or weekly(1 point)basis.The overall score can range from 0 to 24 points.A score of over 13.5 points is considered as good adherence to MD principles.The reliability and validity of the Croatian version of the 14-item MDSS questionnaire in assessment of adherence to MD was evaluated by Marendićet al[18].
Finally,the third questionnaire part included 6 items that investigated the dietary attitudes of the investigated population.All of the included statements could be answered with “yes” or “no “.Statements were about the source of information about diet,nutritionist support,getting diet information off the internet,the importance of diet in managing personal health problems,usefulness,and attendance of diet-related educational programs.
Measurement of AGEs
AGEs value and associated CV risk were measured using AGE Reader(DiagnOptics Technologies BV,Groningen,The Netherlands).This is a non-invasive desktop device that uses the characteristic fluorescence of certain AGEs to calculate the level of accumulated AGEs in the skin.This method was confirmed to be firmly consistent with the measurement of the accumulation of AGEs in a skin biopsy sample,taken from the same site where the autofluorescence reading was performed[13].
Participants were briefly introduced to the method of measurement.There was no risk for our participants during this measurement.They were then asked to place their right forearm on the device,which is a standard and practical measuring point on the body for calculating the autofluorescence of certain AGEs from the skin[13].A series of three consecutive measurements were performed.The results were summed and divided to obtain the mean,which was later used in the analysis.Based on the association of the obtained result with the age of the subjects,a value that classifies participants into one of the four groups(none,limited,increased,definite)depending on their CV risk was calculated.We further stratified these groups into two CV risk groups.The first group included patients with none and limited CV risk,whereas the second included patients with increased and definite CV risk.Finally,this method is observer-independent and has an intrapersonal coefficient of variation of less than 5%[14].
Statistical analysis
Statistical analysis was performed with MedCalc package(version 19.1.2,MedCalc Software,Ostend,Belgium).Categorical variables were presented as whole numbers and percentages,while differences were evaluated with the chi-squared test and Fisher’s exact test.Continuous variables were presented as mean and standard deviation or median and interquartile range,according to the normality of data distribution analysis performed with D'Agostino-Pearson test.Accordingly,differences between groups were evaluated with Mann Whitney U-test and t-test for independent samples.Furthermore,the correlation between MDSS score and other selected variables was tested with Spearman’s correlation coefficient,while independent factors associated with MDSS scores were evaluated with multiple linear regression analysis.For this purpose,enter algorithm was used,with a report of unstandardized beta coefficients(β),t-values,standard errors(SE),and P-values.The selected model had all assumptions in using multiple regression satisfied.Statistical significance was set atP< 0.05.
RESULTS
The study enrolled a total of 273 DM type II patients,with overall AGEs levels of 3.0(2.6-3.5).Significantly higher values of AGEs were found in men when compared with women[3.1(2.7-3.7)vs2.9(2.5-3.3),P< 0.001],while HbA1c values were without significant difference between genders[7.3(6.7-8.8)%vs7.5(6.7-8.8)%,P= 0.475].According to AGEs levels,patients were divided into none/limited CV risk group(n= 99)and increased/definite CV group(n= 174).According to these groups,increased CV risk group had significantly higher percentage of male patients(55.2%vs41.4%,P= 0.029),and higher levels of HbA1c[7.65(6.8-8.8)%vs7.2(6.5-8.5)%,P= 0.041].Other baseline parameters according to the CV risk can be found in Table 1.
According to the MDSS questionnaire,a total of 27(9.9%)patients fulfilled criteria for adherence to MD,with a median score of 8.0(6.0-10.0).Patients with none/limited CV risk had significantly higher percentage of those who adhered to MD in comparison to patients with increased/definite CV risk(15.2%vs6.9%,P= 0.028).In addition,those participants who followed the MDSS guidelines for nuts(23.2%vs12.6%,P= 0.023)and legumes(40.4%vs25.9%,P= 0.013)consumption also had significantly higher adherence(Table 2).Furthermore,analysis of MDSS according to DM type II management has shown that significantly higher number of patients with HbA1c < 7 % adhere to MD when compared to patients with HbA1c > 7 %(14.9%vs7.3%,P= 0.045).Moreover,those patients follow the guidelines for eggs(33.0%vs46.8%,P= 0.025)and wine(15.6%vs29.8%,P= 0.006)consumption more frequently(Table 3).
According to gender,women followed the guidelines for red meat consumption more frequently than men(34.3%vs58.8%,P< 0.001),while men had better follow of guidelines for cereals(70.8%vs55.9%,P= 0.011)and wine(33.6%vs7.4%,P< 0.001)consumption.Adherence to all food groups in MDSS according to gender can be found in Table 4.

Table 1 Baseline parameters analysis according to cardiovascular risk groups derived from advanced glycation endproducts result
Further analyses have shown that MDSS score has a significant positive correlation with disease duration(r= 0.179,P= 0.003)and negative correlation with BMI values(r= -0.159,P= 0.008)(Table 5).Moreover,in the multiple linear regression model,BMI(β ± SE,-0.09 ± 0.04,P= 0.037)and disease duration(β ± SE,0.07 ± 0.02,P< 0.001)remained significant independent correlates of MDSS score(Table 6).
Finally,attitudes regarding diet and diet behaviours were analysed.Most of the patients that get diet information from a physician(96.3%),think that a better and more controlled diet could reduce their health problems(88.6%)and would visit educational programs if they existed(81.7%).Furthermore,advice from a nutritionist was received in 16.8%of cases,while 17.9% of patients have informed themselves on the Internet regarding diet in diabetes.According to DM management,patients with worse DM control think that educational programs on nutrition would be helpful,in significantly more cases in comparison to patients with better control of DM(98.9%vs92.6%,P= 0.009).Dietary attitudes of the studied population according to DM management can be seen in Table 7.
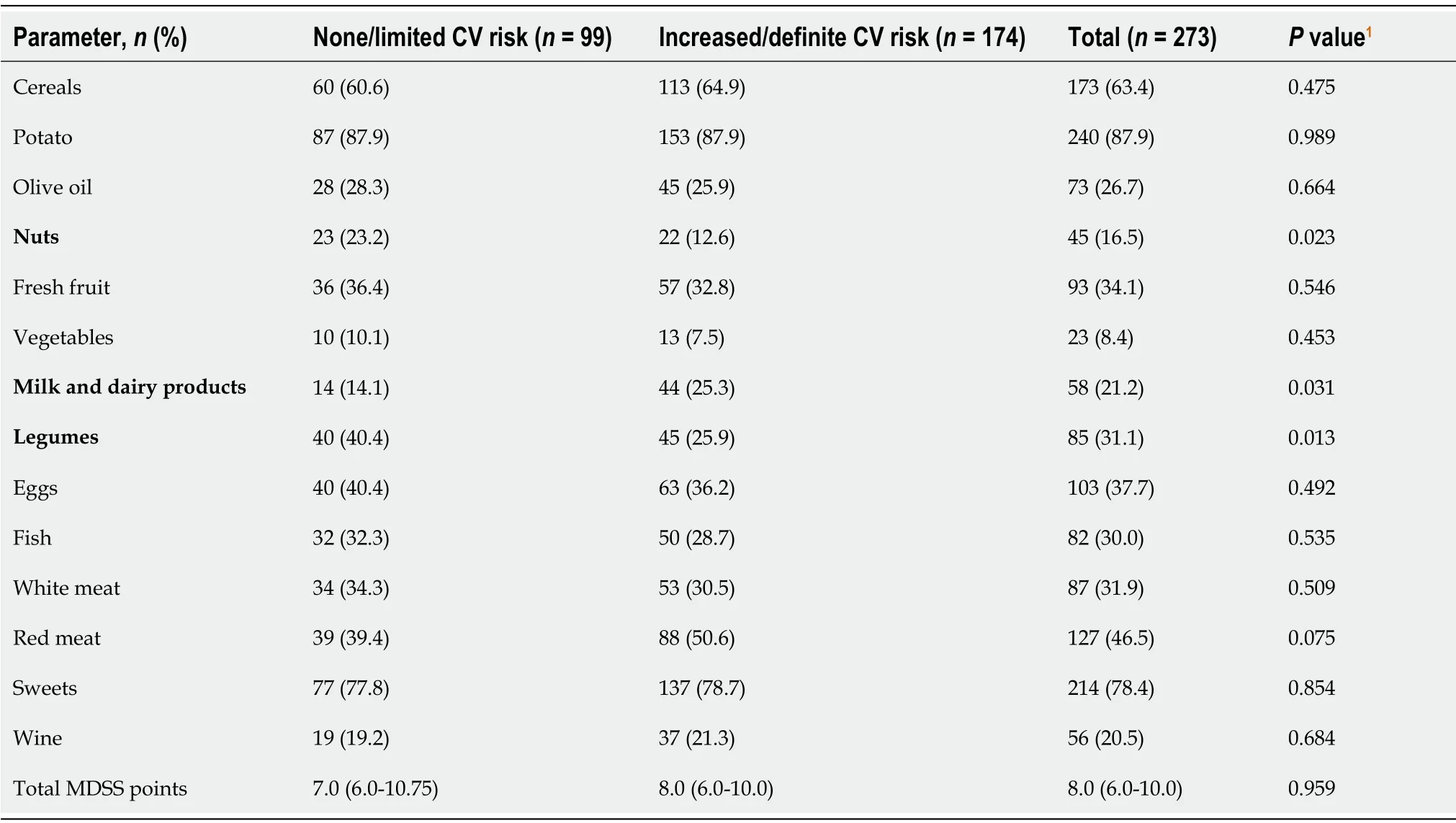
Table 2 Adherence to individual food groups and total Mediterranean diet guidelines according to cardiovascular risk groups derived from advanced glycation endproducts levels
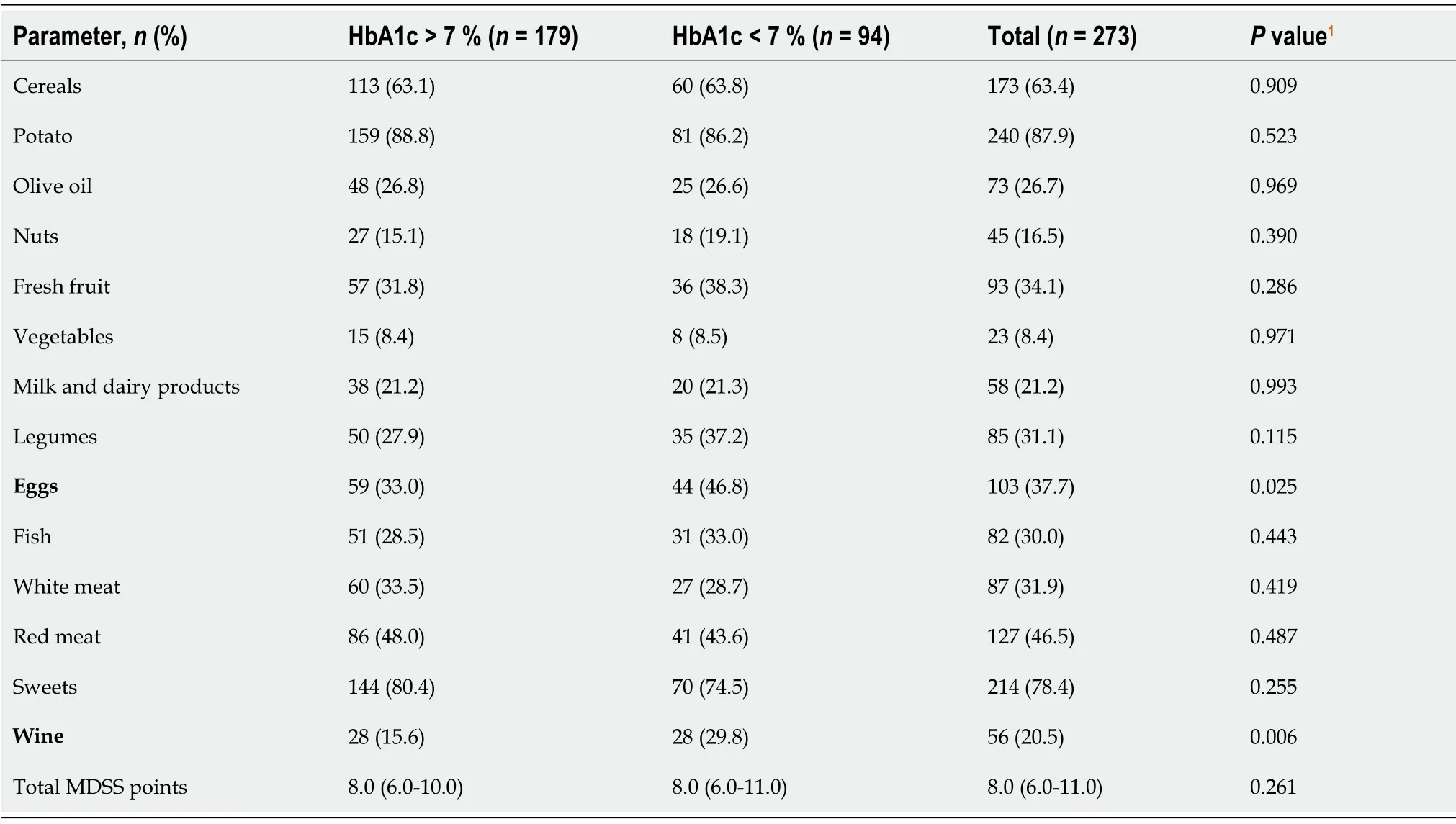
Table 3 Adherence to individual food groups and total Mediterranean diet guidelines according to diabetes management
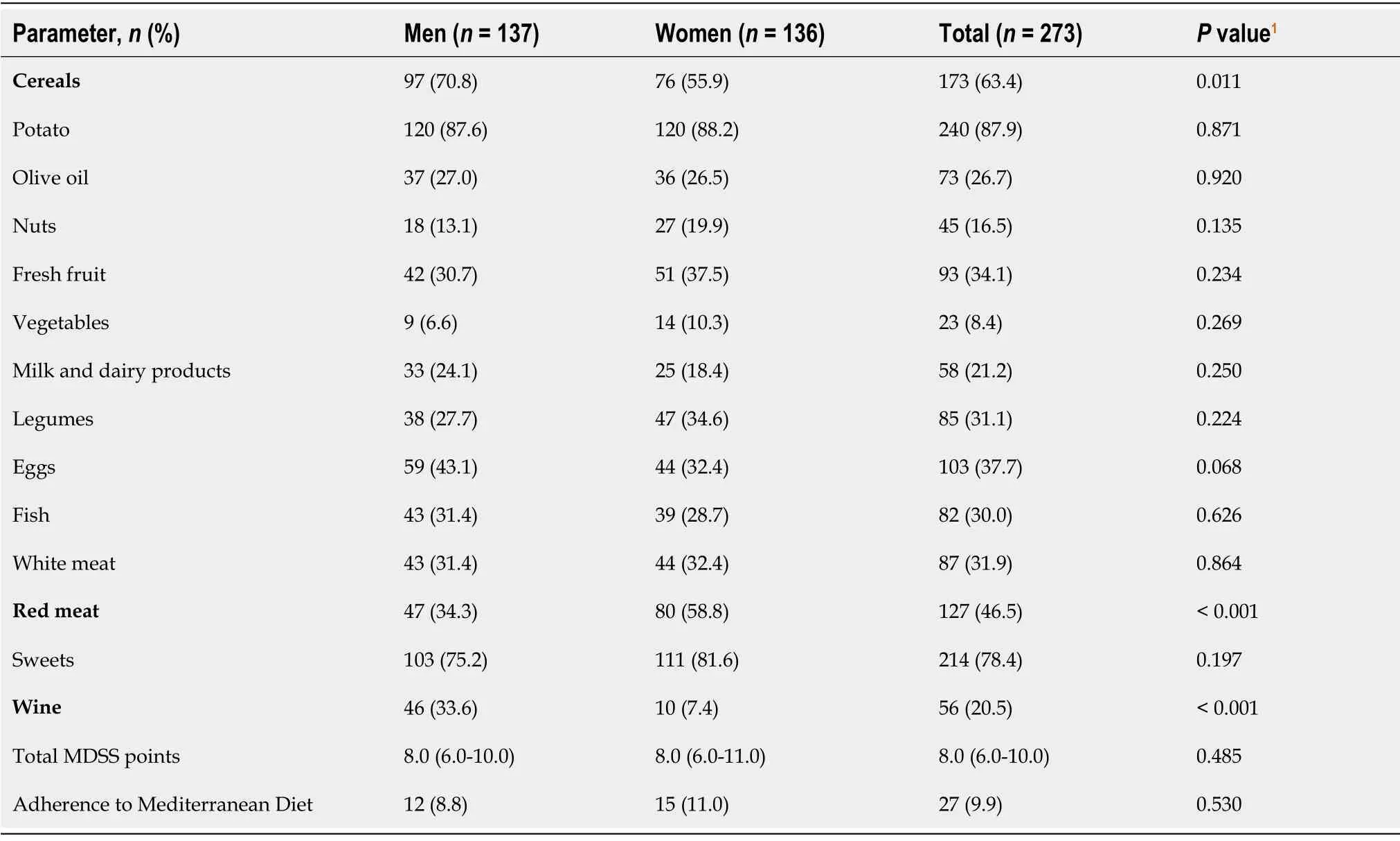
Table 4 Adherence to individual food groups and total Mediterranean diet guidelines according to gender
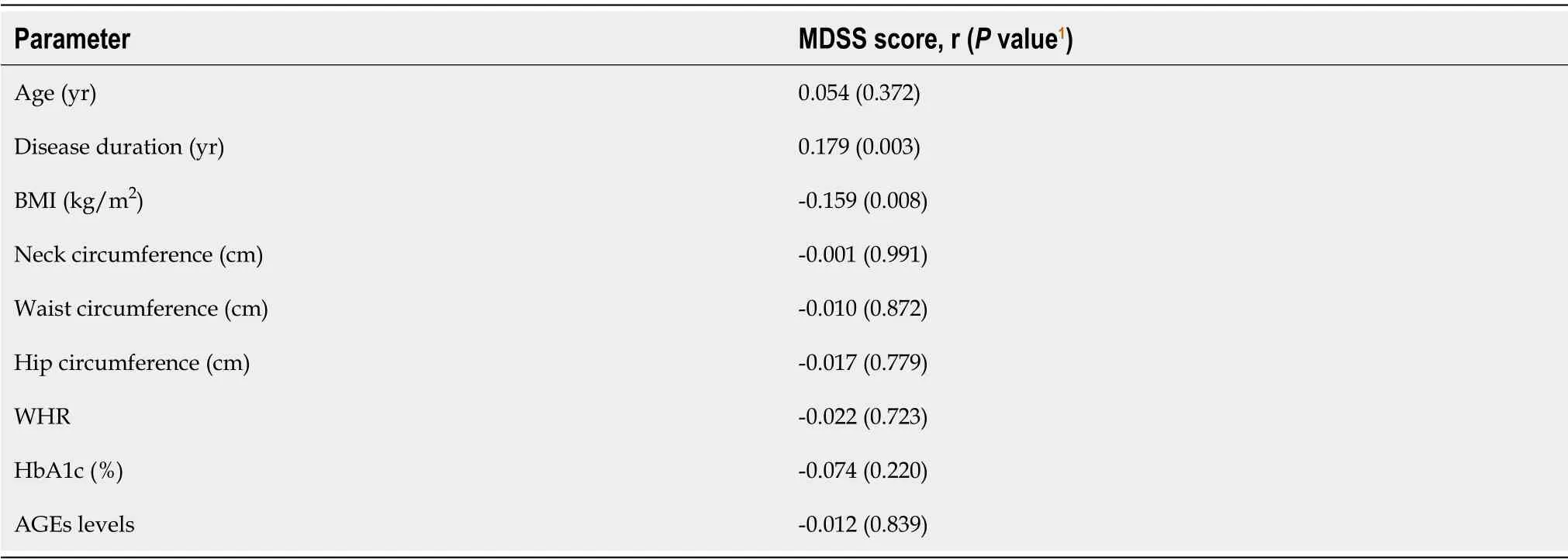
Table 5 Correlation of Mediterranean diet serving score with selected parameters in study population(n= 273)
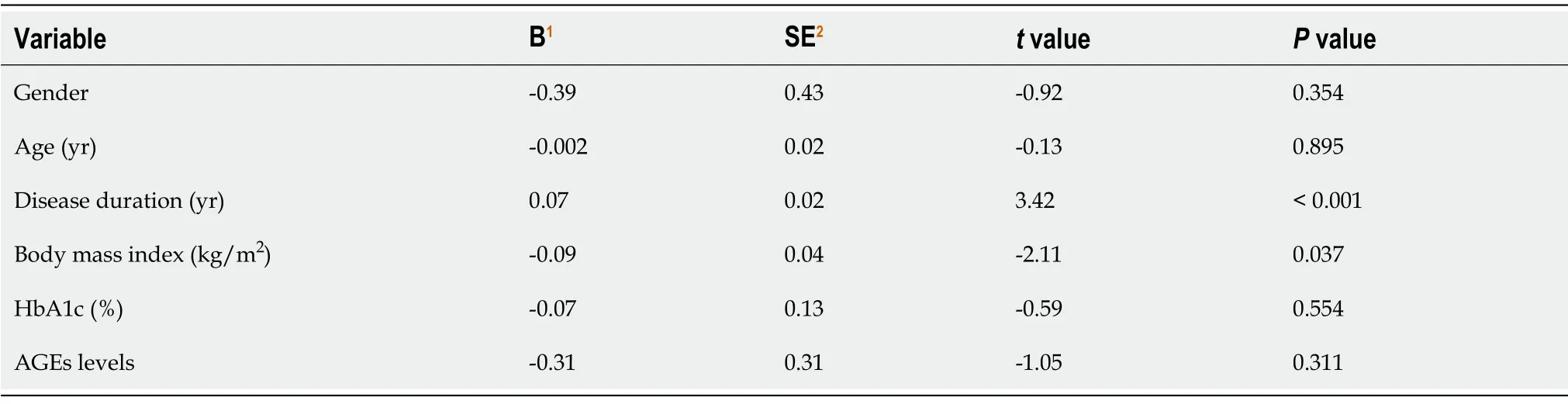
Table 6 Multiple linear regression model of independent predictors for Mediterranean diet service score
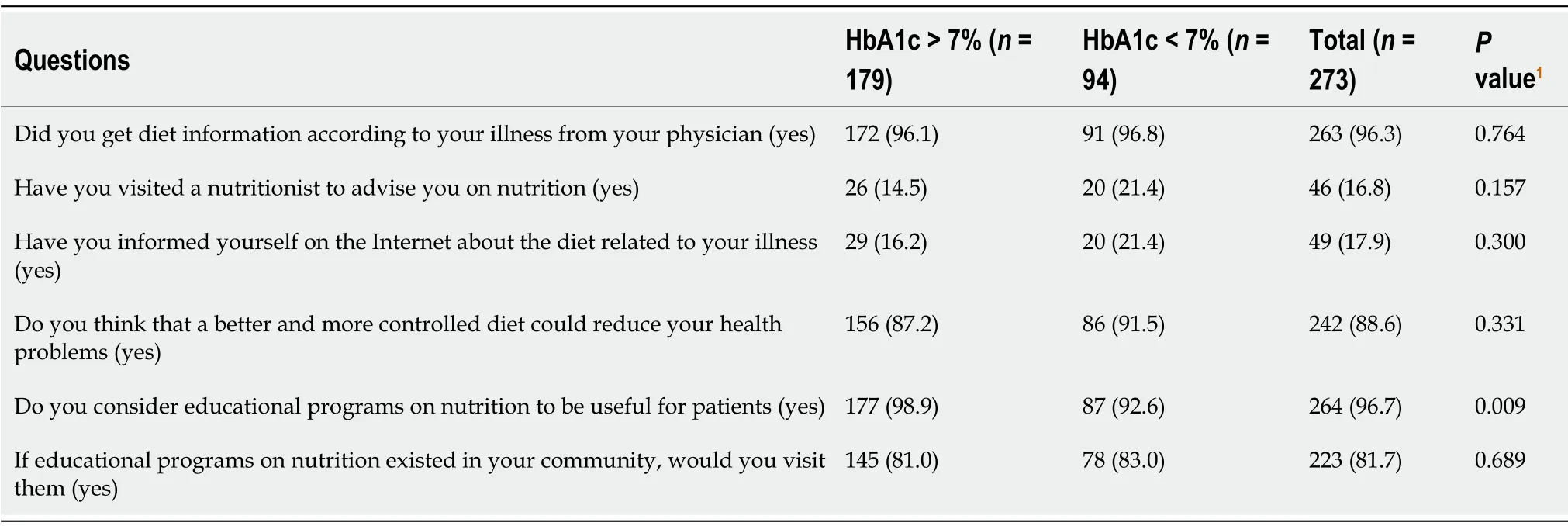
Table 7 Dietary attitudes of studied population according to diabetes management
DISCUSSION
In the present cross-sectional study,we demonstrated that DM type II patients with no or limited CV risk adhere more to the MD than patients with either increased or definite CV risk.In line with this,significantly more patients with none or limited CV risk followed the recommended use of nuts and legumes.Furthermore,we showed that the subgroup of DM type II patients with lower HbA1c levels(< 7%)adheres better to the MD than the subgroup of patients with higher HbA1c levels(> 7%),markedly in terms of following the recommended use of wine and eggs.In addition,these subgroups mainly did not differ in dietary attitudes.Interestingly,MDSS correlated positively with disease duration and negatively with BMI,which was further confirmed in a multiple linear regression model.Finally,certain gender differences in diet adherence were also observed,as women followed guidelines for red meat consumption more frequently than men,whereas it was vice versa with respect to guidelines for cereals and wine.
Our results regarding the association between MD adherence and CV risk are in concordance with the available studies.Namely,it has so far been well established that adherence to MD improves CV outcomes[21-24].Among an array of the conducted studies,the PREDIMED(PREvención con DIeta MEDiterránea)trial should be specially addressed,as insights from it provided a large body of evidence on the association between MD and diverse health outcomes[25].The PREDIMED is a multicentre,randomized,primary prevention trial that included 7447 participants aiming to assess the long-term effects of MD on the occurrence of CV events.The trial clearly showed a 30% relative risk reduction in CV event incidence,while additionally calculating that,in a 5-year follow-up,in a hypothetic cohort of 1000 people following the MD,13 CV events can be prevented.Notably,accounting for the advanced age of the study participants,it has been concluded that it is never too late to improve dietary regiments in terms of CV health.The main advantage of the PREDIMED trial was a continuous assessment of MD adherence,unlike most of the other follow-up studies in which dietary habits were only measured at the commencement of the study.However,it is important to point out that no effect on all-cause mortality was apparent in this trial,unlike other studies conducted on this topic[26-28].Pathophysiological mechanisms by which MD exhibits the above-noted protective effects on the CV system are diverse[29].Although not completely elucidated,the richness of MD nutrients in anti-oxidant and anti-inflammatory molecules is likely to be relevant[30,31].Nutrients can either have intrinsic anti-oxidant capacity or modulate gene and protein expression.Available studies suggest that MD exerts protective effects on the expression of several proatherogenic genes,resulting in modulation of vascular inflammation,thrombosis,and foam-cell formation[32-34].In this sense,legumes,for which we demonstrated that patients with lower CV risk have a higher adherence,contain a lot of phytochemicals endowed with useful biological activities[35,36].Phytochemicals were shown to have prominent antioxidant activity,improve endothelial function by increasing nitric oxide bioavailability and prevent athero-sclerosis progression by inhibition of low-density lipoprotein oxidation[37,38].Accordingly,nutrients in nuts,for which we demonstrated better adherence among low-risk CV subgroup as well,are also associated with multiple molecular pathways which grant their beneficial CV effects.Namely,randomized trials have proven that nuts consumption is associated with attenuation of inflammation and oxidative stress burden,improvement in endothelial function and lipid status,as well as in insulin resistance[39,40].
The rationale for using AGE Reader in CV risk stratification is substantiated by multiple evidence[41].AGEs serum or plasma levels do not reflect levels of AGEs in tissues,owing to the high protein turnover rate in the circulation[42].Conversely,AGE Reader reliably reflects AGEs tissue levels obtained using skin biopsy by utilizing fluorescent properties that several AGEs possess[43].Furthermore,multiple studies indicate that accelerated accumulation of AGEs was proportionally associated with higher CV risk,thus justifying the use of AGE in this setting[13,14,15,44].
Effects of MD adherence on glycaemic control in DM type II were thoroughly reviewed by Espositoet al[45].Multiple authors provided evidence which points to an inverse association between MD and indices of glucose homeostasis in the general population,the elderly,and high-risk patients[46-48].Among five conducted RCTs that evaluated the effects of MD on glycaemic control in DM type II[49-53],only one trial showed no difference in HbA1c levels between the control group[49].Namely,Shaiet al[49]compared three weight-loss diets in 322 moderately obese patients,46 of which suffered from DM type II,and demonstrated no difference in HbA1c decrease between the groups assigned to the MD as compared with the low-fat diet,however,a significant decrease in fasting glucose concentration was found in the MD cohort.Our results seem to be in line with findings from the aforementioned studies.In addition,more optimal adherence for wine and eggs in the subgroup with lower HbA1c was observed in the present study.This observation could be explained by the fact that wine and eggs were both shown to exert favourable effects on the metabolic profile in patients with DM[54,55].
Although our findings that adherence to MD positively correlates with disease duration seem reasonable,conflicts with some of the available data.Austinet al[56]demonstrated that DM type I duration is indicative of poorer dietary self-care in adolescents[56].Authors attributed this observation to contextual and motivational factors as posited by Self-Determination Theory.However,owing to the significant age difference and concomitant differences in psychological features between ours andAustinet al[56]’s study participants,their findings could hardly be extrapolated to the current study.On the other hand,multiple studies conducted on populations similar to the population present in this study also demonstrated opposite results.Most authors agree that strict dietary habits fade over time,as DM patients are under the constant threat of severe diabetic complications despite being adherent to self-care behaviours,which results in burnout[57,58].As overall MD adherence was low in the current,but in other studies as well,a search for novel educational techniques is warranted[59-61].This is also recognized by study participants(97%),markedly in those with higher HbA1c levels.These results may be explained by multiple factors.In both our and other studies,the first and probably the main culprit for low MD adherence are overall high prices for dietary products of which MD is comprised.Furthermore,the westernization of society has also impacted the dietary preferences of the population,shifting to high-sugar,low-fibre processed food.Finally,the knowledge concerning healthy dietary habits in our population is generally low,even among general practitioners[62,63].Given that only 16% of our participants underwent nutritionist evaluation despite that average disease duration was 12 years,this could be a promising niche for diet improvement in patients with DM,as demonstrated by multiple authors[64,65].Conversely,a negative correlation was found between MD adherence and BMI.These results are expected,as MD adherence was previously shown to participate in weight reduction[66,67].In addition,patients who are more motivated for dietary self-care are more prone to weight loss[67].
The observed decrease in consumption of red meat in female participants and increased consumption of wine and cereals among men is in line with the available data[66].Multiple authors suggest that gender differences in adherence to certain food groups could be explained by psychological dissimilarities between men and women,more frequent veganism in woman populations,and reduced accessibility of meat to women[68,69].Results from the present study imply that patients with higher AGEs levels and concomitantly higher CV risk are less eager to remain physically active.The obtained results are in concordant with the available data,as most studies demonstrated that physical inactivity is associated with high levels of AGEs and other predictors of CV risk[70,71].Interestingly,in a study by Rodrigueset al[72],the authors demonstrated that low AGEs levels in patients with human immunodeficiency virus could be restored to normal values by exercising in just a few months[72].
Our study bears several limitations.Firstly,the cross-sectional design of the study which prevents us from making any causal inferences.Secondly,in the questionnaire,we have relied on the participant’s recall memory,therefore,the answers are susceptible to subjectivity and recall bias.Finally,although considered reliable,we must bear in mind that AGE Reader has many different endogenous and exogenous components which may influence measurement of the AGEs.
CONCLUSION
In summary,this cross-sectional study brought further evidence concerning the association between AGE tissue levels and adherence to MD using a validated MDSS questionnaire.In line with this,we demonstrated that adherence to MD is very low in patients with DM type II,especially in those with poorly controlled glycaemia.Nevertheless,survey results indicate that patients seem to realize the importance of diet in DM management.Furthermore,it has been observed that dietary preferences are influenced by gender,women followed guidelines for red meat consumption more frequently than men,whereas it was vice versa in guidelines for cereals and wine.Finally,we showed that DM duration independently predicted better adherence to MD,whereas BMI predicted poorer MD adherence.
ARTICLE HIGHLIGHTS
Research background
In recent years,major diabetic organizations started to strongly advocate the use of the Mediterranean diet(MD)over other diets in patients with diabetes mellitus(DM)because of its beneficial effects on glycaemic control and cardiovascular(CV)risk factors.Evidence suggests that CV risk may be assessed using tissue levels of advanced glycation endproducts(AGEs)in patients with DM.
Research motivation
As DM prevalence is constantly rising in well-developed countries,there is an urgent need to mitigate the poor outcomes of this disease.Regarding the importance of diet in this setting,we endeavoured to bring further evidence with respect to the benefits of the use of the MD in patients with DM.
Research objectives
The main objective of this study was to examine the association between adherence to the MD,assessed by MD serving score(MDSS)and CV risk,assessed by AGEs skin levels,in patients with DM type II.Additionally,we examined the association between anthropometric characteristics,glycaemic control,and physical activity with AGEs levels among patients with DM type 2
Research methods
In this study,we employed the Croatian version of the 14-item MDSS questionnaire to assess adherence to the MD.On the other hand,in order to compare adherence to CV risk,we used skin autofluorescence-based AGE Reader that measures AGEs skin levels.
Research results
The present study demonstrated that patients with diabetes who have none or limited CV risk adhere more to the MD than patients who have either increased or definite CV risk.In addition,we showed that the subgroup of patients with diabetes with better glycaemic control adheres better to the MD than the subgroup of patients with worse glycaemic control.Altogether,these results are generally in line with the available data.It remains to be answered why adherence to MD is so low,despite being undoubtedly beneficial.
Research conclusions
By bringing additional data about the association of the MD with CV outcomes,this study addresses the need to implement novel strategies that will lead to better MD adherence in patients with diabetes.
Research perspectives
In future studies,the highlight should be placed further delineation off mechanisms by which MD exerts its favourable effects to establish the optimal dietary pattern.Furthermore,psychological studies could be important in this setting,as the main problem of MD is low adherence.Namely,psychological studies may give a deeper insight into non-adherence,thus facilitating the resolution of this issue.
ACKNOWLEDGEMENTS
The paper has been proofread by language professional Dalibora Behmen.
杂志排行

World Journal of Diabetes的其它文章
- Letter to editor ‘Gastroenteropathy in gastric cancer patients concurrent with diabetes mellitus’
- Comprehensive genetic screening reveals wide spectrum of genetic variants in monogenic forms of diabetes among Pakistani population
- Association between admission hemoglobin level and prognosis in patients with type 2 diabetes mellitus
- Factors influencing the effectiveness of using flash glucose monitoring on glycemic control for type 1 diabetes in Saudi Arabia
- p66Shc-mediated oxidative stress is involved in gestational diabetes mellitus
- Profilin-1 is involved in macroangiopathy induced by advanced glycation end products via vascular remodeling and inflammation